Download presentation
Presentation is loading. Please wait.

1
I-CAN v4.1 www.i-can.org.au This is an old presentation! Check out our latest work at www.i-can.org.au

2
Acknowledgements Aussies: Vivienne Riches, Trevor Parmenter, Samuel Arnold, Roger Stancliffe, Gwynnyth Llewellyn, Keith McVilly, Jeffrey Chan, Gabrielle Hindmarsh, Julie Pryor, Tony Harman (and many others) POMs: Helen Sanderson, Edwin Jones, David Felce, Sandy Toogood, Jim Mansell and colleagues Yanks: Michael Smull, John O’Brien, Marc Gold, AAIDD WHO ICF
 POMs: Helen Sanderson, Edwin Jones, David Felce, Sandy Toogood, Jim Mansell and colleagues Yanks: Michael Smull, John O’Brien, Marc Gold, AAIDD WHO ICF")
3
Ice-breaker Credo for Support What is the I-CAN Theoretical models A New Way to do Assessment A screenshot or two Dreams, Goals and I Can statements Case Examples and some other tidbits Possible Future Projects Lots of Discussion In today’s semi-structured workshop:

4
7.5 Minutes TOTAL Find someone who you don’t know, ideally who isn’t from your organisation (2.5 minutes max) Interview your new friend - fill out on PAGE 2 the ‘About me’, ‘Long term goals, dreams and aspirations’ and ‘Current Life Situation’ boxes (2.5 minutes) for your new friend Swap GO! ICE BREAKER

5
Credo for Support Download me from Youtube

6
Why do we need assessments, models, classifications? In a perfect world we would prefer to have no classification at all. However, for the purposes of statistics, assessment for services and programs and above all for non- discrimination legislation, we do need to have a definition of who we are and of our situation and we reluctantly accept that this means some sort of classification or analysis of disablement. Rachel Hurst of Disabled Peoples International (1998) cited in ICF Australian User Guide v1 section 3.2
 cited in ICF Australian User Guide v1 section 3.2.")
7
What is the I-CAN? The Instrument for the Classification and Assessment of Support Needs (I-CAN) “a support needs assessment designed to assess and guide support delivery for people with a disability including mental illness. It provides a user, client, staff and family friendly holistic assessment, conceptually based upon the internationally recognized WHO ICF framework.”
 a support needs assessment designed to assess and guide support delivery for people with a disability including mental illness. It provides a user, client, staff and family friendly holistic assessment, conceptually based upon the internationally recognized WHO ICF framework. .")
8
Project in the ACT (started in 1998) to develop a resource allocation tool for assessing and classifying support needs of people with an intellectual disability prior to determining funding needs SCAN Supports Classification and Assessment of Needs A Bit of History
 to develop a resource allocation tool for assessing and classifying support needs of people with an intellectual disability prior to determining funding needs SCAN Supports Classification and Assessment of Needs A Bit of History")
9
ARC linkage funding over 3 years to develop an instrument to assess & classify support needs administered by the University of Sydney with CDDS and ROYAL REHAB as industry partners Over 5000 participants in trials of first three versions, n = 1012 assessments completed. Ongoing revisions based upon: Factor Analysis Validity and reliability studies Feedback (what’s missing?) Ongoing review of the WHO ICF framework (WHO, 2001) Our History
 Ongoing review of the WHO ICF framework (WHO, 2001) Our History.")
10
I-CAN Theoretical Models Or how to describe humans with boxes and arrows.

11
World Health Organisation’s (WHO) International Classification of Functioning, Disability & Health (ICF) Bio-psycho-social model Person-environment interaction (the little red book)
 International Classification of Functioning, Disability & Health (ICF) Bio-psycho-social model Person-environment interaction (the little red book)")
13
The Hotel Model AVOID AT ALL COSTS! Residents are spectators in their own lives. Staff feel like glorified domestics. Staff Residents Essential to link support needs assessment with Active Support the question is NOT how much support would this person need to live in a hotel

15
The Active Support Model People participate in everyday activities with support Support can close the gap between what people can do and what is needed – that’s the type of support we need to be measuring!

16
Health Condition (disorder/disease) I-CAN is based on the WHO ICF framework Environmental Factors Personal Factors Body function&structure (Impairment) Activities(Limitation)Participation(Restriction)
 I-CAN is based on the WHO ICF framework Environmental Factors Personal Factors Body function&structure (Impairment) Activities(Limitation)Participation(Restriction)")
17
The AAIDD 2002 Theoretical Model I. Intellectual Abilities II. Adaptive Behaviour III. Participation, Interactions, Social Roles IV. Health & Etiology V. Context Individual Functioning Supports

18
Diagnosis of Intellectual Disability requires 1. IQ Assessment 2. Adaptive Behavior Assessment 3. Support Needs Assessment Support Needs – Redefining our definition of Intellectual Disability

19
A Synthesis of Models I-CAN is based on philosophical, theoretical and practical levels, of the ICF, AAIDD Model, Active Support, Person-centred thinking & strengths focus Active Support demands a focus on the engagement and empowerment of the person with disability AAIDD 2002 model demands a new conceptualization in the way we conduct assessment, with a focus on support need not deficit or medical diagnosis ICF demands a holistic health informatics system, based in biopsychosocial philosophy, that considers facilitators and barriers to everyday life Person-centeredness demands the person with disability is present and drives their assessment wherever possible, with a focus on individualised supports Strengths focused demands a focus on empowerment with the right support, not a mere list of deficits

20
The (proposed) I-CAN Theoretical Model Environment Supports Person Disablement
 I-CAN Theoretical Model Environment Supports Person Disablement")
21
The I-CAN Theoretical Model – ‘People are not boxes’ version EnvironmentSupports Disablement a human condition, not a category Person

22
The I-CAN Theoretical Model – ‘We are all people’ version EnvironmentSupports Disablement a human condition, not a category Person The Human Experience (the supports continuum)
")
23
The Amount of Support we Need How old we are and what’s going on in our life The Supports Continuum Rug rat Here comes dementia Midlife Crisis Car Accident

24
The I-CAN Theoretical Model – Mapping it out, v1.03 Physical Health Mental Emotional Health Behavioural Concerns Activities Participation Barriers Limitations Attitudes (in) Society Culture Built Environment, Natural Environment (pollution) Political / Economic Family / Friends Technological Historical Supports People (Family, Friends, Community Members, Staff, Health Professionals), Training, Technical Aids, Equipment… Commerce, Industry Person Environment Personal Factors
 Society Culture Built Environment, Natural Environment (pollution) Political / Economic Family / Friends Technological Historical Supports People (Family, Friends, Community Members, Staff, Health Professionals), Training, Technical Aids, Equipment… Commerce, Industry Person Environment Personal Factors")
25
Another way to perceive it? Person Supports Environment

26
Person in the centre Person Support Environment Support Environment

27
At a societal, rather than individual level People Supports Society Support Systems Other people Environment Everything else (archetypes)
")
28
Gestalt… Person Human Relationships Society Contact Boundary Everything else in my contact boundary that isn’t human Environment Everything Else (archetypes, my story) The focus is a person’s life, supportive human relationships, and the political, economic and cultural world the person lives in. The emphasis is no longer health, disability and functioning. Human relationships is key to the work

29
Hmmm a simplified model needs a new name… “All you need is love” - no no, not technical enough, already copyrighted! “All you need is support” - no no, not catchy

30
International Classification of Functioning, Disability and Health OR International Classification of People, the Support they Need, and the Environment

31
A model illustrating a system that aligns different levels of support around the person with a disability (reproduced and slightly adapted from Gillenson, Green & Miller, 2005)
")
32
The Supports Paradigm Historically, support had a narrow meaning in the human service system that was synonymous with services. The role of supports in human services has gradually evolved from a primary emphasis on caretaking, to a developmental model emphasizing rehabilitation services, to the current paradigm that embraces a broad view of support that is more consistent with the generic definition. Bradley (1994a, 1994b) characterised these phases as encompassing (a) an era of dependence and segregation, (b) an era of deinstitutionalisation and community development that still emphasized specialized services, and (c) an era of community membership. This third phase marks a shift to a primary focus on personal outcomes, such as friendships, personal fulfilment, and self-determination. The importance and power of social relationships in determining a person's quality of life help define the nature of support in this new paradigm (Schalock, 1995; Snell & Vogtle, 1997). Schalock, R. L., Baker, P. C. & Croser, D. (2002). Embarking on a New Century: Mental Retardation at the End of the 20th Century. AAMR
 characterised these phases as encompassing (a) an era of dependence and segregation, (b) an era of deinstitutionalisation and community development that still emphasized specialized services, and (c) an era of community membership. This third phase marks a shift to a primary focus on personal outcomes, such as friendships, personal fulfilment, and self-determination. The importance and power of social relationships in determining a person s quality of life help define the nature of support in this new paradigm (Schalock, 1995; Snell & Vogtle, 1997). Schalock, R. L., Baker, P. C. & Croser, D. (2002). Embarking on a New Century: Mental Retardation at the End of the 20th Century. AAMR.")
33
A New Way to do Assessments Adaptive Behavior and Functional Limitation Vs. Support Needs

34
Support needs assessments are “developed on the assumption that a direct measure of support needs will provide more specific and direct information and therefore will be more useful for planning teams and those in systems-level supports management who try to determine how best to support an individual in community settings” (Thompson et al., 2004, p.10). Functional Assessment vs. Support Needs Assessment Deficit Assessment vs. Empowerment Assessment

35
The questions we use to ask were: Can you count change? Can you climb a ladder? Now we are asking: How much support do you need to go to the shops? If you wanted to climb a ladder, how much support would you need? I don’t get it – what’s so different about assessing support needs instead of assessing adaptive behavior or functioning?

36
Support needs assessments tend to be focused on resource allocation, should the focus instead be supports planning and support delivery?? Are we missing the forest for the trees??

37
Most Assessments ‘Professional’ conducts interview, fills out assessment form (30-90 minutes) ‘Professional’ scores assessment form (10-60 minutes) You are a 7 (of 9) ‘Professional’ writes up report trying to explain why you are a 7 (of 9) (takes 1-3 hours, if you are lucky you will get a report in 1- 2 weeks)
 ‘Professional’ scores assessment form (10-60 minutes) You are a 7 (of 9) ‘Professional’ writes up report trying to explain why you are a 7 (of 9) (takes 1-3 hours, if you are lucky you will get a report in 1- 2 weeks)")
38
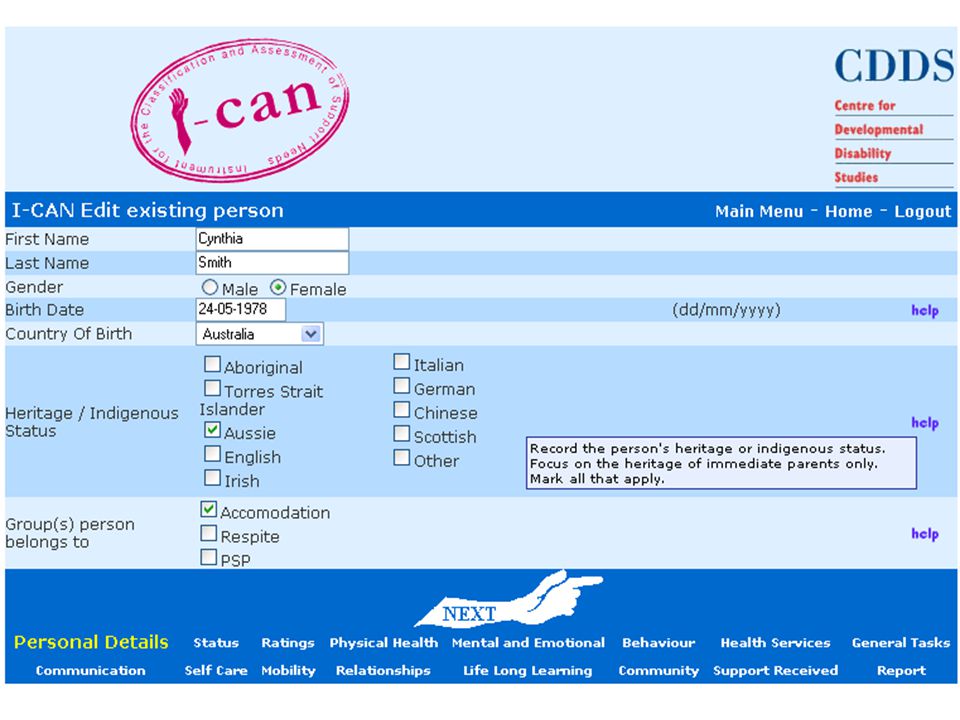
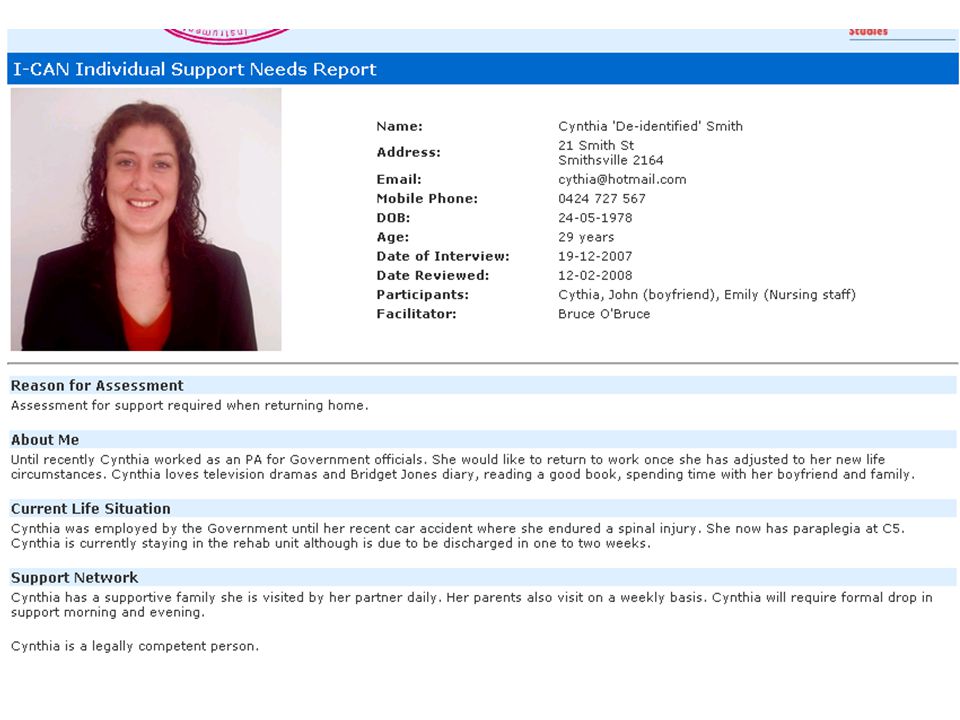
Doing an I-CAN online Trained Facilitator guides Person with disability, family and support persons through a semi- structured self- assessment process (1-2 hours approx.) Website scores assessment and generates comprehensive report in seconds You receive a report that explains a bit about who you are, and comprehensively describes the supports you need Caregivers, support persons and health professionals will find this report very useful
 Website scores assessment and generates comprehensive report in seconds You receive a report that explains a bit about who you are, and comprehensively describes the supports you need Caregivers, support persons and health professionals will find this report very useful")
39
Fitting the jigsaw together Closing the Gap

40
Government Eligibility Resource Allocation Monitor trends / needs Psychologists Conceptualization of support need – how do we measure it? Good clinical assessment tool Researchers Comprehensive, valid data Statistical linkage keys Health Professionals Accurate, concise, up to date health information required for decision making Direct Support Professionals Info of what support to provide and how to provide it Service Providers Paperless office systems and client databases Methods to ensure quality and to meet compliance Person with disability and their family Quality support when and how I want and need it Support to achieve my dreams, as well as the day to day stuff

41
Reproduced with permission from Shaddock, A. (2007). Mainstream Mindsets for Resilient Services: or, “How to Get into Shape by Getting Rid of Normal Curves”. Intellectual Disability Australia, 28(3), 3-10.
,")
43
I-CAN v4.1

44
Version 4.1 – web based assessment e-Health, telemedicine, telepsychology Can be completed on or offline Comprehensive Individual Support Needs Report Additional online functions include: Upload a photo! Custom Summary Report National Minimum Data Set (NMDS) export Excel export (import into SPSS) Comparison of small groups’ scores Track changes over time Cost Estimation Tool Where are we now?
 export Excel export (import into SPSS) Comparison of small groups’ scores Track changes over time Cost Estimation Tool Where are we now .")
70
Concurrent / Multiple Ratings…

72
First draft!

74
Dreams, Goals and I Can Statements

76
Don’t take away a person’s dream even if it seems like it can never be achieved – write it down

77
An I can statement Instead of writing ‘Bob can’t count change’ (an I can’t statement) Simply try ‘Bob can use a dollar more strategy and make purchases with supervision’ I-can’t: (name) cant (do this) I-can: (name) with (type of) support can (do this)
 Simply try ‘Bob can use a dollar more strategy and make purchases with supervision’ I-can’t: (name) cant (do this) I-can: (name) with (type of) support can (do this)")
78
Let’s turn those I can’t statements upside down! ‘John can’t tie shoelaces’ ‘Judy can’t catch the bus unless she has been on it before’ ‘Robert can’t dress himself’

79
Lets talk about Goals… Firstly and most importantly; “Bob’s goals is to…” “Our goal is for Bob to…” Important To or Important For* *credit going to originators of person-centered planning for their work on goal setting

80
Goals, Goals, Goals Some types of goals... Skill building: “Bob’s goal is to independently cook stir-fry, he is going to practice cooking with supervision from staff three times each week” Management: “Our goal is to ensure Bob does not eat excessive amounts of takeaway pizza, we will support Bob to cook three times each week” Maintenance: “Our goal is to ensure Bob retains his cooking skills by having the opportunity to cook a variety of dinners three times each week”

81
Clear Specific Activities vs Fuzzy Statements* *Credit goes to Active Support authors for Specifics vs. Fuzzies

82
Fuzzies and Clear Specific Activities Fuzzy statements are vague and open to interpretation (and misinterpretation). Clear activity statements are specific and unambiguous descriptions of what behaviour is expected (of clients & staff).
..")
83
Fuzzy & Clear Specific Activities Jane will understand numbers. Bill will be friendly. Nicole will listen carefully. Joe will be affectionate. Jane will count six items. Bill will smile when greeting strangers. Nicole will repeat four words. Joe will hug his mum.

84
e.g., Matthew will: FUZZIES learn to toast bread choose what to put on his toast develop competency in domestic tasks CLEAR SPECIFIC ACTIVITIES place 2 slices of bread in the toaster each morning and switch it on select one of two spreads offered to him each morning vacuum the lounge twice a week

85
Fuzzies & Clear Specific Activities Understand Co-operate Really understand Think Share Listen Happy Affectionate Mobile Withdrawn Disruptive Challenging Match two identical items Wait in a queue Match two identical items Add two single digit numbers Take turns Maintain eye contact Smile Hold hands Walk Looking down Throw furniture Punch self

86
SMART MEN* goals MEN goals M = morning E = evening N = night SMART goals S = specific M= measurable A = achievable R = relevant T = time-limited *Credit goes to Julie Pryor for SMART MEN goals

87
Some nursing examples of SMART MEN goals Mrs Davis will don her lower limb prosthesis with step by step verbal instructions within 15 minutes within 5 days. Mr Singh will transfer safely from wheelchair to bed using a slide board with standby supervision between 9pm and 10pm each evening. Miss Chu will have no more than two cigarettes between 9pm and 6am. *Credit goes to Julie Pryor for these examples

88
Sequence goals in a logical order Identify the overall aim: Joan will learn to manage her long term catheter using techniques that will prevent infection. Joan will commence by learning to change her night drainage bag to a day bag in the morning. Joan will progress to learn how to empty her catheter bag and change to a night bag in the evening. *Credit goes to Julie Pryor for these examples

89
Writing a clear specific goal Who, will do what, with what help, how often and how well.

90
Yay an exercise! Lets write some goals! 1.Domestic 2.Community 3.Social

91
Testing the Adequacy of Clear Specific Activities The Man from Mars Test – could the MfM implement the goal from its written description alone? The ‘Hey Dad’ Test – can you prefix ‘Hey Dad, come and see me ________’, and it still make sense?

92
Goals in the I-CAN It’s ok for Long team Goals, Dreams and Aspirations to be a little fuzzy Elsewhere in the I-CAN, try to be a bit more specific regarding what the goal is –within reason, you may not have time to write SMART MEN, but hopefully goals written won’t all be warm fuzzies –It may not be appropriate to write an ‘I can’ statement and identify ‘goals’ in response to every question of the I-CAN. In some cases you may not even be identifying ‘My Support Needs’, you may just be giving some background info and scoring ‘N/A’ –It’s up to the facilitator and people involved in the assessment to figure out the best things to put down to get a clear, positive and proactive report. Identifying goals and I can statements can make things happen.

93
Fellow living in institutional setting who required very little support Fellow known to a support service for many years, during I-CAN group interview process family member identified cause of a challenging behaviour unknown to staff Bringing allied health teams together Case Examples of the benefit of comprehensive support needs assessment

94
Moderate Intellectual Disability OR Person with an Intellectual Disability and Limited Support Needs Does everyone have autism these days? Inclusion of ‘query only’ checkbox for the diagnoses section Case Examples of the benefit of comprehensive support needs assessment

95
*Credit to Anthony Shaddock

96
Progress on SNAP comparison… n=38, 24 male 14 female, mostly people with a high level of support need, every person recorded multiple support needs. One fellow has 3 SNAPs completed as family were continually unhappy with the assessment outcome Unfortunately had to use SNAP raw scores for most calculations, could not afford $88 per assessment to have them scored Overall significant correlation with higher overall SNAP scores correlated to higher overall I-CAN scores, at the 0.5 level when controlled for age The SNAP overall score correlated specifically with the I-CAN Mobility and Physical health domains only Combined I-CAN Health & Well-Being Scales correlated with SNAP Total score and behaviour support, whereas the I-CAN Activities and Participation Scales only correlated with SNAP behaviour support This and other correlations (too many for a presentation, will be written up soon) lead us to conclude the I-CAN is more holistic in the areas it assesses as support needs, whereas the SNAP may be more focused on physical health.
 lead us to conclude the I-CAN is more holistic in the areas it assesses as support needs, whereas the SNAP may be more focused on physical health..")
97
Similar cost or more expensive for other support needs / adaptive behavior assessments, that will turn the people you support into a number. Costs of not doing a comprehensive assessment: Person-Centred Planning can lose its direction No way to track changes over time Haphazard identification of people in need of additional supports Haphazard identification of outcome of skills building programs Support Needs may go unaddressed, people get sick, or miss out on opportunities, goals and dreams Cost of poorly organized documentation Staff don’t know what to do Documents and information gets lost, people suffer I could go on Cost of not using the I-CAN

98
Many, many, many possibilities that could be explored coming from the I-CAN, and the synthesis of the ICF, Active Support and AAIDD 2002 models. Trying to close the gap between the multiple goals of various stakeholders, is the next step for the I-CAN to grow from a support needs assessment to a health informatics client database? Is this where a combination of the AAIDD 2002 model and the ICF leads us? Resources and time available will tell Possible Futures

99
Possible future projects ProjectDifficultyResources required Output PDF reports Very Easy -Still- waiting on third party software provider Output pre-completed DADHC-style risk assessment Easy Psychologist / Computer programmer time Allow recording of Pension number weight etc / Output Emergency Hospital Admission Form Easy Psychologist / Computer programmer time

100
Possible futures ProjectDifficultyResources required Allow online document storage / paperless office systems / health info management / client database Medium Additional programmer and webserver Standardization Medium-Hard More data (ideally), Researchers, some programming Standardization across various disability groups Medium-Hard As above + LOTS more data
, Researchers, some programming Standardization across various disability groups Medium-Hard As above + LOTS more data")
101
Possible futures ProjectDifficultyResources required 100% Audit Trail, 100% Data Redundancy, 99% Uptime Medium-Hard Additional webserver(s) and programmer Additional Work Skills Training Needs Assessments / PSP Assessments Medium-Hard Additional programmer, lots of Senior Research / Psychologist experience & creativity Annual Health Check module Medium Additional programmer, lots of Specialist Dr assistance, field testing
 and programmer Additional Work Skills Training Needs Assessments / PSP Assessments Medium-Hard Additional programmer, lots of Senior Research / Psychologist experience & creativity Annual Health Check module Medium Additional programmer, lots of Specialist Dr assistance, field testing")
102
Possible futures ProjectDifficultyResources required Additional Alternative & Augmentative Communication Supports Off and Online Medium Time, lot’s of help from a good speechie and graphic designer Edit my own I-CAN online, and set confidentiality restrictions (PHR) Medium-Hard Additional programmer, Full NMDS data recording and transmission Easy-Medium Additional programmer, few months
 Medium-Hard Additional programmer, Full NMDS data recording and transmission Easy-Medium Additional programmer, few months")
103
Possible futures ProjectDifficultyResources required Map ICD / ICF codes Medium Psychologist / Researcher time (a fair chunk of) Go in search of the ICF ‘core sets’ Medium-Hard Above project completed, more data Develop a Child & Youth Version Hard Additional Researchers, Programmers, field testing, ICF-CY Link with other databases (already some links with NMDS) Medium Which databases? Additional programmer Link with electronic prescribing systems / eMR systems Medium Programmer(s), assistance from USyd Health Informatics Unit
, assistance from USyd Health Informatics Unit.")
104
Possible futures ProjectDifficultyResources required Output Staffing Roster Estimate to Excel for costing Medium - Hard Done!! Costing estimation based on support need scores Medium Ideally access to government data on funding allocations (i.e. project in partnership with government) Active Support Style Outcomes and Goals Tracking Module Easy-Medium Additional programmer, creativity
 Active Support Style Outcomes and Goals Tracking Module Easy-Medium Additional programmer, creativity.")
105
Possible futures ProjectDifficultyResources required Multi-lingual versions Medium-Hard (not sure how some Asiatic languages would go) Skilled interpreter who can speak multiple languages, including PHP, field testing Develop brief I-CAN Hard Lots of time, more data, funding, creativity, additional programmer Develop super dooper I-CAN 5, with ‘drill down’ capabilities, voice controlled and bells and whistles Very Hard Team of programmers, Lots of help from Viv, Roger and some additional genius researchers Complete a PhD Very Very Hard Sam has multiple complex support needs
 Skilled interpreter who can speak multiple languages, including PHP, field testing Develop brief I-CAN Hard Lots of time, more data, funding, creativity, additional programmer Develop super dooper I-CAN 5, with ‘drill down’ capabilities, voice controlled and bells and whistles Very Hard Team of programmers, Lots of help from Viv, Roger and some additional genius researchers Complete a PhD Very Very Hard Sam has multiple complex support needs")
106
So many possible futures… Or should we just focus on the I-CAN assessment we have developed so far? No need to add more bells and whistles, focus on the core – a comprehensive assessment of support needs? You may say that I'm a dreamer But I'm not the only one I hope someday you'll join us….

107
Thank you!! It must be time for a drink! www.i-can.org.au

Similar presentations









































 2009 DEPARTMENT OF EDUCATION AND TRAINING.>")





