Download presentation
Presentation is loading. Please wait.

1
Inflammatory Disorders of Larynx
Dr. Vishal Sharma

2
Classification A. Acute infection B. Chronic infection
Acute simple laryngitis Chronic laryngitis Acute epiglottitis Tuberculosis Viral LTB Scleroma Bacterial LTB Candidiasis Spasmodic croup Sarcoidosis C. Laryngeal edema D. Laryngo-pharyngeal reflux disease (LPRD)
")
3
Causes for laryngeal edema
Laryngeal infections Retropharyngeal abscess / quinsy / Ludwig’s angina Angio-neurotic edema; Reinke’s edema Thermal / caustic burn Trauma: accidental / intubation / endoscopy Ca of larynx / pharynx; Post-irradiation Nephritis / heart failure / myxedema / anasarca

4
Acute (simple) Laryngitis
 Laryngitis")
5
Etiology Viral infection (common cold) Vocal abuse
Allergy / smoking / environmental pollution Gastro esophageal reflux disease Thermal / chemical burn due to inhalation Use of asthma inhalers Laryngeal trauma (endotracheal intubation) Undue physical or psychological stress
 Undue physical or psychological stress.")
6
Clinical Features History of upper respiratory tract infection
Hoarseness: high pitched husky voice Dry, paroxysmal cough, mainly at night Sore throat worsened by talking; fever, malaise Laryngoscopy: red, swollen supraglottic mucosa; mild erythema / swelling of true vocal cords; inspissated secretions b/w vocal cords

7
Flexible laryngoscopy

8
Treatment Prevention: avoidance of cold fluids, cold air, smoking, alcohol consumption Absolute voice rest Tincture Benzoin steam inhalation & mucolytics Anti-tussives: dextromethorphan, codeine Pantoprazole for GERD; analgesics for pain Antibiotics: for secondary bacterial infections Steroid: for laryngeal edema

9
Acute Epiglottitis

11
Synonym: Acute Supraglottitis Supraglottic laryngitis
Definition: Rapidly developing inflammation of epiglottis & adjacent tissues, due to bacterial infection, may cause life-threatening airway obstruction Causative agents: Haemophilus influenzae type b (Hib), Streptococcus pyogenes, Streptococcus pneumoniae, Staphylococcus aureus
, Streptococcus pyogenes, Streptococcus pneumoniae, Staphylococcus aureus.")
12
Symptoms Distress (respiratory) Dysphagia
Drooling (due to inability to swallow) Severe sore throat / odynophagia Muffled voice Sudden onset & rapid progression in children (in hours); Indolent course in adults (in days)
 Severe sore throat / odynophagia. Muffled voice. Sudden onset & rapid progression in children (in hours); Indolent course in adults (in days)")
13
Examination Simply depressing child's tongue with tongue depressor or indirect laryngoscopy may visualize enlarged, cherry red epiglottis in some situations These procedures may precipitate complete airway obstruction, hence avoided

14
Tripod sign Pt appears anxious
Leans forward with support of both forearms Extends neck in an attempt to maintain an open airway

15
Investigations 1. Flexible laryngoscopy: carried out only in ICU or OT with intubation / tracheostomy set ready 2. Post-intubation direct laryngoscopy 3. Plain x-ray soft tissue of neck lateral view 4. Culture from epiglottis during intubation: ve in 15% cases of H. influenzae 5. Blood culture: +ve in 15% cases of H. influenzae

16
Flexible laryngoscopy
Inflamed cherry-red epiglottis Thickened aryepiglottic folds Edematous arytenoid cartilages

17
Post-intubation direct laryngoscopy

18
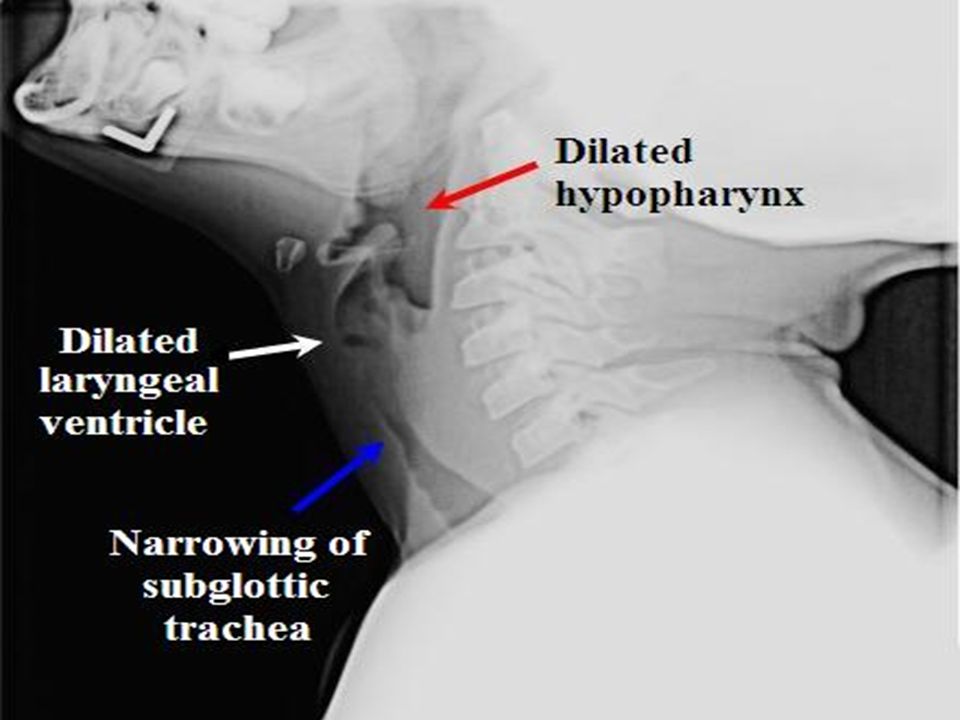
X-ray soft tissue neck Lateral view taken in erect position only
Enlargement of epiglottis (thumb sign) Absence of well defined vallecula (Vallecula sign) Thickening of aryepiglottic folds (cause for stridor) Circumferential narrowing of subglottic portion of trachea during inspiration (25% cases) Ballooning of hypopharynx
 Absence of well defined vallecula (Vallecula sign) Thickening of aryepiglottic folds (cause for stridor) Circumferential narrowing of subglottic portion of trachea during inspiration (25% cases) Ballooning of hypopharynx.")
19
X-ray soft tissue neck

20
X-ray soft tissue neck Red arrow = enlarged epiglottis
Yellow arrow = thickened ary-epiglottic folds

21
Ballooning of hypopharynx

23
Treatment Hospitalization, careful monitoring & isolation
Hydration + humidification + oxygen tent therapy Secure airway in acute stridor → Mechanical ventilation till swelling + inflammation subside IV Ceftriaxone: 100 mg/kg/d in 2 divided doses Hydrocortisone: 100 mg IV stat & 25 mg Q8H Rifampicin prophylaxis for household contacts

24
Methods of securing airway
Endotracheal intubation Trans-nasal: preferred Trans-oral Percutaneous trans-laryngeal ventilation by needle cricothyrotomy Tracheostomy: last resort for acute stridor

25
Prevention Hib vaccination for all children
Rifampicin prophylaxis (20 mg/kg /day; max. 600 mg) for 4 days should be given to all household contacts if: a. child in household < 4 years, not received appropriate doses of Hib vaccine b. immuno-compromised child, despite vaccination Children > 2 years with epiglottitis do not need vaccination as disease provides immune protection
 for 4 days should be given to all household contacts if: a. child in household < 4 years, not received appropriate doses of Hib vaccine. b. immuno-compromised child, despite vaccination. Children > 2 years with epiglottitis do not need vaccination as disease provides immune protection.")
26
Laryngo-Tracheo-Bronchitis (LTB)
")
27
Acute viral LTB (Croup)
Commonest infective cause of stridor in children Mean age for presentation = 18 months Causative agents: Parainfluenza virus type I, II, III Influenza virus Respiratory syncytial virus Rhinovirus Measles

28
Clinical Features Gradual onset preceeded by URTI of > 48 hrs
Hoarseness Biphasic stridor, mainly at night Dry cough (like barking of seal) Low grade fever (< 102 F) Child prefers to lie down, but is restless Dysphagia & drooling absent
 Low grade fever (< 102 F) Child prefers to lie down, but is restless. Dysphagia & drooling absent.")
29
Investigations Plain X-ray soft tissue neck, AP view
a. Church steeple or pencil-point sign: squared appearance of subglottic area replaced by cone shaped narrowing just below vocal cords b. Ballooning of hypopharynx Flexible laryngoscopy: narrowed subglottic area

30
Church Steeple sign

33
Treatment Hospitalization Humidification & mucolytic drugs
Hydration with IV fluid Hydrocortisone: 100 mg IV stat & 25 mg Q8H Oxygen tent: es bronchospasm & pulm. edema Antibiotic (IV Ceftriaxone): 100 mg/kg/day Racemic adrenaline (1:1000) nebulization Intubation / Tracheostomy for acute stridor
: 100 mg/kg/day. Racemic adrenaline (1:1000) nebulization. Intubation / Tracheostomy for acute stridor.")
36
Bacterial LTB Synonym: pseudo-membranous croup
More severe than viral LTB Causative agent: Staphylococcus aureus Pathology: sloughing of respiratory epithelium C/F: Hoarseness, biphasic stridor, dry cough, high grade fever (> 102F), child supine but restless X-ray neck, AP view: church steeple sign Rx: moist air + oxygen + antibiotics
, child supine but restless. X-ray neck, AP view: church steeple sign. Rx: moist air + oxygen + antibiotics.")
37
Subglottic laryngitis
Synonym: spasmodic croup Etiology: unknown (? Influenza virus infection) causing subglottic mucosal edema C/F: Child below 3 years with rapid onset of biphasic stridor + barking cough + low grade fever (< 102 F). Dysphagia & drooling are absent. X-ray neck, AP view: church steeple sign Rx: Moist air + oxygen + supportive treatment. Rarely endotracheal intubation. Avoid sedatives.
 causing subglottic mucosal edema. C/F: Child below 3 years with rapid onset of biphasic stridor + barking cough + low grade fever (< 102 F). Dysphagia & drooling are absent. X-ray neck, AP view: church steeple sign. Rx: Moist air + oxygen + supportive treatment. Rarely endotracheal intubation. Avoid sedatives.")
38
Acute epiglottitis Viral croup Bacterial croup Spasmodic croup R.P. abscess Age (yr) 3-7 1-3 1-8 Voice Normal or muffled Hoarse Cough Absent Barking seal-like Stridor Inspiratory Biphasic Dysphagia + drooling Severe Fever > 102 F < 102 F Posture Quiet, sitting Restless, supine Restless, sitting

39
Chronic Laryngitis

40
Definition: Chronic non-specific inflammation
causing irreversible changes of laryngeal mucosa Etiology of chronic laryngitis: Viral infection (common cold) Vocal abuse Allergy / smoking / environmental pollution Gastro esophageal reflux disease Thermal / chemical burn due to inhalation Laryngeal trauma (endotracheal intubation) Undue physical or psychological stress
 Vocal abuse. Allergy / smoking / environmental pollution. Gastro esophageal reflux disease. Thermal / chemical burn due to inhalation. Laryngeal trauma (endotracheal intubation) Undue physical or psychological stress.")
41
Chronic hyperemic laryngitis
Hoarseness (worse in morning) + dry cough for > 3 wk Persistent clearing of throat H/o previous URTI / GERD may be present Laryngoscopy: hyperemic laryngeal mucosa with sub-mucosal edema Treatment: Voice test + medicated steam inhalation + systemic antibiotic. Avoidance of alcohol & tobacco. Reversible within few weeks.
 + dry cough for > 3 wk. Persistent clearing of throat. H/o previous URTI / GERD may be present. Laryngoscopy: hyperemic laryngeal mucosa with sub-mucosal edema. Treatment: Voice test + medicated steam inhalation + systemic antibiotic. Avoidance of alcohol & tobacco. Reversible within few weeks.")
42
Chronic hyperemic laryngitis

43
Chronic hyperplastic laryngitis
Hoarseness (worse in morning) + dry cough for > 3 wk Persistent clearing of throat H/o previous URTI / GERD may be present Laryngoscopy: Mild congestion of laryngeal mucosa Patches of epithelial thickening Broad based polypoid lesions
 + dry cough for > 3 wk. Persistent clearing of throat. H/o previous URTI / GERD may be present. Laryngoscopy: Mild congestion of laryngeal mucosa. Patches of epithelial thickening. Broad based polypoid lesions.")
44
Chronic hyperplastic laryngitis

45
Chronic hyperplastic laryngitis

46
Chronic laryngitis histology
Kleinsasser’s classification: Grade I: simple squamous cell hyperplasia or keratosis Grade II: squamous cell hyperplasia + atypia (mild to moderate dysplasia) Grade III: carcinoma in situ with intact basal membrane
 Grade III: carcinoma in situ with intact basal membrane.")
47
Rx of hyperplastic laryngitis
Absolute voice rest for 48 hours Systemic antibiotic Tincture Benzoin steam inhalation Analgesics & anti histamine-decongestant Micro-laryngoscopic excision of lesion & HPE Grades I & II: no further treatment Grade III: total excision of lesion / radiotherapy

48
Prevention of recurrent attacks
Avoid breathing polluted air Avoid tobacco in any form (chewing, smoking) Avoid recreational drugs like marijuana Avoid alcohol consumption Avoid talking or shouting at noisy places Avoid continuous throat clearing Avoid whispering loudly
 Avoid recreational drugs like marijuana. Avoid alcohol consumption. Avoid talking or shouting at noisy places. Avoid continuous throat clearing. Avoid whispering loudly.")
49
Reinke’s edema

50
Introduction Accumulation of fluid in Reinke’s space
Synonyms: Bilateral diffuse polyposis, Smoker’s polyps, Polypoid corditis, Polypoid degeneration of vocal cords, Localized hypertrophic laryngitis 10% of benign laryngeal lesions

51
Reinke’s space

52
Etiology Irritants: tobacco smoke, dry air, dust, alcohol
Laryngeal allergy Infection: chronic sinusitis Idiopathic Edema limited to superior surface of vocal cord due to dense fibrous attachment to conus elasticus on under surface of vocal cord

53
Clinical Features Common in men b/w 30 – 60 years
Hoarseness: monotonous low-pitch voice Diplophonia: in asymmetric cord involvement Stridor: in B/L gross edema Early cases: ed convexity of medial cord margin Late cases: Pale, watery bags of fluid on superior surface of vocal cords, move to & fro on phonation

54
Reinke’s edema

55
Treatment Elimination of causative factors. Stop smoking.
Vocal cord stripping (decortication) under MLS: postero-anterior incision made on superior vocal cord surface → edematous fluid sucked out → edematous tissue removed with cup forceps Voice therapy: 1 wk before & 3 wks after surgery
 under MLS: postero-anterior incision made on superior vocal cord surface → edematous fluid sucked out → edematous tissue removed with cup forceps. Voice therapy: 1 wk before & 3 wks after surgery.")
56
Vocal cord stripping

57
Removal of edematous tissue

58
Trimming & re-draping

59
Pre-op vs. post-op

60
Angio-neurotic edema

61
Introduction Recurring attacks of swelling of face, larynx & extremities caused by edema due to vasodilatation & increased capillary permeability Types: Allergic: swelling with itching, laryngeal edema & bronchospasm Hereditary: Non-pruritic swelling + laryngeal edema + recurrent abdominal pain with vomiting & diarrhea

62
Etiology Atopy Food: nut, prawn, fish, egg, meat
Drug: penicillin, NSAIDs, ACE inhibitors, Sulpha drugs Insect bites: bee, wasp Physical stimulus: cold air, smoke, pollution C1 esterase inhibitor deficiency → complement pathway activation Trauma: accidental, surgical Emotional stress, anxiety

63
Treatment Allergic: antihistamines + corticosteroids
Hereditary: IV purified C1 esterase inhibitor 36,000 U for acute attacks & before surgery. Tranexemic acid (anti-fibrinolytic) & Methyl- testosterone → stimulate C1 esterase inhibitor Life-threatening stridor: subcutaneous adrenaline + aminophylline infusion + intubation / tracheostomy
 & Methyl- testosterone → stimulate C1 esterase inhibitor. Life-threatening stridor: subcutaneous adrenaline + aminophylline infusion + intubation / tracheostomy.")
64
Laryngeal Tuberculosis

65
Introduction Commonly associated with pulmonary TB
Posterior commissure arytenoids, vocal cords, ventricular bands & epiglottis mainly affected Method of spread: Bronchogenic: contact of larynx with sputum containing tubercular bacilli Hematogenous

66
Stages of laryngeal TB 1. Exudation + hyperemia in subepithelial layers 2. Mono-nuclear round cell infiltration of subepithelial layers causing pseudo-edema 3. Tubercle formation: granuloma with epithelioid cells + Langhans giant cells + caseation necrosis 4. Ulceration: shallow ulcers with undermined edges involving arytenoids & epiglottis (moth eaten or mouse nibbled appearance) 5. Cicatrization: ulcers heal by fibrosis
 5. Cicatrization: ulcers heal by fibrosis.")
67
Symptoms History of pulmonary TB
Weakness of voice followed by hoarseness Cough with hemoptysis Throat pain Referred earache Dysphagia & odynophagia due to perichondritis

68
Laryngoscopic examination
Impairment of vocal cord adduction (first sign) Areas affected commonly are inter-arytenoid area, posterior vocal cords + false cords + epiglottis Congestion of these areas with surrounding pallor Pseudo-edema mamillated appearance of interarytenoid area + turban-shaped epiglottis Shallow, undermined ulcers Vocal cord palsy + perichondritis
 Areas affected commonly are inter-arytenoid area, posterior vocal cords + false cords + epiglottis. Congestion of these areas with surrounding pallor. Pseudo-edema mamillated appearance of interarytenoid area + turban-shaped epiglottis. Shallow, undermined ulcers. Vocal cord palsy + perichondritis.")
69
Moth eaten ulcerations

70
Management Diagnosis Direct laryngoscopy & biopsy
Chest X-ray, P.A. view Sputum for A.F.B. Treatment Anti-tubercular medication for 9 months

71
Laryngo-pharyngeal reflux disease (LPRD)
")
72
GERD vs. LPRD

73
Symptoms of LPRD Hoarseness Persistent clearing of throat
Difficulty in swallowing food Breathing difficulties or choking episodes Annoying cough after eating Sticking sensation or lump in throat Heartburn & indigestion absent

74
Laryngoscopic findings
Erythema & swelling of inter-arytenoid area Erythema & swelling of arytenoids Posterior commissure mucosal hypertrophy Granulations / granuloma in posterior commissure Contact ulcer in posterior glottic commissure

75
Acid laryngitis

76
Diagnosis Ambulatory 24-hour double-probe (esophageal & pharyngeal) pH monitoring or pHmetry = gold standard for diagnosis of LPRD Distal probe = 5 cm above lower esophageal sphincter Proximal probe = 1 cm above upper esophageal sphincter, in hypopharynx behind laryngeal inlet LPRD = acidic pH in both probes GERD = acidic pH in distal probe only

77
24 hour ambulatory double-probe pH monitoing

79
pH metry

80
Hoarseness & dysphagia Nocturnal (supine) reflux -
GERD LPRD Heartburn ++++ + Hoarseness & dysphagia Nocturnal (supine) reflux - Daytime (upright) reflux ed lower esophageal pH ++ ed pharyngeal pH Pantoprazole treatment 40 mg OD X 6 wk 40 mg BD X 6 mth
 reflux. - Daytime (upright) reflux. ed lower esophageal pH. ++ ed pharyngeal pH. Pantoprazole treatment. 40 mg OD X 6 wk. 40 mg BD X 6 mth.")
81
Treatment Level I: Antireflux therapy (ART) A. Dietary modification
1. No eating or drinking within 3 hours of bedtime 2. Avoid overeating or reclining right after meals 3. No fried food; low-fat diet 4. Avoid coffee, tea, chocolate, mints, sodas 5. Avoid caffeine-containing foods & beverages 6. Avoid alcohol, especially in evening 7. Avoid other foods that cause reflux

82
B. Lifestyle modification
1. Elevate head-end of bed by 4 to 6 inches 2. Avoid wearing tight-fitting clothing or belts 3. If you use tobacco, quit! C. Liquid antacids: qid (1 tsf 1 hour after meal & at bedtime) Level II: Pantoprazole → 40 mg BD for 6 months Level III: Fundoplication surgery
 Level II: Pantoprazole → 40 mg BD for 6 months. Level III: Fundoplication surgery.")
83
Thank You

Similar presentations

















 Dr. ZAID AL-DAHWI Consultant ENT Head of ENT department KING SAUD MEDICAL CITY.>")






