Download presentation
Presentation is loading. Please wait.

1
Managing Seizure Patients in the Emergency Department Managing Seizure Patients in the Emergency Department James Wheless, MD Director, Texas Comprehensive Epilepsy Program University of Texas - Houston James Wheless, MD Director, Texas Comprehensive Epilepsy Program University of Texas - Houston

2
Question #1: When is an antiepileptic drug (AED) loading dose necessary? Question #1: When is an antiepileptic drug (AED) loading dose necessary?
 loading dose necessary .")
3
Acute Seizures That Need a Loading Dose Seizures secondary to partial compliance Dose (mg) = weight (Kg) x V D (L/Kg) x D Cp (mg/dL) Seizures with a high rate of recurrence (Some seizures are like potato chips: you can never have just one!!) Seizures secondary to partial compliance Dose (mg) = weight (Kg) x V D (L/Kg) x D Cp (mg/dL) Seizures with a high rate of recurrence (Some seizures are like potato chips: you can never have just one!!) Myoclonic, tonic, absence, atonic
 = weight (Kg) x V D (L/Kg) x D Cp (mg/dL) Seizures with a high rate of recurrence (Some seizures are like potato chips: you can never have just one!!) Seizures secondary to partial compliance Dose (mg) = weight (Kg) x V D (L/Kg) x D Cp (mg/dL) Seizures with a high rate of recurrence (Some seizures are like potato chips: you can never have just one!!) Myoclonic, tonic, absence, atonic")
4
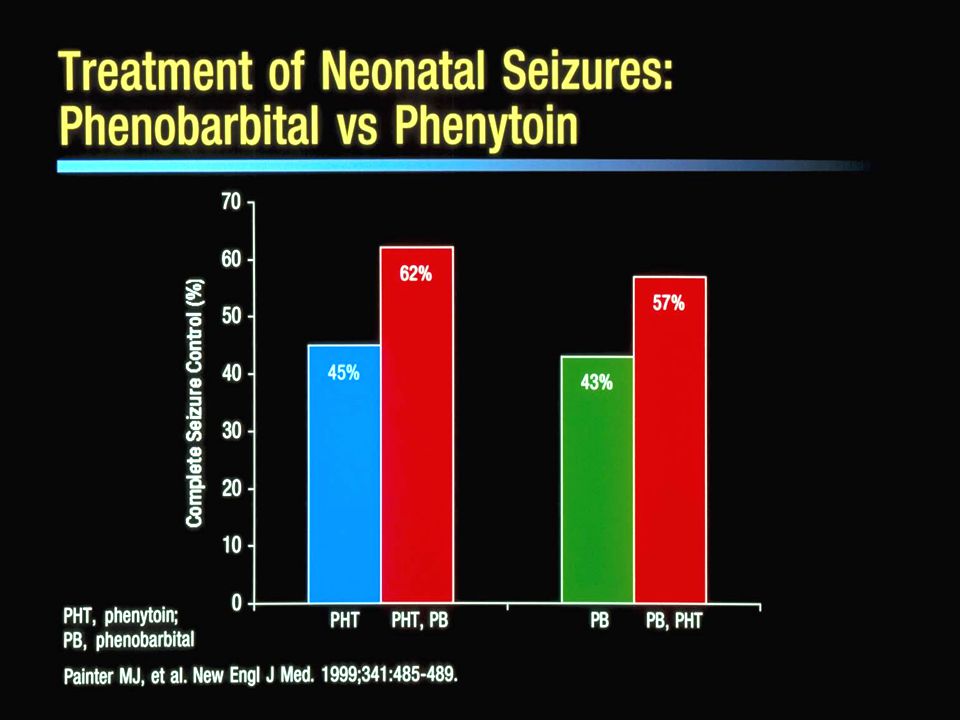
Acute Seizures That Need a Loading Dose Progressive neurologic disease Acute symptomatic seizures New onset adult seizures Status epilepticus – depends on etiology (febrile status epilepticus- probably not) Neonatal seizures Progressive neurologic disease Acute symptomatic seizures New onset adult seizures Status epilepticus – depends on etiology (febrile status epilepticus- probably not) Neonatal seizures
 Neonatal seizures Progressive neurologic disease Acute symptomatic seizures New onset adult seizures Status epilepticus – depends on etiology (febrile status epilepticus- probably not) Neonatal seizures")
5
Acute Seizures That May Not Need a Loading Dose New onset pediatric complex partial, generalized tonic-clonic seizures (not status epilepticus) Febrile seizures Some acute symptomatic seizures (i.e., decreased blood sugar) New onset pediatric complex partial, generalized tonic-clonic seizures (not status epilepticus) Febrile seizures Some acute symptomatic seizures (i.e., decreased blood sugar)
 Febrile seizures Some acute symptomatic seizures (i.e., decreased blood sugar) New onset pediatric complex partial, generalized tonic-clonic seizures (not status epilepticus) Febrile seizures Some acute symptomatic seizures (i.e., decreased blood sugar)")
6
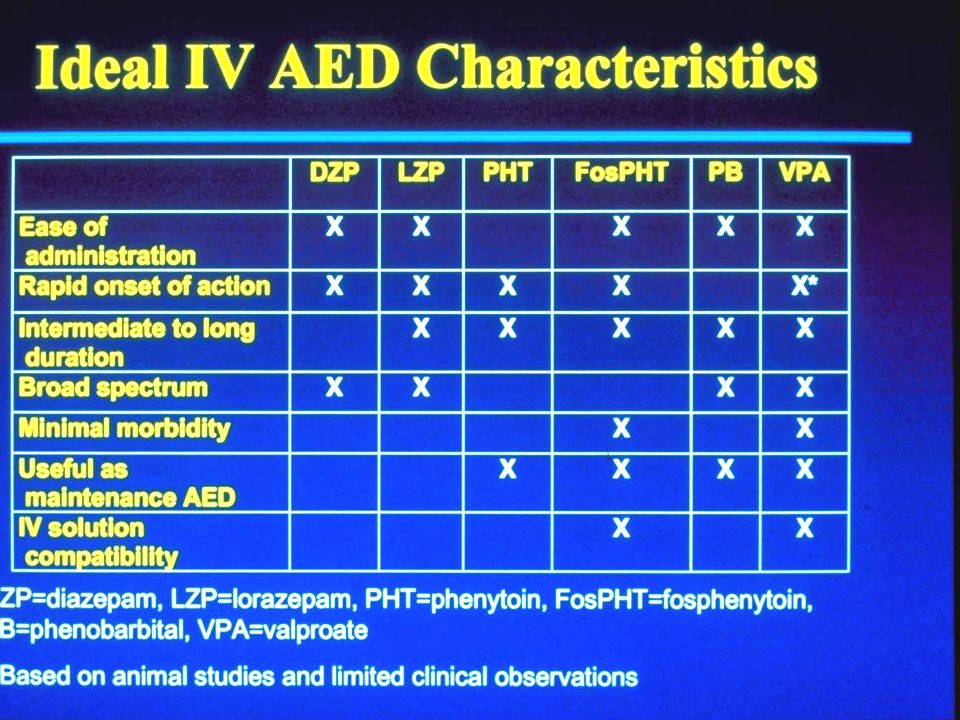
Question #2: What medications are best for an AED loading dose? Question #2: What medications are best for an AED loading dose?

8
Question #3: What is the empirical therapy for acute seizures? Question #3: What is the empirical therapy for acute seizures?

18
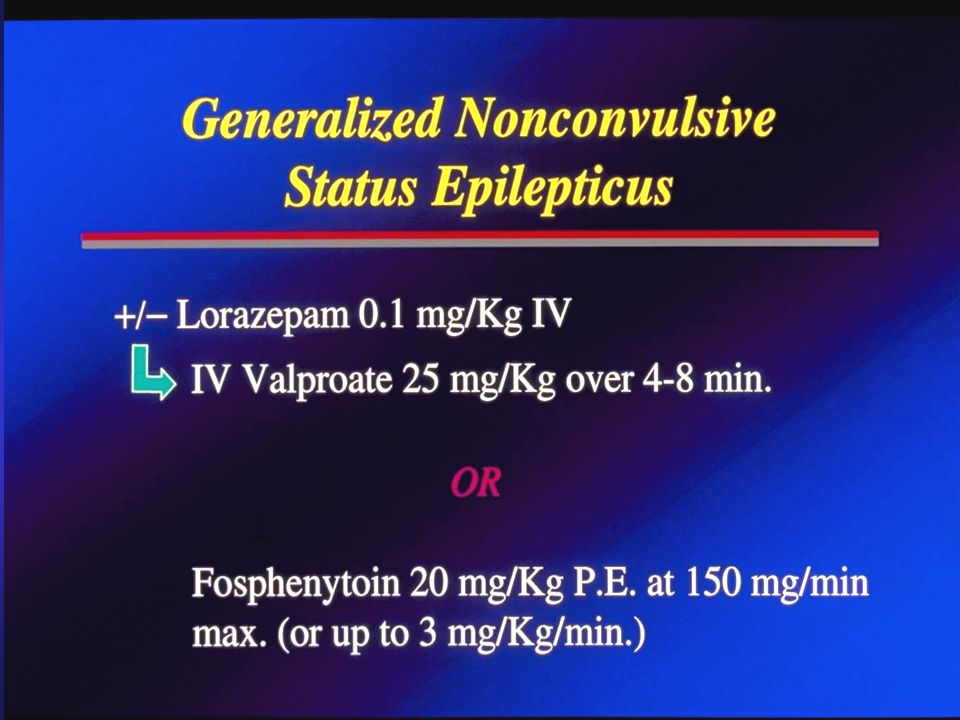
Question #4: What antiepileptic drugs are useful for nonconvulsive status epilepticus (SE) (altered mental status presenting as SE)? Question #4: What antiepileptic drugs are useful for nonconvulsive status epilepticus (SE) (altered mental status presenting as SE)?
 (altered mental status presenting as SE) .")
24
Question #5: When do we use: 1. Fosphenytoin? 2. Phenobarbital? 3. IV Valproate? Question #5: When do we use: 1. Fosphenytoin? 2. Phenobarbital? 3. IV Valproate?

39
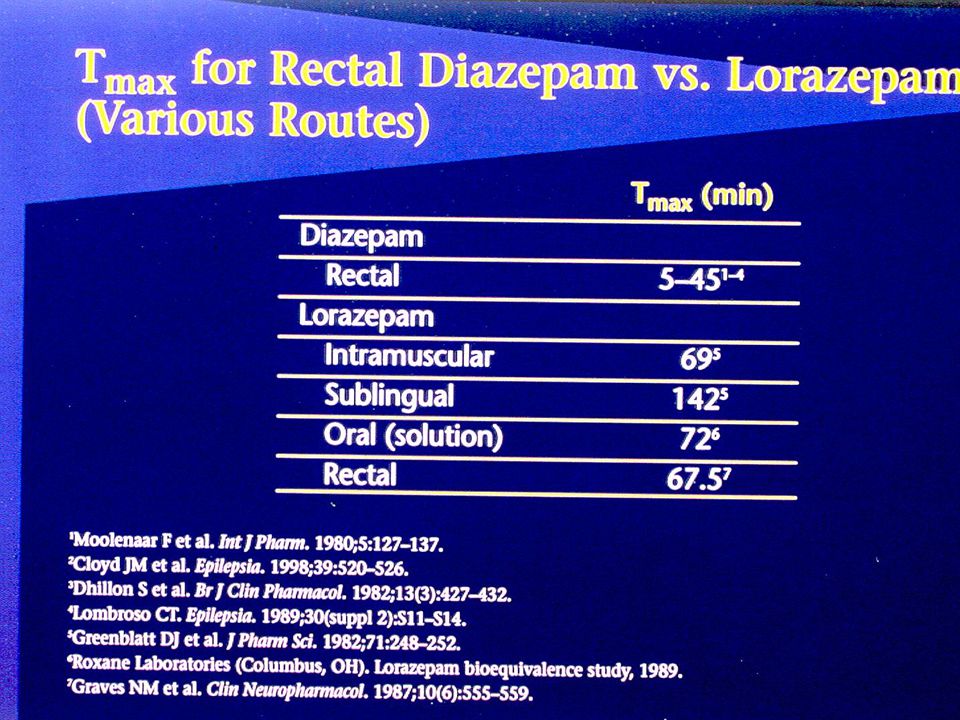
Question #6: What parenteral medications can be given if no IV access is available? Question #6: What parenteral medications can be given if no IV access is available?

43
Development of a Rapid- Onset Intranasal Delivery of Diazepam Effective nasal delivery volume < 300ml (150ml/nostril) Ethyl laurate-based microemulsion developed Diazepam solubility in microemulsion is 41 mg/ml Bioavailability = ½ of IV diazepam Maximum plasma concentration reached in 2-3 min. Li L et al (B M Squibb), Int. J. Pharm., 2002, 237 (1-2): 77-85 Effective nasal delivery volume < 300ml (150ml/nostril) Ethyl laurate-based microemulsion developed Diazepam solubility in microemulsion is 41 mg/ml Bioavailability = ½ of IV diazepam Maximum plasma concentration reached in 2-3 min. Li L et al (B M Squibb), Int. J. Pharm., 2002, 237 (1-2): 77-85
, Int. J. Pharm., 2002, 237 (1-2): Effective nasal delivery volume < 300ml (150ml/nostril) Ethyl laurate-based microemulsion developed Diazepam solubility in microemulsion is 41 mg/ml Bioavailability = ½ of IV diazepam Maximum plasma concentration reached in 2-3 min. Li L et al (B M Squibb), Int. J. Pharm., 2002, 237 (1-2):")
44
Pediatric Status Epilepticus: IM Midazolam Children (N = 48) 4 mo.- 14 yrs. (69 episodes) Midazolam 0.2 mg/Kg IM in ER 35 seizures 10-20 min., 34 > 20 min. duration at presentation in ER Results: 57 episodes (83%) stopped in 1-5 min. 7 episodes (10%) stopped in 5-10 min. Lahat E et al, Pediatric Neurology, 1992; 8: 215-216 Children (N = 48) 4 mo.- 14 yrs. (69 episodes) Midazolam 0.2 mg/Kg IM in ER 35 seizures 10-20 min., 34 > 20 min. duration at presentation in ER Results: 57 episodes (83%) stopped in 1-5 min. 7 episodes (10%) stopped in 5-10 min. Lahat E et al, Pediatric Neurology, 1992; 8: 215-216
 Midazolam 0.2 mg/Kg IM in ER 35 seizures min., 34 > 20 min. duration at presentation in ER Results: 57 episodes (83%) stopped in 1-5 min. 7 episodes (10%) stopped in 5-10 min. Lahat E et al, Pediatric Neurology, 1992; 8: Children (N = 48) 4 mo.- 14 yrs. (69 episodes) Midazolam 0.2 mg/Kg IM in ER 35 seizures min., 34 > 20 min. duration at presentation in ER Results: 57 episodes (83%) stopped in 1-5 min. 7 episodes (10%) stopped in 5-10 min. Lahat E et al, Pediatric Neurology, 1992; 8:")
46
Chaimberlain JM, Pediatric Emerg. Care, 1997;13, 92

50
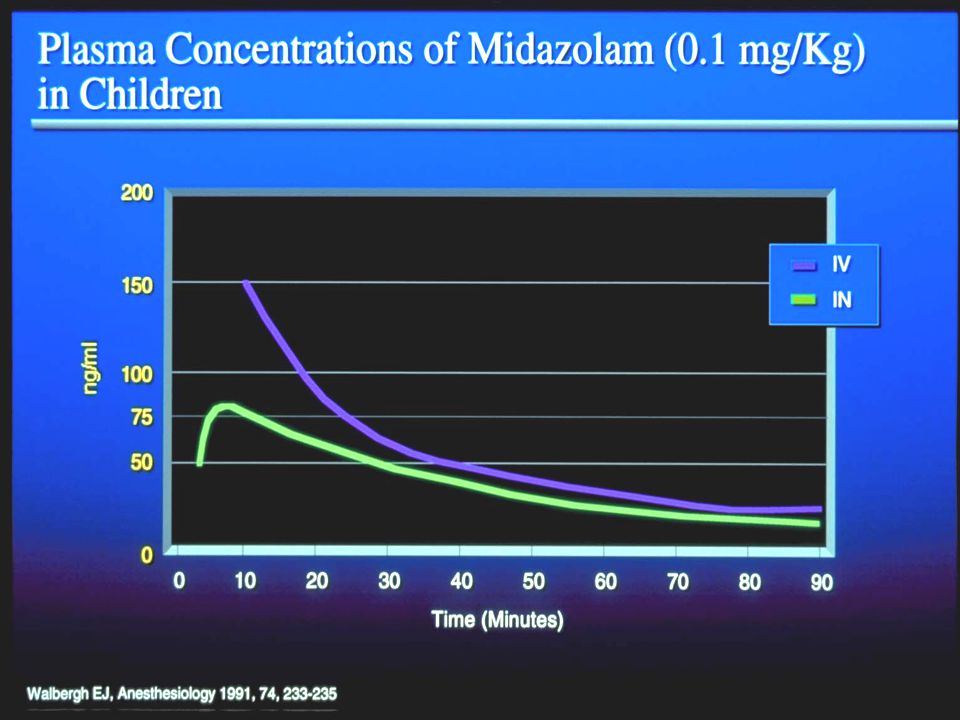
Pharmacokinetics of Midazolam by Intranasal (IN) Administration Subjects (6) had irritation, general discomfort Suggested doses for status epilepticus: - children 0.2 mg/Kg IN - adults5-10 mg IN Parenteral midazolam 5 mg/ml Mean peak plasma conc. reached 14 min. (+5) Mean bioavailability 0.83 (+0.19) IN Knoester PD et al, Br. J. Clin. Pharmacol., 2002; 53(5): 501-507 Subjects (6) had irritation, general discomfort Suggested doses for status epilepticus: - children 0.2 mg/Kg IN - adults5-10 mg IN Parenteral midazolam 5 mg/ml Mean peak plasma conc. reached 14 min. (+5) Mean bioavailability 0.83 (+0.19) IN Knoester PD et al, Br. J. Clin. Pharmacol., 2002; 53(5): 501-507
 Mean bioavailability 0.83 (+0.19) IN Knoester PD et al, Br. J. Clin. Pharmacol., 2002; 53(5): Subjects (6) had irritation, general discomfort Suggested doses for status epilepticus: - children 0.2 mg/Kg IN - adults5-10 mg IN Parenteral midazolam 5 mg/ml Mean peak plasma conc. reached 14 min. (+5) Mean bioavailability 0.83 (+0.19) IN Knoester PD et al, Br. J. Clin. Pharmacol., 2002; 53(5):")
56
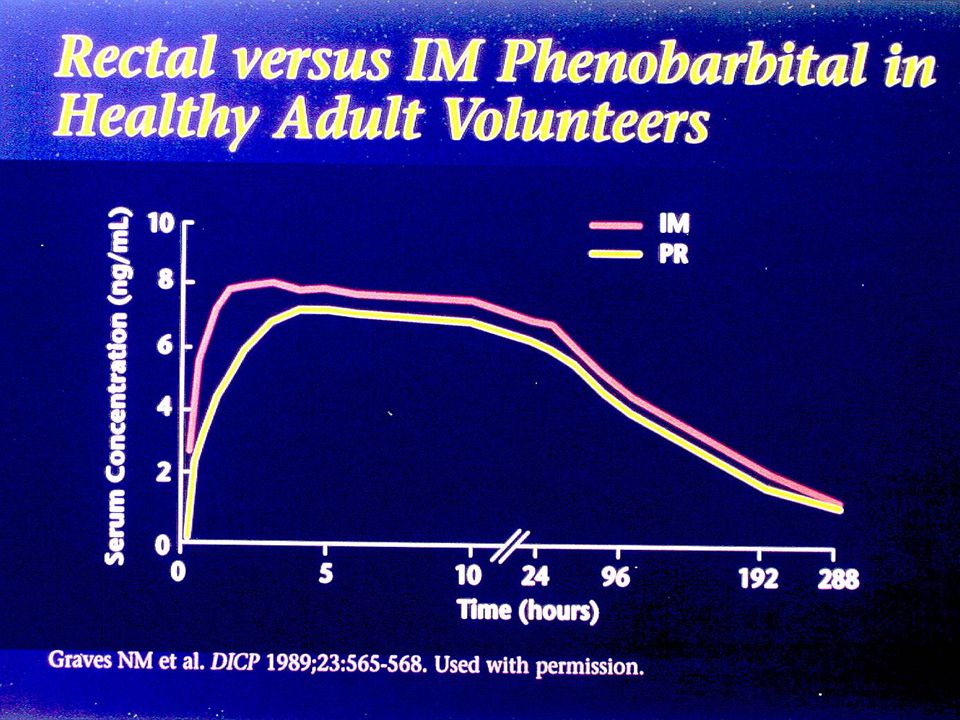
Parenteral Formulation to Avoid for IM Use Depacon (IV Valproate) IM – muscle necrosis Phenytoin IM – muscle necrosis Phenobarbital slow onset Depacon (IV Valproate) IM – muscle necrosis Phenytoin IM – muscle necrosis Phenobarbital slow onset
 IM – muscle necrosis Phenytoin IM – muscle necrosis Phenobarbital slow onset Depacon (IV Valproate) IM – muscle necrosis Phenytoin IM – muscle necrosis Phenobarbital slow onset")
58
Question #7: How do pediatric and adult cases of acute seizures and status epilepticus differ? Question #7: How do pediatric and adult cases of acute seizures and status epilepticus differ?

Similar presentations