Download presentation
3
Non-colon › Esophagogastric › Pancreatic › Hepatobiliary

5
Phase III trial of everolimus in previously treated patients with advanced gastric cancer (AGC): GRANITE-1 Survival analysis according to disease subtype in AVAGAST : First-line capecitabine and cisplatin, plus bevacizumab or placebo, in patients with AGC
: GRANITE-1 Survival analysis according to disease subtype in AVAGAST : First-line capecitabine and cisplatin, plus bevacizumab or placebo, in patients with AGC")
7
Gastric cancer is aggressive and difficult to treat 5 year survival for advanced/metastatic is <5% Limited options upon failure of first-line chemotherapy

8
Key regulator of cell proliferation, growth, survival, metabolism, and angiogenesis Disregulated in 50-60% of gastric cancers Everolimus -Oral mTor inhibitor, efficacy in preclinical models of gastric cancer -Promising efficacy and tolerability in small phase II study (n=53) OS 10.1 mos, PFS 2.7mos
 OS 10.1 mos, PFS 2.7mos")
9
9 Confirmed advanced gastric cancer Progression after 1 or 2 lines of previous systemic chemotherapy Everolimus 10 mg PO daily + BSC* (n = 439) Placebo PO daily + BSC (n = 217) SCREEN Treatment until disease progression or intolerable toxicity Stratification by region: Asia vs rest of world Stratification by number of lines of previous systemic chemotherapy (1 vs 2) Safety follow-up: EOT + 28 d Survival follow-up: every 3 mo RANDOMIZE 2:1 (N = 656) BSC, best supportive care; EOT, end of treatment; PO, orally. ClinicalTrials.gov identifier: NCT00879333. Van Cutsem E et al. GI Cancer Symposium 2012 (Abstr LBA3).
..")
10
Inclusion criteria › Age >18yrs › Confirmed gastric adenocarcinoma › Documented progression after 1-2 lines of chemo › ECOG ≤2 › Adequate bone marrow, renal, and hepatic function Exclusion criteria › >2 lines of systemic treatment for advanced disease › Anticancer treatment within 3 wks or major surgery within 2 weeks of study randomization › Chronic treatment with steriods or immunosuppressive agents › Enteral feeding › CNS metastases › Any severe/uncontrolled medical condition

11
Primary: › OS Secondary: › PFS › ORR › AEs › Time to definitive deterioration of ECOG › Time to 5% deterioration in global health/QOL Exploratory: › Correlation between biomarkers and clinical endpoints

12
North America › Canada › United States Central and South America › Argentina › Colombia › Mexico › Peru East Asia › China › Hong Kong › Japan › Korea › Taiwan Other Asia and Pacific Region › Australia › New Zealand › Thailand Europe and Middle East › Belgium › France › Germany › Israel › Italy › Netherlands › Russia › Spain › United Kingdom

13
Everolimus + BSC (n=439)Placebo + BSC (n=217) Age, median (range) 62.0 (20.0-86.0)62.0 (26.0-88.0) Age <65 yrs, n (%) 260 (59.2)129 (59.4) Male, n (%) 322 (73.3)161 (74.2) Race, n (%) Caucasian166 (37.8)75 (34.6) Age, yrs (median) 251 (57.2) 126 (58.1) Other22 (5.0)16 (7.4) Region, n (%) Asia243 (55.4)120 (55.3) Rest of world196 (44.6)97 (44.7) ECOG, n (%) 0144 (32.8)70 (32.3) 1269 (61.3)120 (55.3) 225 (5.7)27 (12.4)
Placebo + BSC (n=217) Age, median (range) 62.0 ( )62.0 ( ) Age <65 yrs, n (%) 260 (59.2)129 (59.4) Male, n (%) 322 (73.3)161 (74.2) Race, n (%) Caucasian166 (37.8)75 (34.6) Age, yrs (median) 251 (57.2) 126 (58.1) Other22 (5.0)16 (7.4) Region, n (%) Asia243 (55.4)120 (55.3) Rest of world196 (44.6)97 (44.7) ECOG, n (%) 0144 (32.8)70 (32.3) 1269 (61.3)120 (55.3) 225 (5.7)27 (12.4)")
14
Everolimus + BSC (n=439)Placebo + BSC (n=217) Anatomical site, n (%) Proximal162 (36.9)94 (43.3) Distal276 (62.9)123 (56.7) GEJ involvement, n (%) 118 (26.9)69 (31.8) Lauren classification,n (%) AdenoCa, diffuse AdenoCa, intest’l AdenoCa, mixed AdenoCa, NOS Other 93 (21.2) 82 (18.7) 29 (6.6) 105 (23.9) 129 (29.4) 37 (17.1) 50 (23.0) 18 (8.3) 45 (20.7) 67 (30.9) Gastrectomy, n(%) Partial Total 126 (28.7) 97 (22.1) 60 (27.6) 46 (21.2) Previous lines chemo, n (%) 1 2 210 (47.8) 229 (52.2) 103 (47.5) 114 (52.5)
Placebo + BSC (n=217) Anatomical site, n (%) Proximal162 (36.9)94 (43.3) Distal276 (62.9)123 (56.7) GEJ involvement, n (%) 118 (26.9)69 (31.8) Lauren classification,n (%) AdenoCa, diffuse AdenoCa, intest’l AdenoCa, mixed AdenoCa, NOS Other 93 (21.2) 82 (18.7) 29 (6.6) 105 (23.9) 129 (29.4) 37 (17.1) 50 (23.0) 18 (8.3) 45 (20.7) 67 (30.9) Gastrectomy, n(%) Partial Total 126 (28.7) 97 (22.1) 60 (27.6) 46 (21.2) Previous lines chemo, n (%) (47.8) 229 (52.2) 103 (47.5) 114 (52.5)")
15
15 CI, confidence interval. Van Cutsem E et al. GI Cancer Symposium 2012 (Abstr LBA3).
.")
16
16 ROW, rest of world. Van Cutsem E et al. GI Cancer Symposium 2012 (Abstr LBA3). Prior chemotherapy Region Cross-class. of strata Hazard Ratio (95% CI) 0.80.6 Everolimus 10 mg/d Placebo In favor of 1.01.21.4 All (N = 656)0.90 (0.75-1.08) 2 (n = 343)0.90 (0.70-1.15) Asia (n = 363)0.96 (0.75-1.23) ROW (n = 293)0.85 (0.65-1.10) 1 prior chemo & ROW (n = 167)0.91 (0.64-1.31) 2 prior chemo & ROW (n = 126)0.74 (0.50-1.09) 1 (n = 313)0.94 (0.73-1.23) 0.98 (0.71-1.35)2 prior chemo & Asia (n = 217) 0.94 (0.63-1.39)1 prior chemo & Asia (n = 146)
 Everolimus 10 mg/d Placebo In favor of All (N = 656)0.90 ( ) 2 (n = 343)0.90 ( ) Asia (n = 363)0.96 ( ) ROW (n = 293)0.85 ( ) 1 prior chemo & ROW (n = 167)0.91 ( ) 2 prior chemo & ROW (n = 126)0.74 ( ) 1 (n = 313)0.94 ( ) 0.98 ( )2 prior chemo & Asia (n = 217) 0.94 ( )1 prior chemo & Asia (n = 146).")
17
17 Van Cutsem E et al. GI Cancer Symposium 2012 (Abstr LBA3).
.")
18
Everolimus + BSC (n=379) Placebo + BSC (n=191) Best overall response, n (%) CR1 (0.3)0 PR16 (4.1)4 (2.1) SD147 (38.8)38 (19.9) PD157 (41.4)119 (62.3) unknown58 (15.3)30 (15.7) ORR (CR+PR), n (%)17 ( 4.5 )4 ( 2.1 ) DCR (CR+PR+SD), n (%)164 ( 43.3 )42 ( 22.0 )
 Placebo + BSC (n=191) Best overall response, n (%) CR1 (0.3)0 PR16 (4.1)4 (2.1) SD147 (38.8)38 (19.9) PD157 (41.4)119 (62.3) unknown58 (15.3)30 (15.7) ORR (CR+PR), n (%)17 ( 4.5 )4 ( 2.1 ) DCR (CR+PR+SD), n (%)164 ( 43.3 )42 ( 22.0 )")
19
19 Best % change from baseline (measurable lesions) 160% 140% 120% 100% 80% 60% 40% 20% 0% –20% –40% –60% –80% –100% 160% 140% 120% 100% 80% 60% 40% 20% 0% –20% –40% –60% –80% –100% Everolimus 10 mg/day (n = 304)Placebo (n = 154) Van Cutsem E et al. GI Cancer Symposium 2012 (Abstr LBA3).
..")
20
Everolimus + BSC (n=437) Placebo + BSC (n=215) Any AE, n(%) 433 (99.1)208 (96.7) Any grade 3/4 AE, n(%) 310 (70.9)115 (53.5) Any serious AE, n(%) 207 (47.4)89 (41.4) AE leading to discontinuation,n(%) 94 (21.5)34 (15.8) AE requiring dose interruption/reduction, n(%) 242 (55.4)46 (21.4) AE requiring additional therapy,n %) 395 (90.4)174 (80.9) All deaths, n(%) 352 (80.5)179 (83.3) On-treatment deaths, n(%) 88 (20.1)49 (22.8)
 Placebo + BSC (n=215) Any AE, n(%) 433 (99.1)208 (96.7) Any grade 3/4 AE, n(%) 310 (70.9)115 (53.5) Any serious AE, n(%) 207 (47.4)89 (41.4) AE leading to discontinuation,n(%) 94 (21.5)34 (15.8) AE requiring dose interruption/reduction, n(%) 242 (55.4)46 (21.4) AE requiring additional therapy,n %) 395 (90.4)174 (80.9) All deaths, n(%) 352 (80.5)179 (83.3) On-treatment deaths, n(%) 88 (20.1)49 (22.8)")
21
Everolimus + BSC (n=437)Placebo + BSC(n=215) Adverse Event, n(%) All gradesGrades 3/4All gradesGrades 3/4 Nonheme Decreased Appetite 208 (47.6) 48 ( 11.0 ) 78 (36.3)12 (5.6) Stomatitis 174 (39.8)20 (4.6)23 (10.7)0 Fatigue 150 (34.3)34 (7.8)65 (30.2)11 (5.1) Nausea 132 (30.2)16 (3.7)69 (32.1)8 (3.7) Diarrhea 115 (26.3)15 (3.4)33 (15.3)2 (0.9) Heme Anemia 114 (26.1) 70 ( 16.0 ) 42 (19.5)27 (12.6) Thrombocytopenia 80 (18.3)22 (5.0)5 (2.3)3 (1.4) Neutropenia 47 (10.8)17 (3.9)6 (2.8)1 (0.5) Abn biochem Hypokalemia 52 (11.9)26 (5.9)9 (4.2)2 (0.9) Increased ALP 34 (7.8)20 (3.6)6 (3.8)3 (1.4) Increased AST 34 (7.8)14 (3.2)8 (3.7)2 (0.9)
Placebo + BSC(n=215) Adverse Event, n(%) All gradesGrades 3/4All gradesGrades 3/4 Nonheme Decreased Appetite 208 (47.6) 48 ( 11.0 ) 78 (36.3)12 (5.6) Stomatitis 174 (39.8)20 (4.6)23 (10.7)0 Fatigue 150 (34.3)34 (7.8)65 (30.2)11 (5.1) Nausea 132 (30.2)16 (3.7)69 (32.1)8 (3.7) Diarrhea 115 (26.3)15 (3.4)33 (15.3)2 (0.9) Heme Anemia 114 (26.1) 70 ( 16.0 ) 42 (19.5)27 (12.6) Thrombocytopenia 80 (18.3)22 (5.0)5 (2.3)3 (1.4) Neutropenia 47 (10.8)17 (3.9)6 (2.8)1 (0.5) Abn biochem Hypokalemia 52 (11.9)26 (5.9)9 (4.2)2 (0.9) Increased ALP 34 (7.8)20 (3.6)6 (3.8)3 (1.4) Increased AST 34 (7.8)14 (3.2)8 (3.7)2 (0.9)")
22
Everolimus monotherapy did not significantly improve OS in patients with AGC as second/third line therapy Everolimus did reduce the risk of progression, compared with BSC › Median PFS 1.41 1.68, HR 0.66, p<0.001 Disease control 22% 43%

23
Safety profile was similar to that observed with everolimus in other malignancies Disease control signal worth further study? › Biomarkers to identify those who benefit

25
Clinical/epidemiological data suggest there are three subtypes: › Type 1: proximal, non-diffuse › Type 2: diffuse › Type 3: distal, non-diffuse Each subtype has different gene expression profile

26
SUBTYPEPREVALENT RISK FACTORS Proximal (Type 1) Environmental Clinical Genetic Tobacco use Alcohol Obesity GERD None specifically identified Diffuse (Type 2) Environmental Clinical Genetic None specifically identified H. Pylori infection CDH-1 mutation Family history (non CDH-1 mutant) Distal (Type 3) Environmental Clinical Genetic High dietary salt Eating fruits/vegetables* Tobacco Age (peak at 50-70) H. Pylori infection Use of NSAIDs/ASA* Immune regulatory SNPs
 Distal (Type 3) Environmental Clinical Genetic High dietary salt Eating fruits/vegetables* Tobacco Age (peak at 50-70) H. Pylori infection Use of NSAIDs/ASA* Immune regulatory SNPs.")
27
Global, randomized, phase III study Bevacizumab + chemo vs. placebo + chemo (first-line treatment for AGC) Primary endpoint: OS › Was not met (12 mos vs 10 mos, p=0.1002) Regional efficacy differences were noted › Patients from Europe/Americas did better
 Primary endpoint: OS › Was not met (12 mos vs 10 mos, p=0.1002) Regional efficacy differences were noted › Patients from Europe/Americas did better.")
28
Several analyses have been performed to better understand regional differences Analysis has revealed: › It is the ‘high risk’ pts from Europe/Americas that derive more benefit from bevacizumab

29
To examine the OS data according to gastric cancer subtype and region To identify if disease subtype was: › Prognostic › Predictive of bevacizumab benefit (Europe/Americas) To examine the distribution of angiogenic biomarkers across subtypes › Do gastric cancer subtypes have different biomarker expression profiles?
 To examine the distribution of angiogenic biomarkers across subtypes › Do gastric cancer subtypes have different biomarker expression profiles")
30
Placebo + capecitabine + cisplatin (n=387) Bevacizumab + capecitabine + cisplatin (n=387) Locally advanced or metastatic gastric cancer (n=774) R Endpoints Primary : Overall survival Secondary : Progression-free survival Exploratory : Changes in candidate biomarkers: pVEGFA, NRP-1, VEGFA, VEGFR1, VEGFR2 5-FU allowed if capecitabine contraindicated Maximum of 6 cycles of cisplatin Capecitabine and bevacizumab / placebo until PD Stratification factors: 1. Geographic region 2. Fluoropyrimidine backbone 3. Disease status

31
All patients (n=733) Asia-Pacific (n=355) Europe/Americas (n=378)
 Asia-Pacific (n=355) Europe/Americas (n=378)")
32
There appears to be differences in biomarker distribution amongst gastric cancer subtypes SubtypepVEGF-A (median) NRP-1 (median) VEGF-A (median) VEGFR1 (median) VEGFR2 (median) Total 11190 130100 Proximal 104.2100 110100 Diffuse 102.88078.5140100 Distal 134.5100 120100
 NRP-1 (median) VEGF-A (median) VEGFR1 (median) VEGFR2 (median) Total Proximal Diffuse Distal")
33
30 91 72 28 72 62 22 47 18 28 35 14 22 21 7 13 12 354354 110110 000000 No. at risk Type 1 Type 2 Type 3 Proximal Diffuse Distal Study month 100 90 80 60 50 40 30 20 10 0 0 3 6 9 12 15 18 21 24 Survival rate (%)
.")
34
Disease subtype RegionPts/arm (placebo/bev Median OS, mo (placebo/bev) OS Hazard ratio (95% CI) Proximal All Asia-Pacific Eur/Americas 35/35 5/9 30/26 11.3/10.4 11.3/NR 12.8/10.4 1.05(0.59,1.89) 0.39(0.10,1.58) 1.50(0.77,2.93) Diffuse All Asia-Pacific Eur/Americas 206/176 115/100 91/76 9.3/11.9 11.0/13.5 6.5/9.9 0.83(0.65,1.06) 0.96(0.69,0.34) 0.68(0.48,0.97) Distal All Asia-Pacific Eur/Americas 126/155 54/72 72/83 11.1/13.3 15.5/13.9 9.0/11.7 0.87(0.64,1.16) 1.10(0.70,1.73) 0.72(0.48,1.07)
 OS Hazard ratio (95% CI) Proximal All Asia-Pacific Eur/Americas 35/35 5/9 30/ / /NR 12.8/ (0.59,1.89) 0.39(0.10,1.58) 1.50(0.77,2.93) Diffuse All Asia-Pacific Eur/Americas 206/ /100 91/76 9.3/ / / (0.65,1.06) 0.96(0.69,0.34) 0.68(0.48,0.97) Distal All Asia-Pacific Eur/Americas 126/155 54/72 72/ / / / (0.64,1.16) 1.10(0.70,1.73) 0.72(0.48,1.07)")
35
SubtypeRegionPts/arm (Pla/Bev) Median OS, mo (Pla/Bev) Hazard ratio (95% CI) Proximal All Europe/Americas 35/35 30/26 11.3/10.4 12.8/10.4 1.05 1.50 Diffuse All Europe/Americas 206/176 91/76 9.3/11.9 6.5/9.9 0.83 0.68 Distal All Europe/Americas 126/155 72/83 11.1/13.3 9.0/11.7 0.87 0.72 Diffuse/distal Europe/Americas163/1597.3/11.4 0.67
 Median OS, mo (Pla/Bev) Hazard ratio (95% CI) Proximal All Europe/Americas 35/35 30/ / / Diffuse All Europe/Americas 206/176 91/76 9.3/ / Distal All Europe/Americas 126/155 72/ / / Diffuse/distal Europe/Americas163/1597.3/")
36
Population: Europe/Americas with type 2/3 disease Hazard ratio 0.67 (95% CI 0.52–0.88) Study month 100 90 80 70 60 50 40 30 20 10 0 163 159 134 144 94 119 63 94 43 63 25 28 9 10 1313 0000 No. at risk Pla + chemo Bev + chemo 0 3 6 9 12 15 18 21 24 Pla + chemo Bev + chemo Survival rate (%)
.")
37
BiomarkerSubgroupNHazard ratio for OS (95% CI) P value pVEGF-A Low High 357 355 1.01 (0.77-1.31) 0.72 (0.57-0.93) 0.07 NRP-1Low High 350 329 0.75 (0.58-0.97) 1.07 (0.81-1.40) 0.06
 P value pVEGF-A Low High ( ) 0.72 ( ) 0.07 NRP-1Low High ( ) 1.07 ( ) 0.06")
38
SubtypeNRP-1 (n=679), median pVEGF-A (n=712), median Total 90111 Proximal 100104.2 Diffuse80 102.8 Distal 100 134.5
, median pVEGF-A (n=712), median Total Proximal Diffuse Distal")
39
Proximal (type 1) gastric cancer appears to have the ‘worst’ profile for bevacizumab › High NRP-1, low pVEGF-A Diffuse (type 2) and distal (type 3) appear to have at least one biomarker that may support benefit to an antioangiogenic strategy › Diffuse (type 2) low NRP-1 › Distal (type 3) high pVEGF-A
 gastric cancer appears to have the ‘worst’ profile for bevacizumab › High NRP-1, low pVEGF-A Diffuse (type 2) and distal (type 3) appear to have at least one biomarker that may support benefit to an antioangiogenic strategy › Diffuse (type 2) low NRP-1 › Distal (type 3) high pVEGF-A")
40
Gastric cancer is more than one disease! Gastric cancer subtypes have different prognoses › In all regions, diffuse (type 2) did worse The addition of bev to chemo appears to improve outcomes in pts from Europe/Americas with diffuse and distal disease Biomarkers NRP-1 and plasma pVEGF-A provide a rationale for subtype-specific outcomes with bevacizumab › Additional evaluation warranted
 did worse The addition of bev to chemo appears to improve outcomes in pts from Europe/Americas with diffuse and distal disease Biomarkers NRP-1 and plasma pVEGF-A provide a rationale for subtype-specific outcomes with bevacizumab › Additional evaluation warranted.")
44
Represents a field defect of ductal instability Main and branch duct IPMN carry a risk of malignancy in target cyst itself › 57-95% for MD-IPMN › 6-46% for BD-IPMN Risk of developing malignancy in region other than target cyst is poorly defined

45
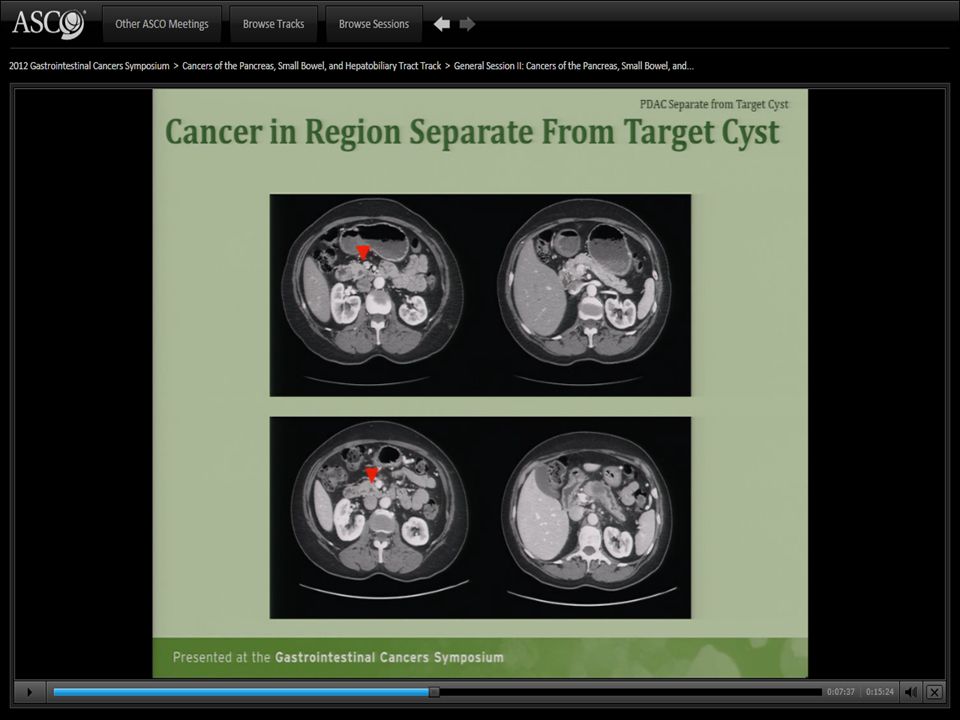
Identify patients with IPMN who underwent resection Define: › Pathologic characteristics of target cyst › Risk of developing a PDAC in a region separate from the target cyst

46
Retrospective review Pts evaluated at MSKCC from Feb ‘89-Aug ‘10: › Radiologic confirmation of target cyst › Pathologic confirmation of IPMN and/or cyst fluid CEA level ≥200ng/mL › Time from IPMN diagnosis to resection ≥6 mos

48
Variable Number (%) 97 (100%) Gender, N (%) Female54 (55) Resection type, N (%) Pancreaticoduodenectomy Distal pancreatectomy Enucleation Total pancreatectomy Central pancreatectomy 53(55) 32(33) 6(6) 4(4) 2(2) Time, diagnosis to resection, median mos 15.5 Time, first MSKCC visit to resection, median mos 2.1 Age at diagnosis, yrs, median 69
 97 (100%) Gender, N (%) Female54 (55) Resection type, N (%) Pancreaticoduodenectomy Distal pancreatectomy Enucleation Total pancreatectomy Central pancreatectomy 53(55) 32(33) 6(6) 4(4) 2(2) Time, diagnosis to resection, median mos 15.5 Time, first MSKCC visit to resection, median mos 2.1 Age at diagnosis, yrs, median 69")
49
Identify patients with IPMN who underwent resection › Define pathologic characteristics of target cyst › Define the risk of developing a PDAC in a region separate from the target cyst

50
VariableResection >6 mos adenoma/borderline i.e. LOW RISK N=57 (59%) Resection >6mos HGD/invasive i.e. HIGH RISK N=40 (41%) P value IPMN location, n(%) Head Body/tail Head/body Diffuse 32(56) 23(40) 2(4) 0(0) 25(62) 14(35) 0(0) 1(2) 0.70 IPMN size, cm, median 2.130.01 IPMN subtype, n(%) Main Branch Mixed 10(18) 39(68) 8(14) 17(42) 11(27) 12(30) <0.001
 Resection >6mos HGD/invasive i.e. HIGH RISK N=40 (41%) P value IPMN location, n(%) Head Body/tail Head/body Diffuse 32(56) 23(40) 2(4) 0(0) 25(62) 14(35) 0(0) 1(2) 0.70 IPMN size, cm, median IPMN subtype, n(%) Main Branch Mixed 10(18) 39(68) 8(14) 17(42) 11(27) 12(30) <")
51
VariableResection >6 mos adenoma/borderline i.e. LOW RISK (N=57) Resection >6mos HGD/invasive i.e. HIGH RISK (N=40) P value Degree of dysplasia, N(%) Adenoma Borderline High gr dysplasia Invasive 16(28) 41(72) 0(0) 22(55) 18 (45) N/A Subtype, N(%) Tubular Colloid Mixed Other Uknown N/A 11(61) 4(22) 2(11) 0(0) 1(6) N/A
 P value Degree of dysplasia, N(%) Adenoma Borderline High gr dysplasia Invasive 16(28) 41(72) 0(0) 22(55) 18 (45) N/A Subtype, N(%) Tubular Colloid Mixed Other Uknown N/A 11(61) 4(22) 2(11) 0(0) 1(6) N/A.")
53
Identify patients with IPMN who underwent resection › Define pathologic characteristics of target cyst › Define the risk of developing a PDAC in a region separate from the target cyst

56
Of 158 patients ≥6 mos after diagnosis › 97 came to resection › Invasive carcinoma in 18 pts, representing 11% of those being followed 19% of those who came to resection › Of those with invasive carcinoma, 5 pts developed PDAC in region other than target cyst, representing 3.2% of those being followed 5.2% of those who came to resection

57
Surveillance strategies for patients with IPMN should consider risk of malignancy to not only the region of target cyst, but to entire gland Patients with invasive components in their target cyst are at risk for PDAC in a separate region, and may need closer surveillance More studies needed to further define this risk

60
TACE is std of care for intermediate stage hcc TACE with DEBDOX has shown advantages in efficacy and safety over conventional TACE › Reduces peak concentration and total systemic exposure to doxorubicin fewer AEs Several phase II trials suggest a synergistic effect between sorafenib and TACE › TACE in these trials was heterogenous › Large global trial needed to test the combo of TACE and Sorafenib with a controlled TACE regimen

61
Objective › To evaluate the efficacy and safety of Sorafenib in combination with TACE using DEBDOX in patients with intermediate-stage hcc Design › Randomized, double-blind, placebo-controlled phase II 85 centres, 13 countries Efficacy assessments performed on ITT population Safety assessments performed on all pts that received at least one dose of study drug

62
Stratification factors › Geographic region Europe North America Asia Pacific › AFP <400 vs ≥400

63
Sorafenib 400mg bid Matching Placebo Inclusion Criteria Unresectable, multinodular, asymptomatic HCC Child-Pugh A without ascites or encephalopathy ECOG PS of 0 Exclusion Criteria Diffuse HCC, vascular invasion, extrahepatic spread (VI/EHS) Contraindication to hepatic embolization procedures Planned liver transplantation Previous local therapy to target lesion Prior TACE, prior systemic therapy RANDOMIZERANDOMIZE Primary Endpoint Time to progression (by central review) Secondary Endpoints Overall survival Time to VI/EHS Time to untreatable progression Safety 135791113151719 TACE (optional) Imaging Cycle no (=4 weeks) Cycle no (=4 weeks) n=307 n=154n=154 n=153n=153 First TACE with DEBDOX performed 3-7 days after first day of treatment with sorafenib or placebo Subsequent TACE with DEBDOX performed on day 1 (±4 days) of cycles 3, 7, and 13, and every 6 cycles thereafter Patients allowed optional TACE sessions between cycles 7 and 13 and cycles 13 and 19, if deemed necessary by the investigator 63
 Contraindication to hepatic embolization procedures Planned liver transplantation Previous local therapy to target lesion Prior TACE, prior systemic therapy RANDOMIZERANDOMIZE Primary Endpoint Time to progression (by central review) Secondary Endpoints Overall survival Time to VI/EHS Time to untreatable progression Safety TACE (optional) Imaging Cycle no (=4 weeks) Cycle no (=4 weeks) n=307 n=154n=154 n=153n=153 First TACE with DEBDOX performed 3-7 days after first day of treatment with sorafenib or placebo Subsequent TACE with DEBDOX performed on day 1 (±4 days) of cycles 3, 7, and 13, and every 6 cycles thereafter Patients allowed optional TACE sessions between cycles 7 and 13 and cycles 13 and 19, if deemed necessary by the investigator 63")
64
Sorafenib (n=154), %Placebo (n=153), % Median age at enrolment (yrs) 64.563.0 Male 87.782.4 Etiology Hep B35.732.7 Hep C25.326.8 Alcohol17.519.6 HCC proven by biopsy 39.043.8 Liver cirrhosis present 85.690.3 Geographic region Europe50.651.6 North America11.011.1 Asia38.337.3
, %Placebo (n=153), % Median age at enrolment (yrs) Male Etiology Hep B Hep C Alcohol HCC proven by biopsy Liver cirrhosis present Geographic region Europe North America Asia")
65
Sorafenib (n=154), %Placebo (n=153), % AFP <400 ng/mL73.473.2 ≥400 ng/mL26.626.8 Child-Pugh score 563.668.6 635.730.7
, %Placebo (n=153), % AFP <400 ng/mL ≥400 ng/mL Child-Pugh score")
66
66 HR: 0.797 95% Cl: 0.588, 1.08 P = 0.072 Sorafenib Median: 169 days 95% Cl: 166, 219 days Placebo Median: 166 days 95% Cl: 113, 168 days

67
67 HR: 0.621 95% Cl: 0.321, 1.200 P = 0.076 Sorafenib Median: NR Placebo Median: NR

68
68 HR: 0.898 95% Cl: 0.606, 1.33 P = 0.295 Sorafenib Median: NR 95% Cl: 554 days, NR Placebo Median: NR 95% Cl: 562 days, NR

69
TTUP › Defined as time to the inability of a patient to further receive/benefit from TACE: Failure to achieve objective response after at least two TACE sessions Appearance of contraindications to TACE Vascular invasion Extrahepatic spread Sustained ascites Sustained Child-Pugh B Clinical progression to ECOG≥2 Plt count <60

70
70 HR: 1.586 95% Cl: 1.200, 2.096 P = 0.999 Sorafenib Median: 95 days 95% Cl: 62, 113 days Placebo Median: 224 days 95% Cl: 158, 288 days

71
TTUP longer in placebo group › What does this mean? Patients on sorafenib more likely to come off treatment Mainly due to developing contraindications to TACE (ie hepatic dysfunction, poor PS, low plt likely sorafenib S/Es) When looking at Asian vs Non-Asian patients: › Asian pts had longer TTUP in Sorafenib group Is TACE + Sorafenib more tolerable and/or efficacious in Asians??
 When looking at Asian vs Non-Asian patients: › Asian pts had longer TTUP in Sorafenib group Is TACE + Sorafenib more tolerable and/or efficacious in Asians .")
72
72 Patients stopped sorafenib earlier than placebo in Western countries (median 17 vs 28 weeks), whereas sorafenib was given longer than placebo in Asian countries (median 30 vs 18 weeks)
, whereas sorafenib was given longer than placebo in Asian countries (median 30 vs 18 weeks)")
73
Assessment Asian (n=104)Non-asian (n=200) Sorafenib (n=54) Placebo (n=50) Sorafenib (n=99) Placebo (n=101) Median Tx duration with study drug, wks 30.025.817.4 27.9 % of pts that received 1 TACE 24.122.042.4 17.8 % of pts that received 2 TACE 35.232.035.4 40.6 % of pts that received >2 TACE 38.944.020.2 39.7 % of pts that received TACE after SPACE 28.819.333.7 32.3 TTP HR 95% CI p value 0.720 0.457-1.135 0.078 0.865 0.576-1.3 2.43 OS HR 95% CI p value 0.677 0.355-1.292 0.117 1.062 0.646-1.745 0.594
Non-asian (n=200) Sorafenib (n=54) Placebo (n=50) Sorafenib (n=99) Placebo (n=101) Median Tx duration with study drug, wks % of pts that received 1 TACE % of pts that received 2 TACE % of pts that received >2 TACE % of pts that received TACE after SPACE TTP HR 95% CI p value OS HR 95% CI p value")
74
Adverse EventSorafenib (n=153), %Placebo (n=151), % All gradeGrade 3/4All gradeGrade 3/4 Diarrhea 52.93.9/017.20.7/0 HFSR 46.49.2/06.61.3/0 Fatigue 43.19.8/1.333.14.6/0.7 Nausea 37.90.7/039.10.7/0 Anorexia 30.72.0/020.50.7/0 Hypertension 30.116.3/016.69.3/0
, %Placebo (n=151), % All gradeGrade 3/4All gradeGrade 3/4 Diarrhea / /0 HFSR / /0 Fatigue / /0.7 Nausea / /0 Anorexia / /0 Hypertension / /0")
75
Primary endpoint of TTP was met › HR 0.797, p=0.072 (one-sided alpha 0.15) TACE + DEBDOX was feasible and well- tolerated Duration of sorafenib was longer in Asian arm, associated with greater efficacy (TTP, OS) › These positive signals in Asian population require further phase III studies Currently not enough data to change practice › Current std of care is to treat with Sorafenib after TACE fails
 TACE + DEBDOX was feasible and well- tolerated Duration of sorafenib was longer in Asian arm, associated with greater efficacy (TTP, OS) › These positive signals in Asian population require further phase III studies Currently not enough data to change practice › Current std of care is to treat with Sorafenib after TACE fails")































 Grants Chapter 6.>")

