Download presentation
Presentation is loading. Please wait.

1
Antiplatelet and anticoagulant therapy in stroke prevention
Dr Sepehr Shakib Director Clinical Pharmacology Royal Adelaide Hospital

2
Topics Stroke basics Risk calculators Lipids and strokes Antiplatelets
Clopidogrel Aspirin + dipyridamole Warfarin for AF

3
What are the different types of strokes?
Ischemic Lacunar Thrombotic Cardioembolic Watershed Hemorrhagic

4
Ischemic strokes Lacunar:
Occlusion of deep penetrating branches of arteries Occlusion caused by microatheroma, lipohyalinosis, hypertension changes Most caused by hypertension Account for 20% of all ischemic strokes

5
Lacunar stroke

6
Ischemic strokes Cardioembolic Thrombotic strokes
Strokes from other parts of the vascular tree eg atrial fibrillation, recent MIs, endocarditis, aortic arch etc… Some caused by lipid accumulation Thrombotic strokes Due to development of thrombosis and occlusion of blood vessels supplying brain eg middle cerebral artery

7
Middle cerebral artery stroke

8
Hemorrhagic strokes Much more rare and more catastrophic Caused by:
Hypertension Amyloid angiopathy Aneurysms

9
Hemorrhagic stroke

10
Hemorrhagic transformation
Development of hemorrhage in large ischemic stroke

11
Risk calculators: http://www.cvdcheck.org.au/

12
Risk 52 years old Bp 142/87 Family history of IHD LDL 6.4, HDL 0.8
Has just stopped smoking

13
Risk Engine Based on UKPDS follow-up data

14
Relationship between lipids and strokes
BMJ June 2003

15
Stroke reduction for 1mmol/L reduction in LDL cohort studies
ischemic strokes 19% increase in hemorrhagic strokes

16
Association between lipids and strokes summary
As your LDL falls ischemic strokes ↑ hemorrhagic strokes Overall benefit depends on the relative balance of absolute risks of ischemic vs hemorrhagic strokes Even with ischemic strokes get smaller relative reduction in events than IHD Cf 32% (95% CI 27-36%) reduction in ischemic heart disease events for every 1 mmol/L reduction in LDL
 reduction in ischemic heart disease events for every 1 mmol/L reduction in LDL.")
17
Benefits of lipid lowering in trials
Original evidence from IHD trials Eg reduction in strokes in 4S and LIPID study Heart Protection Study first study to demonstrate reduction in strokes in those without IHD (Lancet 2002) 25% reduction in all strokes
 25% reduction in all strokes.")
18
Aspirin Antithrombotic Trialists’ Collaboration BMJ 2002
287 studies involving 205,000 patients! Most placebo controlled data related to aspirin

19
Relative Benefit

20
Absolute benefit

21
Benefits in other vascular events

22
What about risk of bleeding?

23
GI bleeding Meta-analysis 24 RCTs with 66,000 patients
0.45% annual bleeding rate OR (95% CI )
")
24
Hemorrhagic stroke risk
16 trials, patients 108 hemorrhagic strokes Risk 0.05% per year

25
What about dose of aspirin - efficacy
“There remains uncertainty about such low doses (<75mg) are as effective” Antiplatelet Trialists Collaboration
 are as effective Antiplatelet Trialists Collaboration.")
26
Dose of aspirin - toxicity?
Opinion quite varied from there being no dose dependency to there being one No direct comparison of doses Small adverse event rate Differences in background populations in different studies

27
Am J Cardiol 2005 31 trials 192,036 patients
Looked at low (<100mg), moderate (1-200mg) and high dose (>200)
, moderate (1-200mg) and high dose (>200)")
28
Bleeding risk There appears to be dose dependency
Toxicity is substantial even at low dose

29
Aspirin summary Effective at reducing rate of recurrent stroke
Even small doses associated with risk of bleeding Mainly GI bleeding but some intracerebral Benefit outweighs risk in patients with previous stroke There appears to be increased toxicity at increased doses

30
Aspirin Questions?

31
Clopidogrel CAPRIE study Clopidogrel 75mg vs aspirin 325mg
History of stroke, MI, or peripheral vascular disease 19,185 patients

32
Clopidogrel efficacy 5.8% 5.3%

33
Clopidogrel toxicity * p<.05

34
Aspirin + Dipyridamole
Antithrombotic Trialists Collaboration 2002 6% non-significant reduction in strokes with addition of dipyridamole to aspirin Systematic review of 25 studies, involving 10,404 patients

35
ESPRIT study 2700 patients randomised to any dose of aspirin +dipyridamole SR 200mg twice daily Open label

36
Esprit results Fewer strokes with aspirin + dipyridamole
Fewer hemorrhages with aspirin + dipyridamole (??) Systematic review of 6 studies shows reduction in recurrent events
 Systematic review of 6 studies shows reduction in recurrent events.")
37
Which is the ideal antiplatelet?
Antiplatelet therapy Which is the ideal antiplatelet? Stroke 2008 meta-analysis: addition of dipyridamole to aspirin: ‘robust benefit’ Editorial: “…considering the 40 times difference in cost and the discrepancies noted above, such benefit is uncertain and, judging by the data, far from robust”

38
What about aspirin+dipyridamole compared to clopidogrel?

39
PROFESS Recent ischemic strokes Randomised to clopidogrel or asa+dip
20,000 patients for 2.5 years Non-inferiority design

40
Primary outcome- recurrent stroke
Hazard Ratio for Aspirin–ERDP 1.01 (0.92–1.11)
")
41
Safety outcomes

42
Other safety

43
Antithrombotic options
Drug Efficacy Adverse effects Aspirin 22% in risk Bleeding risk (0.5-1% per year) Aspirin + dipyridamole ? more effective than aspirin Headaches, nausea, flushing Clopidogrel Slightly more effective than aspirin Similar bleeding to aspirin Warfarin Same as aspirin More bleeding Aspirin + Clopidogrel
 Aspirin + dipyridamole. more effective than aspirin. Headaches, nausea, flushing. Clopidogrel. Slightly more effective than aspirin. Similar bleeding to aspirin. Warfarin. Same as aspirin. More bleeding. Aspirin + Clopidogrel.")
44
Antiplatelet key messages
Aspirin is antithrombotic of choice in primary stroke prevention when CV risk is high Aspirin, aspirin+dipyridamole or clopidogrel are main antiplatelet cfhoices in secondary stroke prevention Choice depends on circumstances (PBS criteria, intolerances)
")
45
Antiplatelet questions?

46
Risk of stroke with AF Risk highest with valvular AF
All other stratification tools refer to non-valvular AF There are numerous different risk stratification tools which rely on different risk factors

47
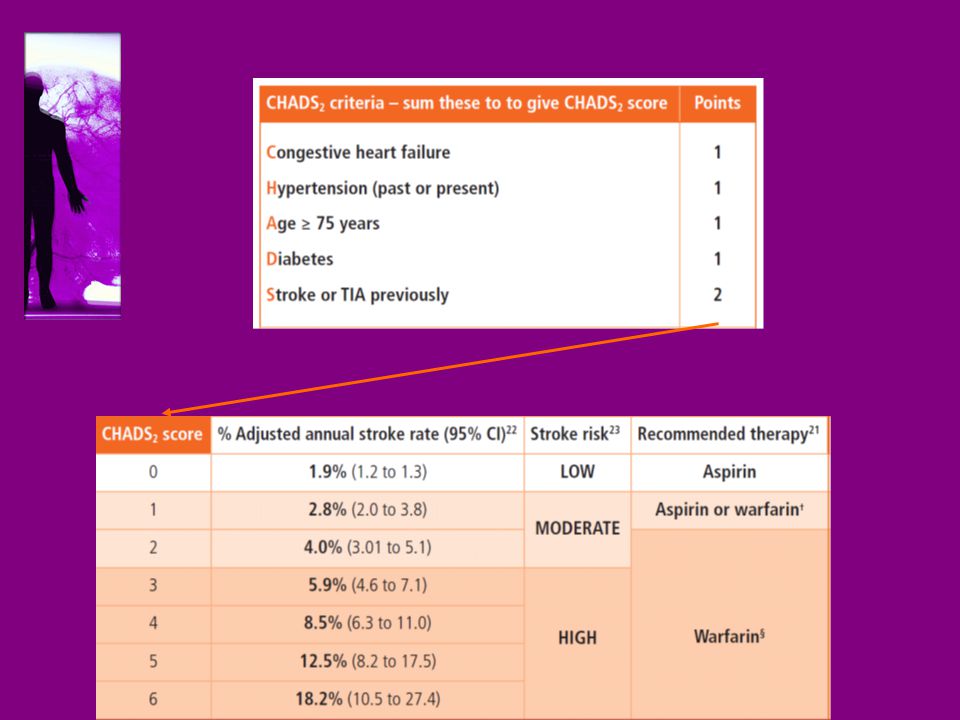
CHADS2 Score National Registry of Atrial Fibrillation JAMA 2001
Subsequently validated in different studies

49
Benefit of antithrombotic therapy
Warfarin reduces risk of stroke by 70% Aspirin reduces risk by 30% Less effect on large disabling strokes Aspirin + dipyridamole- very limited data Clopidogrel- no data Aspirin + clopidogrel- not as good as warfarin ? Better than aspirin

50
Warfarin contraindications

51
Not contraindications
Co-prescription of interacting drug

52
What is risk of bleeding with warfarin?
Literature rate varies between 0.1%-50% per year Initiation/transition period Risk of mis-communication, new behavior Modifiable risk Bleeding due to underlying lesion Eg colonic polyp, peptic ulcer, bladder lesion “Desirable” bleeding Not modifiable Long term bleeding risk Depends on risk factors of bleeding and how well managed Partly modifiable

53
5 point risk calculator Only applies to patients who are suitable for warfarin Validated in other populations Am J Med 1998

54
5 point bleeding scale 1 point each for :
Age > 65 History of stroke History of gastrointestinal bleeding 1 point for any of: diabetes, recent MI, Hb<10, Creat >.13mmol/L Score Classifi-cation Risk of major bleed At 1 year Low 3% 1 - 2 Intermediate 12% 3 - 4 High 25%+

55
Warfarin questions?

Similar presentations