Download presentation
Presentation is loading. Please wait.

1
STROKE UPDATE Carlos S. Kase, M.D. Department of Neurology Boston Medical Center Medicine Grand Rounds New England Baptist Hospital March 17, 2011

2
Albers GW, et al. Chest. 2001;119:300S-320S. Albers GW. Personal communication. February 27, 2003. Rosamond WD, et al. Stroke. 1999;30:736-743. Hemorrhagic Stroke (15%) Subarachnoid Hemorrhage (5%) Intracerebral Hemorrhage (10%) Cardioembolic (25%) Lacunar (15%) Ischemic Stroke (85%) Cryptogenic (15%) Large Vessel (30%) STROKE MECHANISMS ?
 Subarachnoid Hemorrhage (5%) Intracerebral Hemorrhage (10%) Cardioembolic (25%) Lacunar (15%) Ischemic Stroke (85%) Cryptogenic (15%) Large Vessel (30%) STROKE MECHANISMS .")
3
ADVANCES IN CEREBROVASCULAR DISEASE I.Treatment of Acute Ischemic Stroke II. Secondary Stroke Prevention

4
ADVANCES IN CEREBROVASCULAR DISEASE I.Treatment of Acute Ischemic Stroke IV ThrombolysisIV Thrombolysis IA ThrombolysisIA Thrombolysis EmbolectomyEmbolectomy

5
ADVANCES IN CEREBROVASCULAR DISEASE I.Treatment of Acute Ischemic Stroke IV ThrombolysisIV Thrombolysis IA ThrombolysisIA Thrombolysis EmbolectomyEmbolectomy

6
Acute assessment of patient with ischemic stroke TIME IS BRAIN! - Time of symptom onset: Based on patient report or if patient unable to report it, use the last time the patient was seen well, at baseline - Coagulopathy (inherited or acquired) - Inclusion criteria for t-PA – the only FDA- approved treatment for acute ischemic stroke
 - Inclusion criteria for t-PA – the only FDA- approved treatment for acute ischemic stroke.")
7
Eligibility for treatment of acute ischemic stroke patients with IV t-PA Inclusion criteria Clearly defined time of onset NIHSS score > 4 CT: no evidence of ICH, ischemia < 1/3 MCA territory Discussion of risks/benefits; obtain consent Exclusion criteria Recent stroke or head trauma within the preceding 3 months Major surgery within 14 days History of ICH SBP > 185 mm Hg or DBP > 110 Aggressive therapy for BP control Rapidly improving or minor symptoms Symptoms suggestive of SAH Seizure at the onset GI or GU bleeding within previous 21 d. Arterial puncture at a non-compressible site within 7 days Heparin within preceding 48 hours INR > 1.5 Platelets < 100,000 Glucose 400mg/dl

8
First proven effective therapy for acute stroke Double-blind, randomized, 624 pts. t-PA 0.9 mg/kg (max. 90 mg) IV over 1 hour Treatment started < 3 hrs. from stroke onset CT documenting absence of hemorrhage No anticoagulants/antiplatelets for 24 hrs. NINDS t-PA Study NEJM 1995;333:1581-7
 IV over 1 hour Treatment started < 3 hrs. from stroke onset CT documenting absence of hemorrhage No anticoagulants/antiplatelets for 24 hrs. NINDS t-PA Study NEJM 1995;333:")
11
NINDS IV t-PA Study Symptomatic ICH within 36 hours from Rx 6.4% 0.6% Symptomatic ICH t-PA: 20/312 Control: 2/312

13
IV tPA Declining Benefit over Time Hacke W, et al. Lancet 2004;363:768-74

14
IV tPA Declining Benefit over Time Hacke W, et al. Lancet 2004;363:768-74 4½ h.

15
NEJM 2008;359;1317-29

19
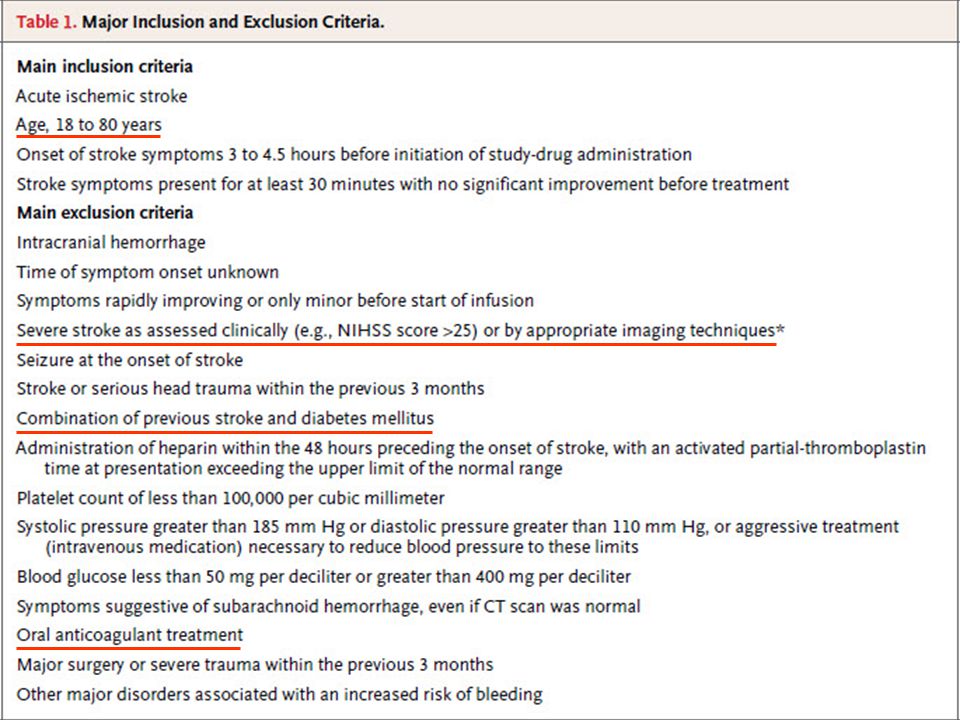
Stroke 2009;40:2945-8 The eligibility criteria for treatment in this time period are similar to those for persons treated at earlier time periods, with any one of the following additional exclusion criteria: Patients older than 80 years, those taking oral anticoagulants, those with a baseline National Institutes of Health Stroke Scale score >25, or those with both a history of stroke and diabetes.

20
ADVANCES IN CEREBROVASCULAR DISEASE I.Treatment of Acute Ischemic Stroke IV ThrombolysisIV Thrombolysis IA ThrombolysisIA Thrombolysis EmbolectomyEmbolectomy

22
(Prolyse in Acute Cerebral Thromboembolism)
")
23
PROACT II 180 patients 6-hour window MCA stem or division occlusion 121 proUK (9 mg) IA; 59 control Efficacy: Rankin 0-2 at 90 days Safety: Rate of symptomatic ICH, mortality
 IA; 59 control Efficacy: Rankin 0-2 at 90 days Safety: Rate of symptomatic ICH, mortality")
24
PROACT II TRIAL Furlan A, Higashida R, Wechsler L, et al. - JAMA 1999;282:2003-11 Randomized trial of IA pro-Urokinase+heparin v. heparin in angiographically-documented MCA occlusion RESULTS Rankin < 2 at 3 months in 40% r-proUK, 25% control (p=.04) Symptomatic ICH in 10% r-proUK, 2% control (p=.06) Recanalization 66% r-proUK, 18% control (p<.001) Mortality 25% r-proUK, 27% control
 Symptomatic ICH in 10% r-proUK, 2% control (p=.06) Recanalization 66% r-proUK, 18% control (p<.001) Mortality 25% r-proUK, 27% control.")
26
Diagnostic Imaging Evaluation Head CT without contrast: r/o ICH CTA: Evaluation for large artery occlusion CTP: Evaluation of perfusion mismatch MRI: Extent of infarct on DWI MRA: Large artery occlusion MRP: Evaluation of perfusion mismatch

27
CBV Cerebral Blood Volume MTT Mean Transit Time Perfusion Mismatch Penumbra =Tissue at Risk

28
CBV Cerebral Blood Volume MTT Mean Transit Time Perfusion Match No Penumbra

29
Diagnostic Evaluation: MRI DWIPWI

30
Diagnostic Evaluation

31
Clinical and Imaging Results of IV Thrombolysis Based on Presence of Mismatch - The DEFUSE Study Albers GW, et al. Ann Neurol 2006;60:508-17

32
Clinical and Imaging Results of IV Thrombolysis Based on Absence of Mismatch - The DEFUSE Study Albers GW, et al. Ann Neurol 2006;60:508-17

33
Clinical and Imaging Results of IV Thrombolysis Based on Malignant Imaging Profile - The DEFUSE Study Albers GW, et al. Ann Neurol 2006;60:508-17

34
33% 75% 14% 40% 43% 12.5% 27% 25% 12.5% 43% Functional Outcome after Thrombolysis with or without Mismatch, with or without Early Reperfusion - The DEFUSE Study Albers GW, et al. Ann Neurol 2006;60:508-17

35
ADVANCES IN CEREBROVASCULAR DISEASE I.Treatment of Acute Ischemic Stroke IV ThrombolysisIV Thrombolysis IA ThrombolysisIA Thrombolysis EmbolectomyEmbolectomy

36
Mechanical removal of thrombus: MERCI trial Embolectomy device (Merci Retriever) to open occluded intracranial large vessels within 8 hours of symptom onset All patients ineligible for intravenous tPA Outcomes - Recanalization and safety - Neurological outcome at 90 days in recanalized vs. non-recanalized patients Intra-arterial thrombectomy Smith WS, et al. Stroke 2005;36:1432-8

39
ACUTE ISCHEMIC STROKE TREATMENT OPTIONS TIME (HOURS) IV t-PA Intra-arterial Thombolysis/ Thrombectomy MERCI MR Rescue trial 0 - 3 4½ 6 - 8 0-80-8 IV tPA extended window
 IV t-PA Intra-arterial Thombolysis/ Thrombectomy MERCI MR Rescue trial ½ IV tPA extended window")
40
ADVANCES IN CEREBROVASCULAR DISEASE I.Treatment of Acute Ischemic Stroke IV ThrombolysisIV Thrombolysis IA ThrombolysisIA Thrombolysis EmbolectomyEmbolectomy HemicraniectomyHemicraniectomy

41
Pre-op - 5/29/07 Post-op - 5/30/07 Post-op – 7/24/07 L.F. – MR# 3546883 11 y/o girl Dominant hemisphere infarct, full MCA + PCA, due to intracranial ICA occlusion Hemicraniectomy on day 2, b/o signs of herniation and brainstem compression

42
DECIMAL DECIMAL (France) Started in 2001 Started in 2001 MRI-based inclusion MRI-based inclusion Early surgery (<30h) Early surgery (<30h) Stroke severity NIHSS≥15 Stroke severity NIHSS≥15 Projected sample size 60 (30/30) Projected sample size 60 (30/30) Interrupted after 38 patients for slow recruitment, significant difference in mortality, and the perspective of a pooled analysis Interrupted after 38 patients for slow recruitment, significant difference in mortality, and the perspective of a pooled analysis DESTINY DESTINY (Germany) Started 2004 Started 2004 CT-based inclusion CT-based inclusion Early surgery within 36h Early surgery within 36h Stroke severity NIHSS≥18/20 Stroke severity NIHSS≥18/20 Projected sample size 68 (34/34) Projected sample size 68 (34/34) On hold after 32 patients (assess mRS, mortality) On hold after 32 patients (assess mRS, mortality) HAMLET HAMLET (Holland) Started in 2002 Started in 2002 CT-based inclusion CT-based inclusion Surgery (within 99h) Surgery (within 99h) Stroke severity NIHSS≥16/21 Stroke severity NIHSS≥16/21 Projected sample size 112 patients Projected sample size 112 patients Randomization ongoing Randomization ongoing 57 patients included 57 patients included Design of the Pooled Analysis PRIMARY END-POINT: mRS 0-4 v. 5+6 at 1 year SECONDARY END-POINTS: Case fatality; mRS 0-3 v. 4-6 at 1 year

43
Inclusion/Exclusion Criteria for Pooled Analysis

44
Modified Rankin Scale score at 12 months Vahedi K, et al. Lancet Neurol 2007;6:215-222

45
Pooled Analysis CONCLUSIONS Decompressive craniectomy was statistically superior to non-surgical management for the primary and the 2 secondary end-points Decompressive craniectomy decreases mortality without increasing the number of severely disabled individuals

46
ADVANCES IN CEREBROVASCULAR DISEASE II. Secondary Stroke Prevention Risk factor controlRisk factor control Anti-platelet agentsAnti-platelet agents AnticoagulantsAnticoagulants Interventional proceduresInterventional procedures

47
ADVANCES IN CEREBROVASCULAR DISEASE II. Secondary Stroke Prevention Risk factor controlRisk factor control Anti-platelet agentsAnti-platelet agents AnticoagulantsAnticoagulants Interventional proceduresInterventional procedures

49
(Perindopril Protection Against Recurrent Stroke Study)
")
52
Serum cholesterol (mg/dl) Incidence rates / 1,000 yr Age-Adjusted Incidence Rate of ICH in Men with Cholesterol <200 mg/dl Yano K, et al. Stroke 1989;20;1460-5

53
Stroke 2008;39:1647-52

55
ATRIAL FIBRILLATION

57
Fibrin Clot IIa Inhibitors XII VII VIII IX XI II V X I Direct Thrombin Inhibitors Tested: Ximelagatran Dabigatran New: Dabigatran Direct thrombin inhibitors

58
Fibrin Clot IIa Inhibitors XII VII VIII IX XI II V X I Direct Thrombin Inhibitors Tested: Ximelagatran Dabigatran New: Dabigatran Direct thrombin inhibitors Ximelagatran As effective as warfarin Hepatotoxic

59
Fibrin Clot IIa Inhibitors XII VII VIII IX XI II V X I Direct Thrombin Inhibitors Tested: Ximelagatran Dabigatran New: Dabigatran Direct thrombin inhibitors Ximelagatran As effective as warfarin Hepatotoxic

60
pp. 1139-1151

61
18,113 patients randomized Design: Open-label, Non-Inferiority trial Median treatment duration: 2 years 951 centers in 44 countries December 2005 to March 2009 pp. 1139-1151
62
Stroke / Systemic Embolism – RE-LY Study % per year 1.53 1.11 P < 0.001 (NI) P < 0.001 (SUP) RRR: 45% 182/6,025 134/6,076 199/6,022 1.69
 P < (SUP) RRR: 45% 182/6, /6, /6,")
64
Major bleeding and components CharacteristicD 110 mg D 150 mg Warfar in P-value 110 vs. W P-value 150 vs. W Number of patients 601560766022 Major bleeding 2.713.113.360.0030.31 - Life threatening - Non-life threatening - Gastrointestinal 1.221.661.121.451.881.511.801.761.02<0.0010.560.430.0370.47<0.001 Data represent %/year

65
Net clinical benefit and components CharacteristicD 110 mg D 150 mg Warfari n P-value 110 vs. W P-value 150 vs. W Number of patients (n) 601560766022 Net Clinical Benefit 7.096.917.640.100.04 - Stroke / SE - Death - MBE* - PE - MI 1.53 3.75 2.71 0.12 0.721.113.64 3.11 0.15 0.741.694.133.360.090.53 <0.001 (NI) 0.34 (sup) 0.130.0030.560.07 <0.001 (NI) <0.001 (sup) 0.0510.310.210.048 Data represent %/year * Major Bleeding Events
 Net Clinical Benefit Stroke / SE - Death - MBE* - PE - MI <0.001 (NI) 0.34 (sup) <0.001 (NI) <0.001 (sup) Data represent %/year * Major Bleeding Events.")
67
Dabigatran for Stroke Prevention in AF: Pros and Cons Cons Open-label design Short f/u period (2 years) Small absolute risk reduction Increase in rate of MI Increase rate GI bleeding Lack of antidote More expensive than warfarin Pros NI/superior to warfarin Fixed-dose Rapid onset of action No need x monitoring No drug/food interactions Lower rates of ICH No hepatotoxicity
 Small absolute risk reduction Increase in rate of MI Increase rate GI bleeding Lack of antidote More expensive than warfarin Pros NI/superior to warfarin Fixed-dose Rapid onset of action No need x monitoring No drug/food interactions Lower rates of ICH No hepatotoxicity")
68
ADVANCES IN CEREBROVASCULAR DISEASE II. Secondary Stroke Prevention Risk factor controlRisk factor control Anti-platelet agentsAnti-platelet agents AnticoagulantsAnticoagulants Interventional proceduresInterventional procedures

69
Aspirin GP IIB/IIIA (Fibrinogen receptor) ADP Collagen Thrombin TxA 2 Ticlopidine Clopidogrel Activation ADP-R Phosphodiesterase Adenosine uptake Dipyridamole TxA2 COX Mechanisms of Action of Antiplatelet Agents
 ADP Collagen Thrombin TxA 2 Ticlopidine Clopidogrel Activation ADP-R Phosphodiesterase Adenosine uptake Dipyridamole TxA2 COX Mechanisms of Action of Antiplatelet Agents")
71
Aspirin Efficacy by Dose: Meta-Analyses in Patients with Stroke or TIA Endpoint: Stroke, MI, or Vascular Death -10-5 0 51015202530 RRR (%) ± 95% CI Low Dose Medium Dose High Dose Algra, van Gijn Johnson Tijssen 50 - 100 50 50 - 75 300 75 - 300 300 900 - 1500 650 - 1500 900 - 1500 Dose (mg/day)
 ± 95% CI Low Dose Medium Dose High Dose Algra, van Gijn Johnson Tijssen Dose (mg/day)")
72
Clopidogrel v. ASA in Pts. at Risk of Ischemic Events (CAPRIE) Randomized, blinded, multicenter trial designed to assess the relative efficacy of clopidogrel (75 mg/day) and ASA (325 mg/day). Randomized, blinded, multicenter trial designed to assess the relative efficacy of clopidogrel (75 mg/day) and ASA (325 mg/day). Primary outcome measure was the composite of ischemic stroke, MI or vascular death. Primary outcome measure was the composite of ischemic stroke, MI or vascular death. Enrolled 19,185 patients, >6000 in each of the three groups. Enrolled 19,185 patients, >6000 in each of the three groups. CAPRIE Steering Committee. Lancet. 1996;348:1329-39.
 Randomized, blinded, multicenter trial designed to assess the relative efficacy of clopidogrel (75 mg/day) and ASA (325 mg/day). Randomized, blinded, multicenter trial designed to assess the relative efficacy of clopidogrel (75 mg/day) and ASA (325 mg/day). Primary outcome measure was the composite of ischemic stroke, MI or vascular death. Primary outcome measure was the composite of ischemic stroke, MI or vascular death. Enrolled 19,185 patients, >6000 in each of the three groups. Enrolled 19,185 patients, >6000 in each of the three groups. CAPRIE Steering Committee. Lancet. 1996;348:")
73
8.7% RRR Time from Randomization (Months) p = 0.043 0 4 8 12 16 0 15 2127369121824303336 Aspirin 5.32% Clopidogrel 5.83% Event rate per year Cumulative Risk % Lancet. 1996;348:1329-1339. CAPRIE: Primary Analysis Combined Endpoint

74
European Stroke Prevention Study (ESPS-2) TIA or stroke <3 months 6,602 patients R DP-XR 200 mg BID (N=1,654) ASA 25 mg BID (N=1,649) DP-XR 200 mg + ASA 25 mg BID (N=1,650) Placebo (N=1,649) Design 2 x 2 factorial design Stroke (76%) or TIA (24%) Endpoints Primary: Stroke, death, stroke and death Secondary: TIA, MI Follow-up: 2 years Diener H-C. et al. J Neurol Sci. 1996;143:1-13

75
ESPS-2 Results: Stroke-Free Survival 80 85 90 95 100 % Patients Without Stroke ASA/ER-DP ER-DP ASA Placebo 6121824 Time (months)
")
76
ESPS-2: Results Both ER-DP and ASA had an independent and statistically significant effect in reducing the risk of stroke recurrence (16% and 18%, respectively) when compared with placebo Both ER-DP and ASA had an independent and statistically significant effect in reducing the risk of stroke recurrence (16% and 18%, respectively) when compared with placebo The combination of ER-DP and ASA was additive, with a 37% RRR The combination of ER-DP and ASA was additive, with a 37% RRR ER-DP plus ASA reduced the risk of stroke, both fatal and non-fatal, by 23% vs. ASA alone ER-DP plus ASA reduced the risk of stroke, both fatal and non-fatal, by 23% vs. ASA alone

77
Aspirin vs control Meta-analysis 11 RCT, 9469 pts Dipyridamole vs aspirin Meta-analysis 3 RCT, 3386 pts Trifusal vs aspirin Meta-analysis 4 RCT, 2918 pts Ticlopidine vs aspirin 1 RCT, 3069 pts Clopidogrel vs aspirin 1 RCT, 19185 pts Clopidogrel vs aspirin 1 RCT, 6431 pts Clopidogrel + aspirin vs aspirin 1 RCT, 15602 pts Clopidogrel + aspirin vs aspirin 1 RCT, 4320 pts Dipyridamole + aspirin vs aspirin Meta-analysis, 6 RCT, 7612 pts Clopidogrel + aspirin vs clopidogrel 1 RCT, 7599 pts Dipyridamole + aspirin vs clopidogrel 1 RCT, 20332 pts Relative risk reduction % -1010203040 Clinical Trials of Antiplatelet Agents for Stroke Prevention

78
ACCP Guidelines - Antiplatelet Agents “ ” “For long-term stroke prevention in patients with noncardioembolic stroke or transient ischemic attack (TIA) [ie, atherothrombotic, lacunar, or cryptogenic], we recommend treatment with an antiplatelet agent (Grade 1A), including aspirin (recommended dose, 50–100 mg/d), the combination of aspirin and extended-release dipyridamole (25 mg/200 mg bid), or clopidogrel (75 mg qd). In these patients, we recommend use of the combination of aspirin and extended-release dipyridamole (25/200 mg bid) over aspirin (Grade 1A) and suggest clopidogrel over aspirin (Grade 2B), and recommend avoiding long-term use of the combination of aspirin and clopidogrel (Grade 1B). For patients who are allergic to aspirin, we recommend clopidogrel (Grade 1A)” Albers et al., Chest 2008;133;630S-669S
![ACCP Guidelines - Antiplatelet Agents For long-term stroke prevention in patients with noncardioembolic stroke or transient ischemic attack (TIA) [ie, atherothrombotic, lacunar, or cryptogenic], we recommend treatment with an antiplatelet agent (Grade 1A), including aspirin (recommended dose, 50–100 mg/d), the combination of aspirin and extended-release dipyridamole (25 mg/200 mg bid), or clopidogrel (75 mg qd).](http://images.slideplayer.com/9/2490039/slides/slide_78.jpg "In these patients, we recommend use of the combination of aspirin and extended-release dipyridamole (25/200 mg bid) over aspirin (Grade 1A) and suggest clopidogrel over aspirin (Grade 2B), and recommend avoiding long-term use of the combination of aspirin and clopidogrel (Grade 1B). For patients who are allergic to aspirin, we recommend clopidogrel (Grade 1A) Albers et al., Chest 2008;133;630S-669S.")
79
ADVANCES IN CEREBROVASCULAR DISEASE II. Secondary Stroke Prevention Risk factor controlRisk factor control Anti-platelet agentsAnti-platelet agents AnticoagulantsAnticoagulants Interventional proceduresInterventional procedures

80
NEJM 2001;345:1444-1451 Secondary stroke prevention trial Design: multicenter, double-blind, randomized Non-cardioembolic, non-operable carotid stroke in prior 3 months Agents: warfarin (INR=1.4-2.8) vs. ASA (325 mg qd) N = 1,103 warfarin – 1,103 ASA Duration of treatment: 2 years Primary end-point: recurrent ischemic stroke/death in 2 yrs. Adverse experience: hemorrhage Analysis: intention-to-treat WARSS
 N = 1,103 warfarin – 1,103 ASA Duration of treatment: 2 years Primary end-point: recurrent ischemic stroke/death in 2 yrs. Adverse experience: hemorrhage Analysis: intention-to-treat WARSS.")
81
Warfarin Aspirin 70 80 90 100 Warfarin Aspirin 1103972885 1103984900 Hazard rate ratio=1.13 95% CI 0.92-1.38 two-sided p-value=0.25 Kaplan-Meier: Recurrent Ischemic Stroke or Death Percent free of event Number at risk 090180270360450540630720 Days after randomization

82
ADVANCES IN CEREBROVASCULAR DISEASE II. Secondary Stroke Prevention Risk factor controlRisk factor control Anti-platelet agentsAnti-platelet agents AnticoagulantsAnticoagulants Interventional proceduresInterventional procedures

83
CEA for Stroke Prevention: Symptomatic v. Asymptomatic Carotid Stenosis Stroke Rate (%/year) 13% 4% 2% 1% (>70% stenosis) (>60% stenosis)
 13% 4% 2% 1% (>70% stenosis) (>60% stenosis).")
84
Carotid Endarterectomy for Stroke Prevention: Summary Benefit is established for high-grade (> 70%) symptomatic carotid stenosis Value in moderate (50-69%) symptomatic stenosis established, but of smaller magnitude No value for symptomatic carotid stenosis < 50% Role of carotid angioplasty/stenting undergoing evaluation in clinical trials
 symptomatic carotid stenosis Value in moderate (50-69%) symptomatic stenosis established, but of smaller magnitude No value for symptomatic carotid stenosis < 50% Role of carotid angioplasty/stenting undergoing evaluation in clinical trials")
85
CAROTID ARTERY STENOSIS Endarterectomy or Angioplasty/Stenting?

86
SAPPHIRE trial NEJM 2006;351;1493-501

87
SAPPHIRE trial Criteria for High-Risk for CEA

88
Patients at High Risk for CEA High cervical carotid lesions (above bifurcation) Re-stenosis after CEA Stenosis after neck area XRT Stenosis after radical neck dissection Contralateral ICA occlusion Concomitant symptomatic cardiac, pulmonary disease (poor general anesthesia/surgical risk)
 Re-stenosis after CEA Stenosis after neck area XRT Stenosis after radical neck dissection Contralateral ICA occlusion Concomitant symptomatic cardiac, pulmonary disease (poor general anesthesia/surgical risk)")
89
SAPPHIRE Stenting and Angioplasty with Protection in Patients at High Risk for Endarterectomy 747 167 NEJM 2004;351:1493-1501

90
SAPPHIRE results – 30 days Intention-to-Treat Analysis Percentage of patients (%) 9.8% 4.8% p value 0.08 0.60 0.07 0.08
 9.8% 4.8% p value")
91
EVA-3S trial NEJM 2006;355:1660-71

92
EVA-3S results – 30 days Intention-to-Treat Analysis Percentage of patients (%) p value 0.68 0.004 0.62 8.8% 2.7%
 p value % 2.7%")
93
CREST trial NEJM 2010;363:11-23

94
Patient Characteristics CAS (n=1262) CEA (n=1240) Age69 Female - %3634 Asymptomatic - %47 Hypertension - %86 Diabetes - %30 Dyslipidemia - %8285 Current smoker - %26
 CEA (n=1240) Age69 Female - %3634 Asymptomatic - %47 Hypertension - %86 Diabetes - %30 Dyslipidemia - %8285 Current smoker - %26")
95
Patient Characteristics CAS(n=1262)CEA(n=1240) Cardiovascular disease - % 4143 Systolic BP, mean mmHg 142141 % stenosis ≥ 70% 8587 Days from randomization to treatment 67
CEA(n=1240) Cardiovascular disease - % 4143 Systolic BP, mean mmHg % stenosis ≥ 70% 8587 Days from randomization to treatment 67")
96
Primary Endpoint ≤ 4 years (any stroke, MI, or death within peri-procedural period plus ipsilateral stroke thereafter) CAS vs. CEA CAS vs. CEA Hazard Ratio, 95% CI Hazard Ratio, 95% CIP-Value 7.2 vs. 6.8% HR=1.11; 95% CI: 0.81-1.51 0.51

97
Primary Endpoint ≤ 4 years (any stroke, MI, or death within peri-procedural period plus ipsilateral stroke thereafter) CAS vs. CEA CAS vs. CEA Hazard Ratio, 95% CI Hazard Ratio, 95% CIP-Value 7.2 vs. 6.8% HR=1.11; 95% CI: 0.81-1.51 0.51

98
Primary Endpoint ≤ 4 years (any stroke, MI, or death within peri-procedural period plus ipsilateral stroke thereafter) CAS vs. CEA CAS vs. CEA Hazard Ratio, 95% CI Hazard Ratio, 95% CIP-Value 7.2 vs. 6.8% HR=1.11; 95% CI: 0.81-1.51 0.51

99
CREST Trial Peri-procedural Stroke and MI Event Rate (%) 2.3% 4.1% 2.3% 1.1% P=0.01 P=0.03
 2.3% 4.1% 2.3% 1.1% P=0.01 P=0.03")
100
CREST trial NEJM 2010;363:11-23

101
Impact of periprocedural events (stroke/MI) on SF-36 at 1 year adjusting age, sex, symptomatic cerebrovascular disease and baseline SF-36 measures – Growth Curve Modeling.
 on SF-36 at 1 year adjusting age, sex, symptomatic cerebrovascular disease and baseline SF-36 measures – Growth Curve Modeling.")
103
Conclusions CEA and CAS have similar net outcomes though the individual risks vary, lower stroke with CEA and lower MI with CAS CEA and CAS have similar net outcomes though the individual risks vary, lower stroke with CEA and lower MI with CAS Younger patients may have improved efficacy with CAS and older patients with CEA Younger patients may have improved efficacy with CAS and older patients with CEA For the future, both CEA and CAS appear to be useful tools for preventing stroke For the future, both CEA and CAS appear to be useful tools for preventing stroke

104
Conclusions At experienced centers both CEA and CAS appear to have low perioperative complications and excellent longer-term results At experienced centers both CEA and CAS appear to have low perioperative complications and excellent longer-term results For the future, both CEA and CAS appear to be useful tools for preventing stroke For the future, both CEA and CAS appear to be useful tools for preventing stroke

Similar presentations





















 University of Helsinki Markku Kaste Department.>")












 Thrombolytic canalization of occluded arteries may reduce the degree.>")
