Download presentation
Presentation is loading. Please wait.

1
INGUINAL HERNIA REPAIR: OPEN vs TEP APPROACHES
Prof Dr Orhan Alimoğlu Department of General Surgery Istanbul Medeniyet University

2
Inguinal hernia One of the most common surgical problem in daily practice Different operations and approaches Gold standard: repair with mesh Currently Lichtenstein hernia repair Endoscopic totally extra-peritoneal (TEP) repair Laparoscopic trans-abdominal preperitoneal (TAPP) repair
 repair. Laparoscopic trans-abdominal preperitoneal (TAPP) repair.")
3
General Precautions No place for routine antibiotic and thromboembolic prophylaxis, only in selected patients Risk factors for wound and mesh infection Advanced age Corticosteroid use Immunosuppression Obesity Diabetes Malignancy

4
Characteristics of mesh
Large vs small Low-weight vs heavy weight Micropore vs macropore Conclusion: Efficiency of lighter mesh with larger pores only during the first few postoperative weeks

5
Lichtenstein Inguinal Hernia Repair
Large mesh (7*15 cm) 2 cm medial to the pubic tubercle, 3–4 cm above the Hesselbach’s triangle, and 5–6 cm lateral to the internal ring, trimming 3–4 cm from its lateral side Crossing and suturing tails of mesh behind spermatic cord Securing mesh with two interrupted sutures on upper edge and one continuous suture with no more than three to four passes on lower edge of mesh Keeping mesh with a slightly relaxed, tented up, or dome-shaped configuration Identification and protection of the ilioinguinal, iliohypogastric, and genital nerves
 2 cm medial to the pubic tubercle, 3–4 cm above the Hesselbach’s triangle, and 5–6 cm lateral to the internal ring, trimming 3–4 cm from its lateral side. Crossing and suturing tails of mesh behind spermatic cord. Securing mesh with two interrupted sutures on upper edge and one continuous suture with no more than three to four passes on lower edge of mesh. Keeping mesh with a slightly relaxed, tented up, or dome-shaped configuration. Identification and protection of the ilioinguinal, iliohypogastric, and genital nerves.")
6
Advantages Every type of inguinal hernia Local anesthesia
Easy to learn and perform Low rate of recurrence Gold standard?

7
Disadvantages Postoperative chronic pain Return to daily activity
Higher than TEP or TAPP ? Return to daily activity Later than TEP or TAPP ?

8
TEP Inguinal Hernia Repair
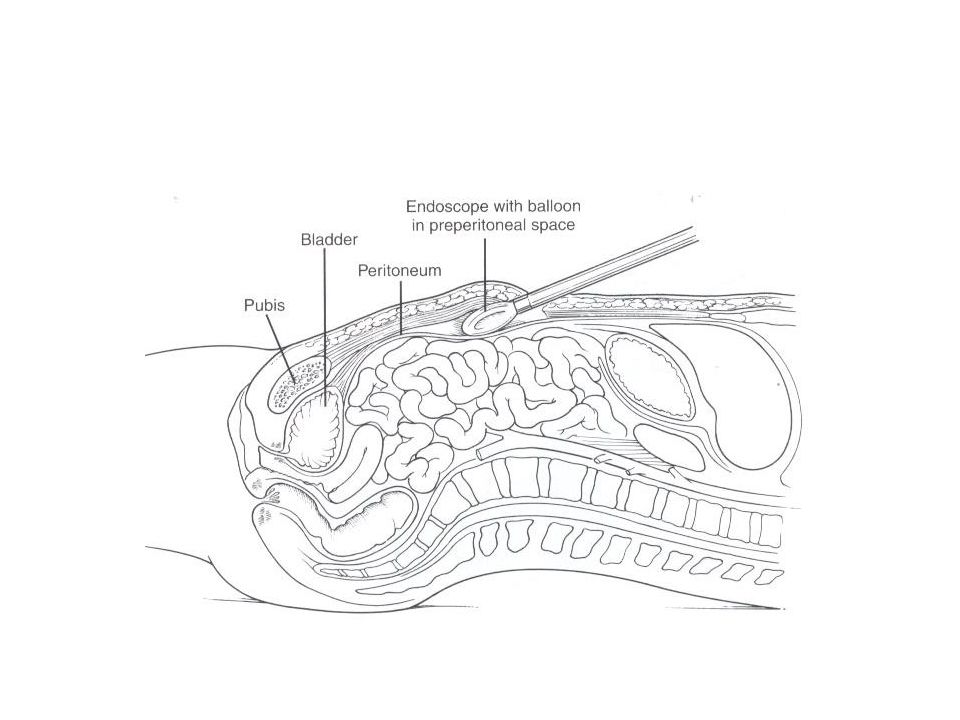
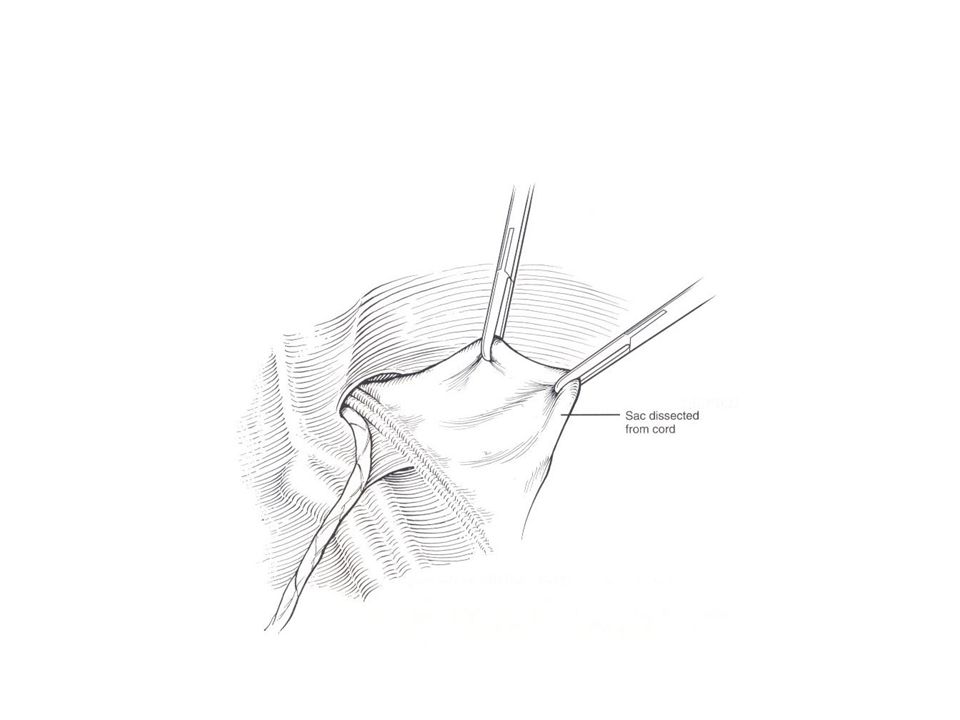
Technique Trocars Direct access of one subumblical 10 mm and two 5 mm at the midline Preperitoneal dissection Dissection of hernial sac Parietalization of spermatic cord and its content Placement of mesh

10
Technical difficulties
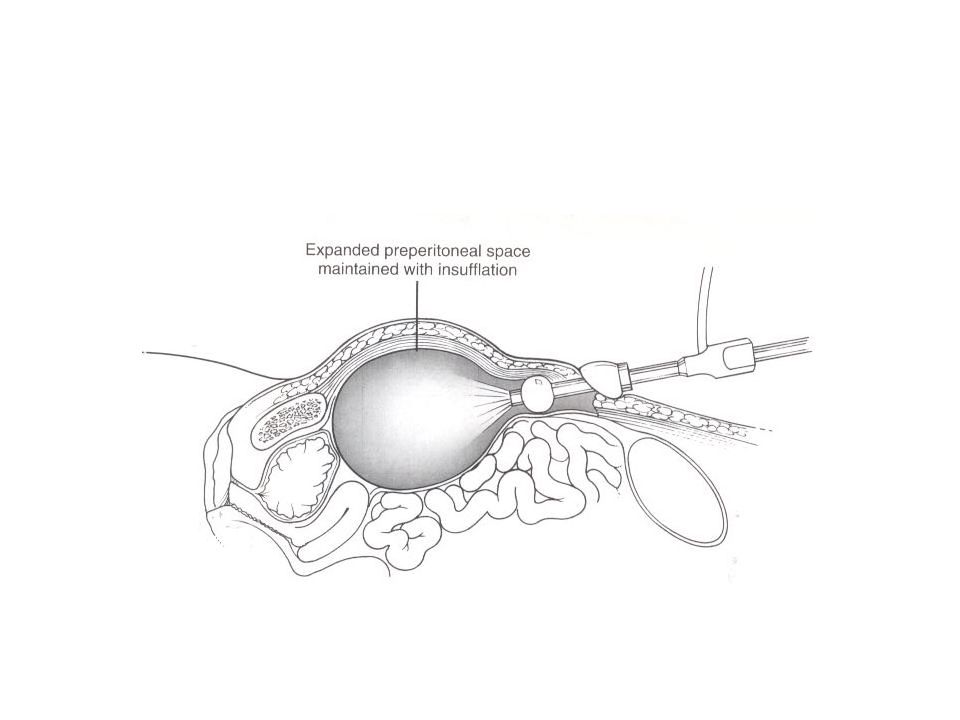
Preperitoneal space creation Baloon dissection in early learning curve besides its cost Peritoneal injury Loss of exposure Closure of defect via pretied suture, loop ligation, endoscopic stapling or endoscopic suturing Port-site closure Closure of fascial defects larger than 10 mm

15
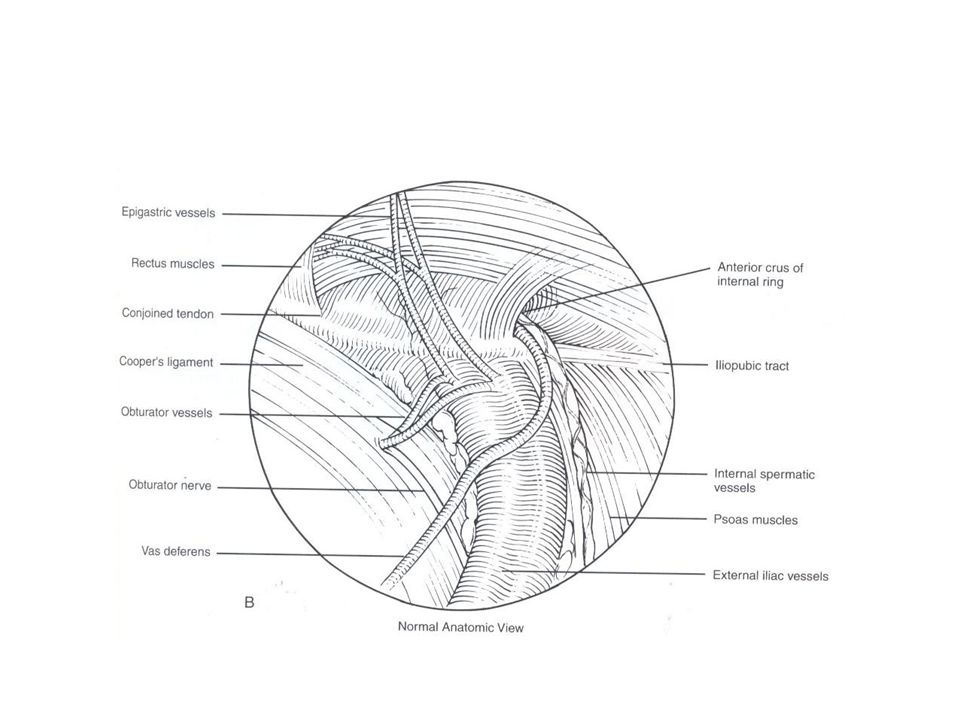
Dissection and Landmarks
Superior Subumblical area Inferior Space of Retzius Inferolateral Psoas muscle and Bogros space Medial Beyond midline Pubic bone Cooper’s ligament Inferior epigastric vessels Cord structures Myopectineal orifice boundaries Fascia over psoas muscle

19
Controversies Preoperative urinary catheterization
Preoperative emptying of urinary bladder by him/herself Catheterization in difficult and long-standing surgery Access for pneumopreperitoneum Subumblical direct trocar vs suprapubic Veress

20
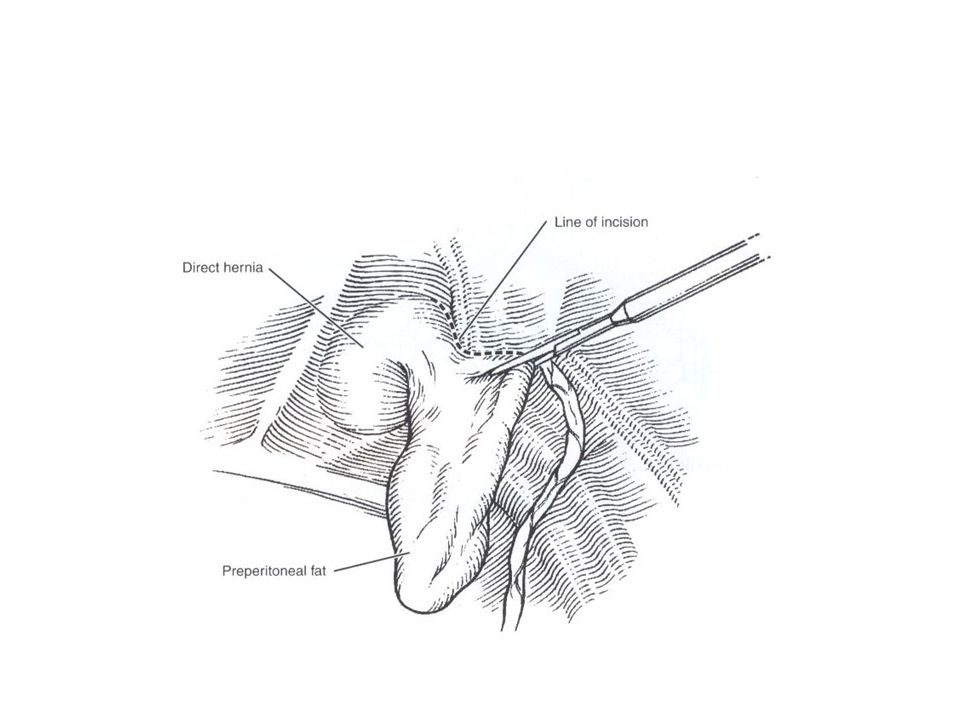
Technical Key Points Inversion and anchoring of direct sac to Cooper’s ligament to decrease risk of seroma and hematoma formation Proximal ligation and distal division of large indirect hernia sac Drains only in selected patients Fixation of mesh in hernias greater than 4 cm

21
Recommendations Larger mesh (12*17 cm) in larger hernia (>3-4 cm)
Stapled fixation of mesh to the symphysis, Cooper’s ligament and rectus muscle in larger direct hernia (>3-4 cm) Overlapping of mesh approximately 1-3 cm lateral to the spina iliaca anterior superior in large indirect hernias (>4-5)
 Overlapping of mesh approximately 1-3 cm lateral to the spina iliaca anterior superior in large indirect hernias (>4-5)")
23
Advantages of TEP repair
Early return to daily activities Low rate of postoperative chronic pain Exploration of contralateral side for hidden hernias ?

24
Disadvantages of TEP repair
General anesthesia; regional anesthesia in selected patients Longer learning curve At least 50 to 60 cases Applicability on incarcerated and scrotal hernias Applicability on patients with previous lower abdominal surgery

25
Learning Curve for TEP repair
Can J Surg, 2012, 55: 33-6 700 patients Learning curve after the first 60 cases A plateau of less than 30 min for duration of surgery A plateau of 1 day for length of stay Conclusion: learning curve for TEP hernia repair as 60 cases for a beginner surgeon

Similar presentations