Download presentation
Presentation is loading. Please wait.

1
Professor Anne O’Hare ARICD 15 International Scientific Meeting Birmingham 2013 Current Perspectives on Child Development in the 21 st Century Cognitive conundrums coming our way?

2
Cognitive Conundrums Coming our Way? DEFINITIONS COGNITIVE: Relating to the mental processes involved in knowing, learning and understanding things As children grow older, their cognitive processes become sharper (Collins Cobuild Advanced Dictionary) CONUNDRUM: A problem that is difficult to solve
 CONUNDRUM: A problem that is difficult to solve.")
3
Cognitive Conundrums Coming our Way? Motor planning and executive function Language pragmatics Social cognition Motor planning and executive function Language pragmatics Social cognition

4
Acute Lymphoblastic Leukaemia Normal Blood Prevalence 2-3 per 10,000 35% of all childhood malignancies Second most common cause of death in 1-15 year olds

5
CNS involved in 5% at presentation Migration of leukaemic cells along perivascular and perineural tissues CNS relapse ‘inevitable’ without cranial prophylaxis Acute Lymphoblastic Leukaemia

6
Event Free Survival by Trial UKALL VIII

7
Impact of Cranial Irradiation Animal Model: Radiosensitivity of brain decreases with age Inhibition of differentiation of myelin Less myelin and immature fatty acid composition Children: Intellectual morbidity - ↓ performance IQ and short-term memory but verbal IQ maintained (Sizer 1980) Effect more marked under 3 years Arrests normal intellectual growth - gap widens over time (Janoun 1983)
 Effect more marked under 3 years Arrests normal intellectual growth - gap widens over time (Janoun 1983)")
8
Neurological Morbidity in ALL CSF biochemical studies: - Hypoxanthene and Xanthene - Cyclic adenosine 3’ 5’, monophosphate - 2’ 3’ -cyclic nucleotide 3’, phosphohydrolase Cranial CT and CSF Procoagulant activity 10 children Pre-treatment, induction and remission, all free of overt CNS involvement 33 children -5 year period, 25 controls undergoing LP to exclude CNS infection

9
Neurological Morbidity - Visual evoked responses and computerised psychometry Long term survivors – no CNS involvement, mainstream school 29 (20 girls, 9 boys) Matched controls – age, gender and socio-economic status O'Hare A E, Eden O B, Aitken K. Computerised psychometry screening in long-term survivors of childhood acute lymphoblastic leukaemia. Paediatric Haematology and Oncology,1988; 5: 197-208

10
Computerised Psychometry Visual spatial ability Symbol coding Visual perceptual analysis Visual spatial recognition memory Verbal recognition memory Abstract problem solving

11
Neurological Morbidity in ALL 1.CSF hypoxanthene raised at diagnosis and induction(p>0.001, p>0.005, p>0.001): ischaemic brain parenchyma from perivascular infiltration of the arachnoid vessels. 2.Cranial radiotherapy breaches the blood/brain barrier, myelin maturation disturbed during subsequent 2 years of treatment (p>0.001 procoagulant activity). 3.Cranial CT abnormal at diagnosis in 20% but only 6% at 4-5 years from treatment. 4.Subtle Neurological Morbidity: verbal recognition short term memory (p>0.02) abstract problem solving – Errors after positive feedback p>0.005 – Number of sorts p>0.005 – Overall performance p>0.01 O'Hare A,Clarke M, McInnes A, Eden O B. The latency of the visual evoked response as an index of myelin disturbance in children treated for acute lymphoblastic leukaemia. Clinical Electroencephalography, 1987; Vol 18 (2): 68-73). O'Hare A E, Eden O B, Simpson R McD, Donaldson A, Sainsbury C P Q. Cranial computerised tomography and CSF procoagulant activity in childhood acute lymphoblastic leukaemia. Haematology and Oncology 1987; Vol 5: 103-113.
. 3.Cranial CT abnormal at diagnosis in 20% but only 6% at 4-5 years from treatment. 4.Subtle Neurological Morbidity: verbal recognition short term memory (p>0.02) abstract problem solving – Errors after positive feedback p>0.005 – Number of sorts p>0.005 – Overall performance p>0.01 O Hare A,Clarke M, McInnes A, Eden O B. The latency of the visual evoked response as an index of myelin disturbance in children treated for acute lymphoblastic leukaemia. Clinical Electroencephalography, 1987; Vol 18 (2): 68-73). O Hare A E, Eden O B, Simpson R McD, Donaldson A, Sainsbury C P Q. Cranial computerised tomography and CSF procoagulant activity in childhood acute lymphoblastic leukaemia. Haematology and Oncology 1987; Vol 5:")
12
Development of an instrument to measure manual praxis Establish typical development of manual praxis – ability to gesture, use tools and sequence movement. Design standardised assessment of ‘hidden’ difficulty for children who struggle to learn everyday hand skills. Explain the role of ‘communication’ in the learning of manual praxis. O’Hare A E, Gorzkowska J, Elton R. Development of an instrument to measure manual praxis. Developmental Medicine and Child Neurology, 1999; 41: 597-607 O’Hare A E, Khans S, Hailey J. Delayed development of manual praxis in the presumed normal pre-term survivor. European Journal of Paediatric Neurology, 1999; 3(6): A137.
: A137..")
13
Development of an instrument to measure manual praxis – some interesting outcomes Aquired dyspraxia Mis-locations Omissions 1. Developmental dyspraxia Mis-sequence, spatial errors and few perseverations 2. Deprivation in childhood Learning to use tools Imitation of motor sequences No disadvantage Ability to imitate complex gesture and to undertake more ‘novel’ motor tasks to verbal instructions (p>0.01) Disadvantage
 Disadvantage.")
14
ASSOCIATED FEATURES OF ASPERGER’S SYNDROME AND THEIR RELATIONSHIP TO PARENTING STRESS Epstein T, Saltzman-Benaiah J, O’Hare A, Goll J, Tuck S. Child: Care, Health & Development, 2008; 34 (4) 503–511. Explore the relationship between some of the associated features of AS and levels of reported parenting stress in families of children affected Determine whether children with AS show impairment in executive function and heightened sensory sensitivity Determine whether parent report of their child’s demanding characteristics would be positively associated with their self-reported levels of parenting stress AIMS OF THE STUDY
 503–511. Explore the relationship between some of the associated features of AS and levels of reported parenting stress in families of children affected Determine whether children with AS show impairment in executive function and heightened sensory sensitivity Determine whether parent report of their child’s demanding characteristics would be positively associated with their self-reported levels of parenting stress AIMS OF THE STUDY.")
15
ASSOCIATED FEATURES OF ASPERGER’S SYNDROME AND THEIR RELATIONSHIP TO PARENTING STRESS 92.1% of mothers and 81.8% of fathers rated their children as having clinically elevated levels of executive dysfunction Correlation between mother’s and father’s overall score on the BRIEF approached significance (r=0.49; p>0.05) RESULTS – EXECUTIVE DYSFUNCTION
 RESULTS – EXECUTIVE DYSFUNCTION")
16
RELATIONSHIP BETWEEN MOTHERS’ (M) AND FATHERS’ (F) SCORES ON EACH VARIABLE AS WELL AS RELATIONSHIP BETWEEN CHILDREN'S DIFFICULTIES AND PARENTING STRESS VariablesCorrelation Confidence interval P-value *P < 0.01. Note that the total raw scores for each measure are used for the correlations. PSI/SF-M PSI/SF-F0.620.29 to 0.820.001458 * * BRIEF-M BRIEF-F0.670.34 to 0.860.0007974 * * SSP-M SSP-F0.730.35 to 0.910.001890 * * BRIEF-M PSI/SF-M0.600.34 to 0.770.000099 * * SSP-M PSI/SF-M−0.56−0.80 to −0.180.006478 * * BRIEF-F PSI/SF-F0.30−0.15 to 0.650.1793 SSP-F PSI/SF-F0.06−0.46 to 0.560.8195 *P < 0.01 Epstein T, Saltzman- Benaiah J, O’Hare A, Goll JC, Tuck S. Associated features of Asperger Syndrome and their relationship to parenting stress. Child: care, health and development 2008

17
ASPERGER’S SYNDROME AND PARENTING STRESS 75.7% of mothers and 75% of fathers reported clinically elevated stress levels No significant difference between mothers and fathers for overall levels of parenting stress or on any of the sub-scales Mothers’ and fathers’ scores were significantly correlated on total stress (r=0.62; p>0.01), parenting distress (r=0.71; p>0.01) and parent-child dysfunctional interaction (r=0.57; p>0.01) However mothers’ and fathers’ scores on the difficult child index were not significantly correlated RESULTS – STRESS LEVELS OF PARENTS OF A.S. CHILDREN

18
Vision and proprioception in ASD, DCD and typical development Does the use of vision and proprioception differentiate ASD and DCD? British Psychological Society, September 2013 Louisa Miller, Rob McIntosh, Anne O’Hare University of Edinburgh

19
Task 1: MABC results 71%67% 14% Fail: <15 th percentile on MABC Findings confirm movement deficits in majority of ASD ASD (n=31) DCD (n=9) TD (n=28) Percent
 DCD (n=9) TD (n=28) Percent")
20
Task 2: Visual-proprioceptive matching task

21
ASD ‘pure’ vs clumsy ASD/DCD ASD ‘pure’ (n=9) Clinical motor deficit (n=28) ASD with spared motor skills tend to weight vision less 0.8 0.4 Mean visual weighting t(35)=2.168, p=0.037, d=0.73 0
 Clinical motor deficit (n=28) ASD with spared motor skills tend to weight vision less Mean visual weighting t(35)=2.168, p=0.037, d=0.73 0")
22
Clinical assessment in ASD Second order mentalising abilities Pettigrew L M, O’Hare A E, Bremner L, Nash M, Happe F, Rutherford M. Journal of Autism and Developmental Disorder (in press). Second order mentalising abilities Pettigrew L M, O’Hare A E, Bremner L, Nash M, Happe F, Rutherford M. Journal of Autism and Developmental Disorder (in press). Disorders of sensory processing O’Hare A E, Adamson A, Graham C. British Journal of Occupational Therapy, 2006; Disorders of sensory processing O’Hare A E, Adamson A, Graham C. British Journal of Occupational Therapy, 2006; Identifying need and service requirements O’Hare A E, Quew R, Aitken K. Autism, 1998; Harrison M J, O’Hare A E, Campbell H, Adamson A, McNeillage J. Developmental Mental Medicine Child Neurology, 2004 Identifying need and service requirements O’Hare A E, Quew R, Aitken K. Autism, 1998; Harrison M J, O’Hare A E, Campbell H, Adamson A, McNeillage J. Developmental Mental Medicine Child Neurology, 2004 Executive function and parental stress Epstein T, Saltzman-Benaiah J, O’Hare A, Goll J, Tuck S. Child: Care, Health & Development, 2008. Executive function and parental stress Epstein T, Saltzman-Benaiah J, O’Hare A, Goll J, Tuck S. Child: Care, Health & Development, 2008. Prosody and pragmatic ability Peppé S, McCann J, Gibbon F, O'Hare A, Rutherford M. Journal Speech Language Hearing Research, 2007. McCann J, Peppe S, Gibbon F, O’Hare A, Rutherford M. International Journal of Language and Communication Disorders 2007. Peppe S, McCann J, Gibbon F, O’Hare A, Rutherford M. Journal of Pragmatics, 2006. Prosody and pragmatic ability Peppé S, McCann J, Gibbon F, O'Hare A, Rutherford M. Journal Speech Language Hearing Research, 2007. McCann J, Peppe S, Gibbon F, O’Hare A, Rutherford M. International Journal of Language and Communication Disorders 2007. Peppe S, McCann J, Gibbon F, O’Hare A, Rutherford M. Journal of Pragmatics, 2006.
. Second order mentalising abilities Pettigrew L M, O’Hare A E, Bremner L, Nash M, Happe F, Rutherford M. Journal of Autism and Developmental Disorder (in press). Disorders of sensory processing O’Hare A E, Adamson A, Graham C. British Journal of Occupational Therapy, 2006; Disorders of sensory processing O’Hare A E, Adamson A, Graham C. British Journal of Occupational Therapy, 2006; Identifying need and service requirements O’Hare A E, Quew R, Aitken K. Autism, 1998; Harrison M J, O’Hare A E, Campbell H, Adamson A, McNeillage J. Developmental Mental Medicine Child Neurology, 2004 Identifying need and service requirements O’Hare A E, Quew R, Aitken K. Autism, 1998; Harrison M J, O’Hare A E, Campbell H, Adamson A, McNeillage J. Developmental Mental Medicine Child Neurology, 2004 Executive function and parental stress Epstein T, Saltzman-Benaiah J, O’Hare A, Goll J, Tuck S. Child: Care, Health & Development, Executive function and parental stress Epstein T, Saltzman-Benaiah J, O’Hare A, Goll J, Tuck S. Child: Care, Health & Development, Prosody and pragmatic ability Peppé S, McCann J, Gibbon F, O Hare A, Rutherford M. Journal Speech Language Hearing Research, McCann J, Peppe S, Gibbon F, O’Hare A, Rutherford M. International Journal of Language and Communication Disorders Peppe S, McCann J, Gibbon F, O’Hare A, Rutherford M. Journal of Pragmatics, Prosody and pragmatic ability Peppé S, McCann J, Gibbon F, O Hare A, Rutherford M. Journal Speech Language Hearing Research, McCann J, Peppe S, Gibbon F, O’Hare A, Rutherford M. International Journal of Language and Communication Disorders Peppe S, McCann J, Gibbon F, O’Hare A, Rutherford M. Journal of Pragmatics,")
23
Prevalence of ASD The prevalence rate of ASD in children in the UK is 1 in 86 children (Baird et al 2006) The prevalence rate of ASD in adults in the UK is 1 in 100 adults (Brugha et al 2009) The USA Center for Disease Control (2012) reports a prevalence of 1 in 88 children in the USA Brugha et al (2012) report a prevalence of 1 in 90 adults in the UK
 The prevalence rate of ASD in adults in the UK is 1 in 100 adults (Brugha et al 2009) The USA Center for Disease Control (2012) reports a prevalence of 1 in 88 children in the USA Brugha et al (2012) report a prevalence of 1 in 90 adults in the UK")
24
24 4.11 Evidence statements: conditions with an increased prevalence of ASD ASD is observed more frequently in children with the following coexisting conditions than in the general population: Intellectual disability (prevalence of ASD: 8-27.9%) Fragile X (prevalence of ASD: 24–60%) Tuberous sclerosis (prevalence of ASD: 36–79%) Neonatal encephalopathy/epileptic/encephalopathy/infantile spasms (prevalence of ASD: 4–14%) Cerebral palsy (prevalence of ASD: 15%) Down‟s syndrome (prevalence of ASD: 6–15%) Muscular dystrophy (prevalence of ASD: 3–37%) Neurofibromatosis (prevalence of ASD: 4–8%). The quality of the evidence was very low in all studies. 4.11 Evidence statements: conditions with an increased prevalence of ASD ASD is observed more frequently in children with the following coexisting conditions than in the general population: Intellectual disability (prevalence of ASD: 8-27.9%) Fragile X (prevalence of ASD: 24–60%) Tuberous sclerosis (prevalence of ASD: 36–79%) Neonatal encephalopathy/epileptic/encephalopathy/infantile spasms (prevalence of ASD: 4–14%) Cerebral palsy (prevalence of ASD: 15%) Down‟s syndrome (prevalence of ASD: 6–15%) Muscular dystrophy (prevalence of ASD: 3–37%) Neurofibromatosis (prevalence of ASD: 4–8%). The quality of the evidence was very low in all studies.
 Fragile X (prevalence of ASD: 24–60%) Tuberous sclerosis (prevalence of ASD: 36–79%) Neonatal encephalopathy/epileptic/encephalopathy/infantile spasms (prevalence of ASD: 4–14%) Cerebral palsy (prevalence of ASD: 15%) Down‟s syndrome (prevalence of ASD: 6–15%) Muscular dystrophy (prevalence of ASD: 3–37%) Neurofibromatosis (prevalence of ASD: 4–8%). The quality of the evidence was very low in all studies..")
25
Child characteristics (n=258) Child characteristic% (n=) Gender Male: Female 84.16 (216:42) (ratio 4:1) Age at survey completion < 2 years 11 months 3 years – 5 years 11 months 6 – 11 years 2 (5) 31(81) 67 (172) ASD diagnosis Autism Asperger’s Syndrome Autism Spectrum Disorder PDD-NOS/ atypical autism 27 (70) 20 (52) 49 (127) 4 (9) Age at diagnosis < 2 years 11 months 3 years – 5 years 11 months 6 – 11 years 27 (70) 57 (146) 16 (42) Language level No meaningful speech Single words and phrases Sentences with good grammar Other( no details) 19 (50) 28 (70) 51 (132) 1 (5) Learning disability31 (81) Type of educational establishment attended Mainstream (school, nursery, unit attached) Specialist provision Home ed. 71 (179) 28 (70) 2 (4) Educational support *Individual Education Plan **Statement of Special Educational Needs 57 (150) 55 (144) * An Individual Education Plan (IEP) is a teaching and learning plan devised to identify the targets, provision and outcomes for a child identified with special educational needs. ** Statement of Special Educational Needs is a legal document issued by the Local Authority responsible for education, following an in- depth multidisciplinary assessment of the child’s needs. Adams S J, Burton N, Cutress A, Adamson A J, McColl E, O’Hare A E, Baird G, Le Couteur A. Parents’ and Child Health Professionals’ Attitudes Towards Dietary Interventions for Children with Autism Spectrum Disorders. JADD. Accepted August 2013
 28 (70) 2 (4) Educational support *Individual Education Plan **Statement of Special Educational Needs 57 (150) 55 (144) * An Individual Education Plan (IEP) is a teaching and learning plan devised to identify the targets, provision and outcomes for a child identified with special educational needs. ** Statement of Special Educational Needs is a legal document issued by the Local Authority responsible for education, following an in- depth multidisciplinary assessment of the child’s needs. Adams S J, Burton N, Cutress A, Adamson A J, McColl E, O’Hare A E, Baird G, Le Couteur A. Parents’ and Child Health Professionals’ Attitudes Towards Dietary Interventions for Children with Autism Spectrum Disorders. JADD. Accepted August")
26
em pathos : ‘feeling into’ Empathy is understanding a person’s subjective experience by sharing it vicariously but maintaining an observant stance Casebook MPS January 2011

27
Descriptions of empathy difficulties by a man affected with Asperger’s syndrome and diagnosed at the age of 50 The Guardian Weekend: 15 Jan 2011 “How can they interact with each other so unselfconsciously …” “I like people, I long to have friends and most of all to be in a relationship…” “The bottom line is, human beings were not meant to have to live like this. Social interaction is a basic human need”

28
How do we measure empathy in young children? Self report Observer report eg ASD screening instruments Direct measurement eg theory of mind assessments Indirect measurement eg perception of facial expression Response to intervention Neuroscience modalities eg electrophysiology, neuroimaging, genetics and animal models Self report Observer report eg ASD screening instruments Direct measurement eg theory of mind assessments Indirect measurement eg perception of facial expression Response to intervention Neuroscience modalities eg electrophysiology, neuroimaging, genetics and animal models

29
29 Total Social Communication Questionnaire (SCQ) scores for extremely preterm children with (n=11) and without (n=162) an autism spectrum disorder (ASD) diagnosis at 11 years of age Johnson S et al. Arch Dis Child 2011;96:73-77 Clinical diagnoses were assigned using the Development and Well Being Assessment (DAWBA) diagnostic interview. Horizontal bars indicate the mean SCQ score. Dashed lines indicate published SCQ cut-offs for positive screening.
 diagnostic interview. Horizontal bars indicate the mean SCQ score. Dashed lines indicate published SCQ cut-offs for positive screening..")
30
Performance of children with transposition of the great arteries (TGA) and of comparison individuals on theory of mind tasks (Calderon 2010) b Second- order false belief task (level 2) a First-order false belief task (level 1)
 and of comparison individuals on theory of mind tasks (Calderon 2010) b Second- order false belief task (level 2) a First-order false belief task (level 1)")
31
INDIRECT MEASUREMENT Reversible autism among congenitally blind children – a controlled follow-up study (Hobson & Lee 2010) Cognitive processing of social cues and in particular facial expression in high risk girls of a major depressive disorder (Joorman 2009)
 Cognitive processing of social cues and in particular facial expression in high risk girls of a major depressive disorder (Joorman 2009)")
32
Module 1 Preverbal/single words eg spontaneous initiation of joint attention. This rating codes the child’s attempts to draw another person’s attention to objects that neither of them is touching. Module 4 Fluent speech. Adolescent/adult. Empathy/comments on other’s emotions. The focus of this item is on the participants communication of his/her understanding and empathy for the feelings of other people, real or conveyed in stories or other tasks. ADOS

33
Was it true what Peter said? Why did he say it? White lie (Hat) One day Aunt Jane came to visit Peter. Now Peter loves his aunt very much, but today she is wearing a new hat; a new hat which Peter thinks is very ugly indeed. Peter thinks his aunt looks silly in it, and much nicer in her old hat. But when Aunt Jane asks Peter, “How do you like my new hat?” Peter says, “Oh, it’s very nice”. A Clinical Assessment Tool for Advanced Theory of Mind Performance in 5 to 12 Year Olds J Autism Dev Disord. 2009; 39(6): 916-928 Incorrect PHYSICAL It’s got a(u)nts on it It looked nice PSYCHOLOGICAL He liked the hat He wanted one He liked the old hat Physical State (2P) The lady asked him It looked horrible Partial Psychological State (2M) He didn’t want to get a row He didn’t want to get into trouble He didn’t like the hat He loved his aunt Psychological State Full and Accurate Answer (2M) To make his auntie feel that he likes it He didn’t want his auntie to think that he didn’t like it He didn’t want her to get sad/to make his auntie sad He didn’t want to hurt her feelings He didn’t want to upset his auntie So his auntie wouldn’t be offended He didn’t want to tell her he hated it He didn’t want to be rude He didn’t want to be nasty to her He wanted to make his auntie feel good He wanted to make his auntie happy
 One day Aunt Jane came to visit Peter. Now Peter loves his aunt very much, but today she is wearing a new hat; a new hat which Peter thinks is very ugly indeed. Peter thinks his aunt looks silly in it, and much nicer in her old hat. But when Aunt Jane asks Peter, How do you like my new hat Peter says, Oh, it’s very nice . A Clinical Assessment Tool for Advanced Theory of Mind Performance in 5 to 12 Year Olds J Autism Dev Disord. 2009; 39(6): Incorrect PHYSICAL It’s got a(u)nts on it It looked nice PSYCHOLOGICAL He liked the hat He wanted one He liked the old hat Physical State (2P) The lady asked him It looked horrible Partial Psychological State (2M) He didn’t want to get a row He didn’t want to get into trouble He didn’t like the hat He loved his aunt Psychological State Full and Accurate Answer (2M) To make his auntie feel that he likes it He didn’t want his auntie to think that he didn’t like it He didn’t want her to get sad/to make his auntie sad He didn’t want to hurt her feelings He didn’t want to upset his auntie So his auntie wouldn’t be offended He didn’t want to tell her he hated it He didn’t want to be rude He didn’t want to be nasty to her He wanted to make his auntie feel good He wanted to make his auntie happy.")
34
Story 5;0-5;116;0-6;117;0-7;118;0-8;119;0-9;1110;0- 10;11 11;0- 11;11 12;0- 12;11 P-value 1 Lie (Dentist)0.750.831.441.431.331.571.451.290.004 2 White Lie (Hat)0.501.001.311.401.831.711.731.86<0.001 3 Misunderstanding (Glove)0.000.430.691.001.171.571.231.43<0.001 4 Sarcasm (Picnic)0.000.090.62 0.780.901.141.71<0.001 5 Persuasion (Kittens)0.000.300.440.671.391.431.361.71<0.001 6 Contrary Emotion (Swings)0.670.480.750.521.561.190.951.430.002 7 Pretend (Bananas)1.000.611.501.051.561.521.591.86<0.001 8 Joke (Haircut)0.250.170.690.951.060.671.051.71<0.001 9 Figure of Speech (Cough)0.000.130.310.621.170.811.051.57<0.001 10 Double Bluff (Ping-Pong)0.000.480.560.620.671.140.550.860.006 11 Appearance/Reality (Santa Claus) 1.00 1.191.241.391.481.501.570.001 12 Forget (Doll)0.500.831.381.241.171.571.092.000.001 Total4.676.3510.8811.6515.0615.5714.6819.00<0.001 Mean scores for individual stories and the total according to age for Question 2M. P-value is for significance of association with age

35
Lower limit: Total = -13.76 + 1.96 x age Question 2M (psychological/mental state) : Age specific lower limits calculated by subtracting twice the residual standard deviation from the linear regression line
 : Age specific lower limits calculated by subtracting twice the residual standard deviation from the linear regression line")
36
Autism and Reactive Attachment Disorder: some research evidence Social relationship difficulties in autism and reactive attachment disorder; improving diagnostic validity through structured assessment. Davidson C, Minnis H, O'Hare A, MacTaggart F, Green J, Gillberg C, Young D Submitted to Journal of Child Psychology and Psychiatry

37
RAD “is a syndrome characterised by relative failure to develop committed intimate social relationships” Michael Rutter JCPP 2009 “…the clearest early sign [of autism], is when a child seems to lose interest in social interaction” Cathy Lord, NYU Child Study Centre Disorders of social interaction
![RAD is a syndrome characterised by relative failure to develop committed intimate social relationships Michael Rutter JCPP 2009 …the clearest early sign [of autism], is when a child seems to lose interest in social interaction Cathy Lord, NYU Child Study Centre Disorders of social interaction](http://images.slideplayer.com/9/2546104/slides/slide_37.jpg "RAD is a syndrome characterised by relative failure to develop committed intimate social relationships Michael Rutter JCPP 2009 …the clearest early sign [of autism], is when a child seems to lose interest in social interaction Cathy Lord, NYU Child Study Centre Disorders of social interaction")
38
Deficits in social communication and social interaction Restricted, repetitive behaviours, interests and activities Autism spectrum disorders

39
Highly heritable Usually life-long NOT related to abuse, neglect or “refrigerator parenting”! Autism spectrum disorders

40
Disinhibited type indiscriminate sociability with marked inability to exhibit appropriate selective attachments Reactive Attachment Disorder N.B. now called Disinhibited Social Engagement Disorder in DSM V

41
Inhibited type excessively inhibited, hypervigilant or highly ambivalent and contradictory responses Reactive Attachment Disorder

42
Emotional, behavioural and developmental features indicative of neglect or emotional abuse in preschool children: a systematic review (Naughton, JAMA Pediatric 2013) Key features in the child: Aggression (11 studies): exhibited as angry, disruptive behaviour, conduct problems, oppositional behaviour and low ego control Withdrawal or passivity (12 studies): including negative self esteem, anxious or avoidant behaviour, poor emotional knowledge and difficulties in interpreting emotional expressions in others Developmental delay (17 studies): delayed language, cognitive function and overall development quotient Poor peer interaction (5 studies): poor social interactions, unlikely to act to relieve distress in others Transition (6 studies): from ambivalent to avoidant insecure attachment pattern and from passive to increasingly aggressive behaviour and negative self-representation
 Key features in the child: Aggression (11 studies): exhibited as angry, disruptive behaviour, conduct problems, oppositional behaviour and low ego control Withdrawal or passivity (12 studies): including negative self esteem, anxious or avoidant behaviour, poor emotional knowledge and difficulties in interpreting emotional expressions in others Developmental delay (17 studies): delayed language, cognitive function and overall development quotient Poor peer interaction (5 studies): poor social interactions, unlikely to act to relieve distress in others Transition (6 studies): from ambivalent to avoidant insecure attachment pattern and from passive to increasingly aggressive behaviour and negative self-representation")
43
Emotional, behavioural and developmental features indicative of neglect or emotional abuse in preschool children: a systematic review (Naughton, JAMA Pediatric 2013) Children aged 20-30 months: Less positive social interaction Toddler spent the least time with adults and were avoidant even of their mothers Deficits of memory in neglected children
 Children aged months: Less positive social interaction Toddler spent the least time with adults and were avoidant even of their mothers Deficits of memory in neglected children")
44
Children aged 3-4 years: Specific delays in receptive language In free play and play initiated by a parent, neglected children demonstrated significantly more negative affect Ability to discriminate amongst emotions did not differ between groups of abused, emotionally neglected and physically neglected children with IQ as entered as a co-variate. Emotional, behavioural and developmental features indicative of neglect or emotional abuse in preschool children: a systematic review (Naughton, JAMA Pediatric 2013)
.")
45
Children aged 4-5 years: Delay in syntatic development of language Increasing social difficulties in interaction with other children Lower scores on cognitive functioning Exhibited disruptive behaviour that correlated with aggression Neglected children perceive other children as responding less often to relieve their distress Neglected children have difficulty recognising angry faces, preferentially selecting sad faces, more difficulty in discriminating among emotional expressions Neglected children are more likely to demonstrate under- controlled or ambivalent emotional response to simulated intra-adult aggression Emotional, behavioural and developmental features indicative of neglect or emotional abuse in preschool children: a systematic review (Naughton, JAMA Pediatric 2013)
")
46
Children aged 5-6 years: Low self esteem Insecure avoidant pattern of attachment Self-rating as angry and oppositional Rating others as sad, hurt or anxious Poor peer relationship Emotional, behavioural and developmental features indicative of neglect or emotional abuse in preschool children: a systematic review (Naughton, JAMA Pediatric 2013)
")
47
The Scottish Index of Multiple Deprivation (SIMD) quintile for our sample: Note: According to the Scottish Index of Multiple Deprivation, SIMD 1 is the most deprived and SIMD 5 is the least deprived.
 quintile for our sample: Note: According to the Scottish Index of Multiple Deprivation, SIMD 1 is the most deprived and SIMD 5 is the least deprived.")
48
Total LAC Population in Edinburgh 1998-2012 Citation from Stuart Osborough. Planning and performance, City of Edinburgh Council. Putting the looked after children population in context. 2012. The national picture for Looked After Children (LAC) populations 2011 LAC 1.5% 34% of LAC ‘at home’ Ratio kinship; residential is 10:1 59% under 12 years 30% in LAC for over 3 years
 populations 2011 LAC 1.5% 34% of LAC ‘at home’ Ratio kinship; residential is 10:1 59% under 12 years 30% in LAC for over 3 years.")
50
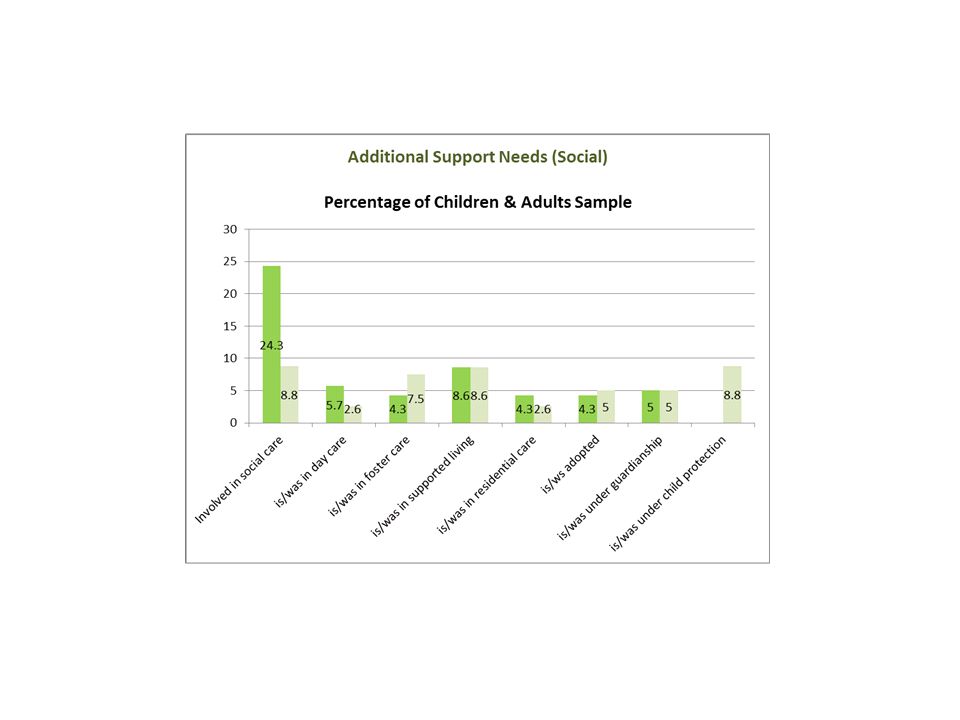
Additional Support Needs (Social) Reasons for being in day care Respite/befriending Share the care Reasons for being in foster care Neglect Physical abuse Behavioural difficulties Supervise parental visits Reasons for being in residential care Adolescent inpatient unit Homeless young person Reasons for under guardianship Parental abuse Parental substance misuse Under care of grandparents Reasons for being under child protection Domestic violence Inappropriate underage sexual activity Parental substance misuse Physical violence Parental psychotic illness
 Reasons for being in day care Respite/befriending Share the care Reasons for being in foster care Neglect Physical abuse Behavioural difficulties Supervise parental visits Reasons for being in residential care Adolescent inpatient unit Homeless young person Reasons for under guardianship Parental abuse Parental substance misuse Under care of grandparents Reasons for being under child protection Domestic violence Inappropriate underage sexual activity Parental substance misuse Physical violence Parental psychotic illness")
51
Identified risk factors for ASD Risk factor% Child cases% Adult cases% Overall Neurological disorder associated with ASD433 Intellectual disability213729 Speech delay554751 Speech regression936 Premature (born 35 weeks or below)1137 Additional support needs (education)842355 Involved in supported social care (adults only)n/a23n/a Family history of ASD14911 Family history of related condition441430 Parental history of psychosis/affective disorder34721
1137 Additional support needs (education) Involved in supported social care (adults only)n/a23n/a Family history of ASD14911 Family history of related condition Parental history of psychosis/affective disorder34721")
52
Identified risk factors for ASD Risk factor% Child cases% Adult cases% Overall Neurological disorder associated with ASD433 Intellectual disability213729 Speech delay554751 Speech regression936 Premature (born 35 weeks or below)1137 Additional support needs (education)842355 Involved in supported social care (adults only)n/a23n/a Family history of ASD14911 Family history of related condition441430 Parental history of psychosis/affective disorder34721
1137 Additional support needs (education) Involved in supported social care (adults only)n/a23n/a Family history of ASD14911 Family history of related condition Parental history of psychosis/affective disorder34721")
53
Identified risk factors for ASD Risk factor% Child cases% Adult cases% Overall Neurological disorder associated with ASD433 Intellectual disability213729 Speech delay554751 Speech regression936 Premature (born 35 weeks or below)1137 Additional support needs (education)842355 Involved in supported social care (adults only)n/a23n/a Family history of ASD14911 Family history of related condition441430 Parental history of psychosis/affective disorder34721
1137 Additional support needs (education) Involved in supported social care (adults only)n/a23n/a Family history of ASD14911 Family history of related condition Parental history of psychosis/affective disorder34721")
54
Antenatal risk factors : ASD Maternal folic acid supplements associated with reduced autism risk in the child (Suren et al, JAMA 2013 309 570-7) Schmidt 2013 Evidence for gestational nutrition influences on autism risk: renewed findings for iron (IMFAR abstract 2013) Offspring with a prenatal history of maternal depression were at higher risk of autism spectrum disorder, particularly autism without intellectual disability (Rai D, BMJ 2013 343) High maternally derived intrauterine androgen concentrations eg gestational diabetes, obstetric suboptimality may be a major environmental cause of autism (James, DMCN 2012)
 Schmidt 2013 Evidence for gestational nutrition influences on autism risk: renewed findings for iron (IMFAR abstract 2013) Offspring with a prenatal history of maternal depression were at higher risk of autism spectrum disorder, particularly autism without intellectual disability (Rai D, BMJ ) High maternally derived intrauterine androgen concentrations eg gestational diabetes, obstetric suboptimality may be a major environmental cause of autism (James, DMCN 2012)")
55
Adjusted odds ratios (95% confidence intervals) for relation between maternal depression and autism spectrum disorder overall and autism with and without intellectual disability in main and supplementary analyses (tables S3-S7). Rai D et al. BMJ 2013;346:bmj.f2059 ©2013 by British Medical Journal Publishing Group

56
Select findings after controlling for race, ethnicity, and mother’s education. Close H A et al. Pediatrics 2012;129:e305-e316 ©2012 by American Academy of Pediatrics

57
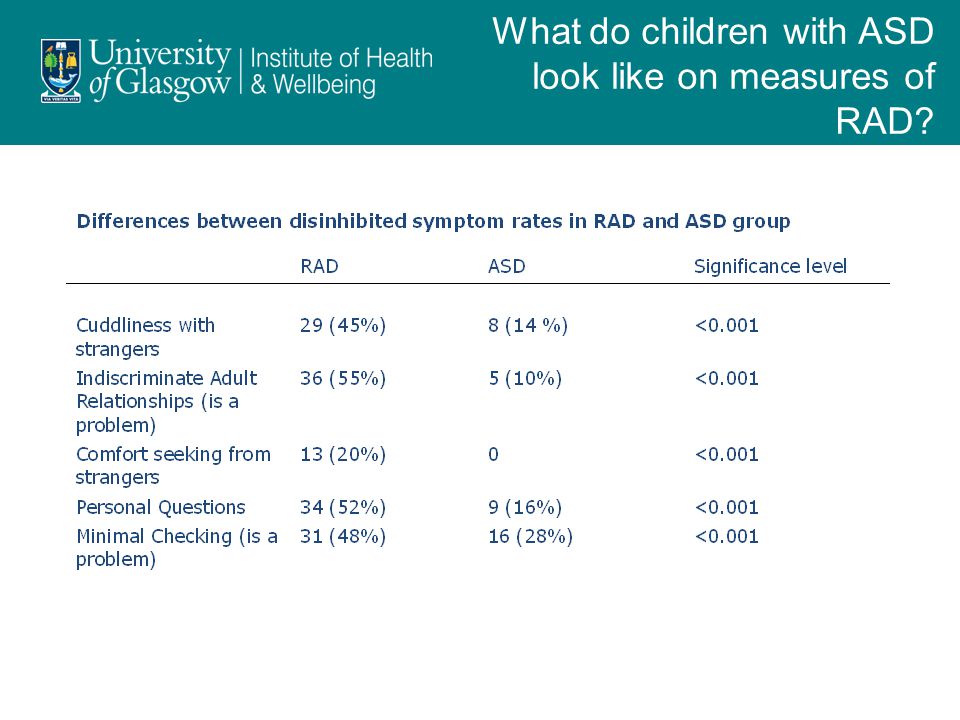
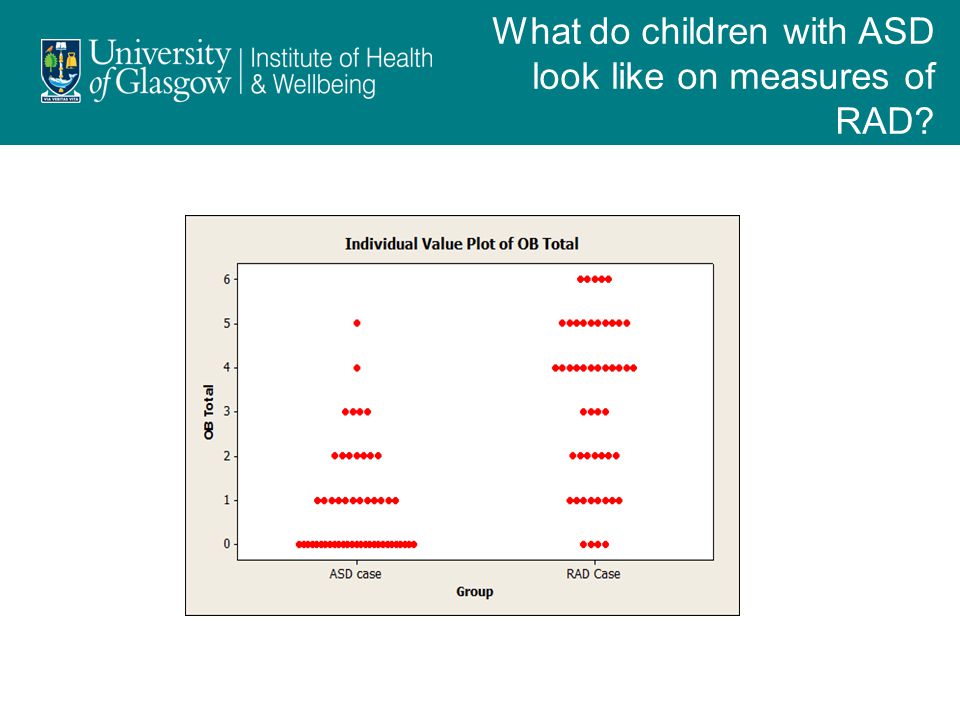
What do children with ASD look like on measures of RAD? Three groups (RAD, ASD, GP comparison) matched on age and verbal IQ 58 children with ASD recruited through Lothian and Lanarkshire 67 children with RAD from previous studies 61 typically developing children from previous studies Parent-report semi- structured interview on RAD symptoms Teacher questionnaire Videotaped observation for interaction with strangers Cognitive assessment
 matched on age and verbal IQ 58 children with ASD recruited through Lothian and Lanarkshire 67 children with RAD from previous studies 61 typically developing children from previous studies Parent-report semi- structured interview on RAD symptoms Teacher questionnaire Videotaped observation for interaction with strangers Cognitive assessment.")
58
Assessment of children with ASD: Parent-report semi-structured interview on RAD symptoms (CAPA-RAD) Parent-report semi-structured interview for other diagnoses (DAWBA) Teacher questionnaire (RPQ) Cognitive assessment in school with videotaped observation for interaction with strangers What do children with ASD look like on measures of RAD?
 Parent-report semi-structured interview for other diagnoses (DAWBA) Teacher questionnaire (RPQ) Cognitive assessment in school with videotaped observation for interaction with strangers What do children with ASD look like on measures of RAD")
63
Prosody and its relationship to language in school aged children with high functioning autism (HFA) Disordered expressive prosody characteristic of the speech in people with autism. “Not what you say but how you say it” - attitude and emotion, emphasis, conversational turns. Impacts on socialising and making friends. All children with HFA had a difficulty with prosody This correlates with receptive and expressive language Prosody (PEPS-C) and theory of mind impairment correlate Abnormal prosody persists over time Disordered expressive prosody characteristic of the speech in people with autism. “Not what you say but how you say it” - attitude and emotion, emphasis, conversational turns. Impacts on socialising and making friends. All children with HFA had a difficulty with prosody This correlates with receptive and expressive language Prosody (PEPS-C) and theory of mind impairment correlate Abnormal prosody persists over time McCann J, Peppe S, Gibbon F, O’Hare A, Rutherford M. International Journal of Language and Communication Disorders 2007; 42 (6) 682-702 Carroll L. Language development and its relationship to theory of mind in children with high functioning autism. 2007
 and theory of mind impairment correlate Abnormal prosody persists over time Disordered expressive prosody characteristic of the speech in people with autism. Not what you say but how you say it - attitude and emotion, emphasis, conversational turns. Impacts on socialising and making friends. All children with HFA had a difficulty with prosody This correlates with receptive and expressive language Prosody (PEPS-C) and theory of mind impairment correlate Abnormal prosody persists over time McCann J, Peppe S, Gibbon F, O’Hare A, Rutherford M. International Journal of Language and Communication Disorders 2007; 42 (6) Carroll L. Language development and its relationship to theory of mind in children with high functioning autism")
64
Receptive and expressive prosodic ability in children with high-functioning autism 0 10 20 30 40 50 60 70 80 90 100 Turnend Input Turnend Output Affect Input Affect Output Chunking Input Chunking Output Focus Input Focus Output Intonation Input Prosody Input Intonation Output Prosody Output Total PEPS-C Subtest % Correct HFA TD HFA TD p=0.001 p=0.003 p=0.0001 Peppé S, McCann J, Gibbon F, O'Hare A, Rutherford M. Receptive and expressive prosodic ability in children with high-functioning autism. Journal Speech Language Hearing Research, 2007; 50: 1015 - 1028

65
Accuracy of signs and symptoms to predict ASD Diagnostic ToolQuality assessmentSummary of Findings NumberDiagnostic accuracy StudiesDesignLimit- ations Incons- istency Indirect -ness QualityASDCon- trols Sensitivity (95%CI) Specificity (95%CI) PRE-SCHOOL CHILDREN (0-5 years) Failure to perform protodeclarative pointing, gaze monitoring and pretend play 1Con obs SomeNANoneVery low1023100 (100,100) Failure to perform protodeclarative pointing or protodeclarative pointing and pretend play 1Con obs SomeNANoneVery low1023100 (100,100) 70 (51,88) No pretend play 1Con obs SomeNANoneVery low101990 (71,100) 63 (41,85) No functional play 1Con obs SomeNANoneVery low101940 (10,70)84 (68,100) No facial concern in response to others distress 1Con obs SomeNANoneVery low1019100 (100,100) 68 (48,89) No attention to distress 1Con obs SomeNANoneVery low723921 (11,30)100 (100,100) Atypical use of object 1Con obs SomeNANoneVery low94778 (51,100) 77 (64,88) Lack of orienting to name 2Con obs SomeNANoneVery low257664 (43,82)88 (79,94) 65
 Specificity (95%CI) PRE-SCHOOL CHILDREN (0-5 years) Failure to perform protodeclarative pointing, gaze monitoring and pretend play 1Con obs SomeNANoneVery low (100,100) Failure to perform protodeclarative pointing or protodeclarative pointing and pretend play 1Con obs SomeNANoneVery low (100,100) 70 (51,88) No pretend play 1Con obs SomeNANoneVery low (71,100) 63 (41,85) No functional play 1Con obs SomeNANoneVery low (10,70)84 (68,100) No facial concern in response to others distress 1Con obs SomeNANoneVery low (100,100) 68 (48,89) No attention to distress 1Con obs SomeNANoneVery low (11,30)100 (100,100) Atypical use of object 1Con obs SomeNANoneVery low94778 (51,100) 77 (64,88) Lack of orienting to name 2Con obs SomeNANoneVery low (43,82)88 (79,94) 65")
66
Accuracy of signs and symptoms to predict ASD Diagnostic ToolQuality assessmentSummary of Findings NumberDiagnostic accuracy StudiesDesignLimit- ations Incons- istency Indirect -ness QualityASDCon- trols Sensitivity (95%CI) Specificity (95%CI) PRIMARY SCHOOL CHILDREN (6-11 years) No social play 1Con obs SeriousNANoneVery low203790 (77,100) 100 (100,100) Social isolation 1Con obs SeriousNANoneVery low203780 (62,98)70 (51,88) No respect for personal boundaries 1Con obs SeriousNANoneVery low203790 (28,72)63 (41,85) Socially inappropriate behaviour 1Con obs SeriousNANoneVery low203740 (19,61)84 (68,100) Unable to follow rules of a game 1Con obs SeriousNANoneVery low2037100 (100,100) 68 (48,89) Doesn’t respond to winning/losing a game 1Con obs SeriousNANoneVery low2037100 (100,100) Doesn’t initiate communication with peers 1Con obs SeriousNANoneVery low203780 (62,98)77 (64,88) Doesn’t sustain conversation with peers 1Con obs SeriousNANoneVery low2037100 (100,100) 88 (79,94) Gross motor inco-ordination 1Con obs SeriousNANoneVery low203765 (44,86)100 (100,100) No functional use of playground equipment 1Con obs SeriousNANoneVery low203750 (28,72)68 (52,83) 66
 Specificity (95%CI) PRIMARY SCHOOL CHILDREN (6-11 years) No social play 1Con obs SeriousNANoneVery low (77,100) 100 (100,100) Social isolation 1Con obs SeriousNANoneVery low (62,98)70 (51,88) No respect for personal boundaries 1Con obs SeriousNANoneVery low (28,72)63 (41,85) Socially inappropriate behaviour 1Con obs SeriousNANoneVery low (19,61)84 (68,100) Unable to follow rules of a game 1Con obs SeriousNANoneVery low (100,100) 68 (48,89) Doesn’t respond to winning/losing a game 1Con obs SeriousNANoneVery low (100,100) Doesn’t initiate communication with peers 1Con obs SeriousNANoneVery low (62,98)77 (64,88) Doesn’t sustain conversation with peers 1Con obs SeriousNANoneVery low (100,100) 88 (79,94) Gross motor inco-ordination 1Con obs SeriousNANoneVery low (44,86)100 (100,100) No functional use of playground equipment 1Con obs SeriousNANoneVery low (28,72)68 (52,83) 66")
67
Discrimination maps for the five different morphometric features in the left and right hemispheres Mundy (2003): PET scanning of children undergoing hemispherectomy showed that left frontal hemisphere was predictive of being able to initiate joint attention Herber (2006): the implicit matching of emotions subserved by the subcortical limbic system, explicit by the prefrontal cortex Ecker (2010): the neuroanatomy of autism is inherently difficulty to describe. A multi-parametric classification showed that the neuroanatomy of autism is truly multidimensional and affects multiple and most likely independent cortical features Lombardo (2010): atypical neural self representation in autism EEG in 5 year old girl with LKS Neuroscience modalities for measuring empathy
: atypical neural self representation in autism EEG in 5 year old girl with LKS Neuroscience modalities for measuring empathy.")
68
Using eye tracking as an early assessment of cognitive and social functioning in at-risk infant groups Karri Gillespie-Smith, Sue Fletcher-Watson, James Boardman, Ian Murray, Jane Norman, Anne O’Hare INTRODUCTION Recent studies have identified that eye-tracking gaze behaviours in at-risk infants are predictive of later ASD diagnosis. Edinburgh Perinatal Injury Research Group are interested in exploring these same effects in babies born premature. We have developed novel eye-tracking assessments measuring social and cognitive constructs in typically developing infants aged 6-12 months. We explore if we can create valid cognitive assessments for the 1 st year of life and relate these to clinically relevant variables.

69
METHODOLOGY PARTICIPANTS 30 typically developing infants (16 female; 14 male) Age = 182–366 days old PROCEDURE An eye-tracking battery was presented in three 8 minute blocks combining both novel visual tasks with previously tested tasks provided by British Autism Study of Infant Siblings (BASIS) Additional measures were also collected to investigate the relationship between eye tracking tasks, maternal mental health and stress
 Age = 182–366 days old PROCEDURE An eye-tracking battery was presented in three 8 minute blocks combining both novel visual tasks with previously tested tasks provided by British Autism Study of Infant Siblings (BASIS) Additional measures were also collected to investigate the relationship between eye tracking tasks, maternal mental health and stress")
70
METHODOLOGY A B C D E (A) Memory (B) Gap-Overlap Task (C) Face Scanning (D) Pop-Out Task (E) Social Scene Preference
 Memory (B) Gap-Overlap Task (C) Face Scanning (D) Pop-Out Task (E) Social Scene Preference")
71
Results: Validation of Tasks Significant age effect with performance in memory task which indicated older infants showed a novelty effect and younger infants showed a familiarity effect (p<0.05) Significant correlation between age and novelty effect during the memory task with 2000 (ms) gap only
 Significant correlation between age and novelty effect during the memory task with 2000 (ms) gap only")
72
Results: Links to Clinical Markers Significant correlation between hassle scores and standardized social scores Significant correlation between Daily Hassles Score and Social Score showing that mothers who view tasks as less stressful show more pro- social gaze (p<0.05)
")
73
DISCUSSION Infants show high social preferences. Social tasks correlated with each other (validating new cognitive tasks); standardized social score was created. Eye gaze data correlated with with clinical markers ie social standardized score and maternal stress/hassle; novel or familiarity preferences during memory task with age. Future research directions will involve developing more visual tasks and exploring eye-tracking further as a clinical marker in at-risk infant groups ie babies born pre-term.
; standardized social score was created. Eye gaze data correlated with with clinical markers ie social standardized score and maternal stress/hassle; novel or familiarity preferences during memory task with age. Future research directions will involve developing more visual tasks and exploring eye-tracking further as a clinical marker in at-risk infant groups ie babies born pre-term..")
74
Grateful thanks to … Prosody: Fiona Gibbon, Joanne McCann J, Sue Peppe, Leanne Carroll, Queen Margaret University, Edinburgh; Marion Rutherford, Royal Hospital for Sick Children, Edinburgh. Dyspraxia/Sensory: Amanda Adamson, Kirsty Forsyth, Jill Gorzkowska, Queen Margaret University; Rob Elton, University of Edinburgh. Mentalising Assessment: Lynne Bremner, Marysia Nash, Royal Hospital for Sick Children, Edinburgh. Prevalence ASD: Harry Campbell, Mark Harrison, Edinburgh University. Leukaemia and CNS: Tim Eden, Midge Clarke, Keith Brown, University of Edinburgh. Autism Achieve Alliance: Iain McClure, Karen McKenzie, University of Edinburgh; Kirsty Forsyth, Marion Rutherford, Ciara Catchpole, Tess Johnson, Ashley Peter, Deborah McCartney, Queen Margaret University ISS: Eye tracking: Karri Gillespie-Smith, Sue Fletcher- Watson, James Boardman, Ian Murray, Jane Norman, University of Edinburgh Autism & Reactive Attachment Disorder: Fiona Minnis, Claire Davidson, Glasgow University; Fiona MacTaggart, NHS Lothian. Prosody: Fiona Gibbon, Joanne McCann J, Sue Peppe, Leanne Carroll, Queen Margaret University, Edinburgh; Marion Rutherford, Royal Hospital for Sick Children, Edinburgh. Dyspraxia/Sensory: Amanda Adamson, Kirsty Forsyth, Jill Gorzkowska, Queen Margaret University; Rob Elton, University of Edinburgh. Mentalising Assessment: Lynne Bremner, Marysia Nash, Royal Hospital for Sick Children, Edinburgh. Prevalence ASD: Harry Campbell, Mark Harrison, Edinburgh University. Leukaemia and CNS: Tim Eden, Midge Clarke, Keith Brown, University of Edinburgh. Autism Achieve Alliance: Iain McClure, Karen McKenzie, University of Edinburgh; Kirsty Forsyth, Marion Rutherford, Ciara Catchpole, Tess Johnson, Ashley Peter, Deborah McCartney, Queen Margaret University ISS: Eye tracking: Karri Gillespie-Smith, Sue Fletcher- Watson, James Boardman, Ian Murray, Jane Norman, University of Edinburgh Autism & Reactive Attachment Disorder: Fiona Minnis, Claire Davidson, Glasgow University; Fiona MacTaggart, NHS Lothian. Funders: CSO Action Medical Research ESRC MRC Autism Speaks NHS QIS RHSC Friends Foundation (Autism Research and Development Fund) Scottish Executive Surestart Programme and Innovation Fund NHS HTA Research and Development Fund, Western Hospital, Toronto LUHTR&D Action Against Autism Wellcome ISSF Funders: CSO Action Medical Research ESRC MRC Autism Speaks NHS QIS RHSC Friends Foundation (Autism Research and Development Fund) Scottish Executive Surestart Programme and Innovation Fund NHS HTA Research and Development Fund, Western Hospital, Toronto LUHTR&D Action Against Autism Wellcome ISSF
 Scottish Executive Surestart Programme and Innovation Fund NHS HTA Research and Development Fund, Western Hospital, Toronto LUHTR&D Action Against Autism Wellcome ISSF Funders: CSO Action Medical Research ESRC MRC Autism Speaks NHS QIS RHSC Friends Foundation (Autism Research and Development Fund) Scottish Executive Surestart Programme and Innovation Fund NHS HTA Research and Development Fund, Western Hospital, Toronto LUHTR&D Action Against Autism Wellcome ISSF.")
Similar presentations



, Bsc. (Hons) OT>")

















