Download presentation
Presentation is loading. Please wait.

1
The Ophthalmology of Childhood Vision Impairment Alistair Fielder City University, London This version probably has little stand-alone value but is meant as an accompaniement to the lecture

2
Topics Role of clinician Assessment of visual functions Causes and epidemiology of VI VI issues specific to children Patterns of presentation & development Impact of VI Clinical role

3
“Ophthalmologists tell me what I can see, but it has nothing to do with what I can do”

4
Role of Clinician in VI Orthopist, Optometrist & Ophthalmologist Diagnosis & quantification Treatment Involve & link other agencies Communication –Client & family, others Registration Monitor Research Maintain contact - be amenable Through the ages

5
What does he see? How do I measure? Approximation or precision? & when can I do this? How long for parents to wait?

8
Paediatric Ophthalmology Vision tests Visibility sweets, fixation patterns, Catford drum Resolution preferential looking, acuity card procedure, Cardiff cards Recognition Snellen, logMAR Sensitivity to detect vision impairment amblyopia

9
Vision Assessment - Infancy Birth –Fix & follow 6 weeks –Smile 4 months –Reach Anytime –Grating response –History

11
Babies have an innate preference to look at patterns, such as a face This is the basis of vision testing in infancy & why parents are such good historians

13
What Visual Functions? Their development Visual acuity Contrast sensitivity Colour Binocular vision Visual field Movement

21
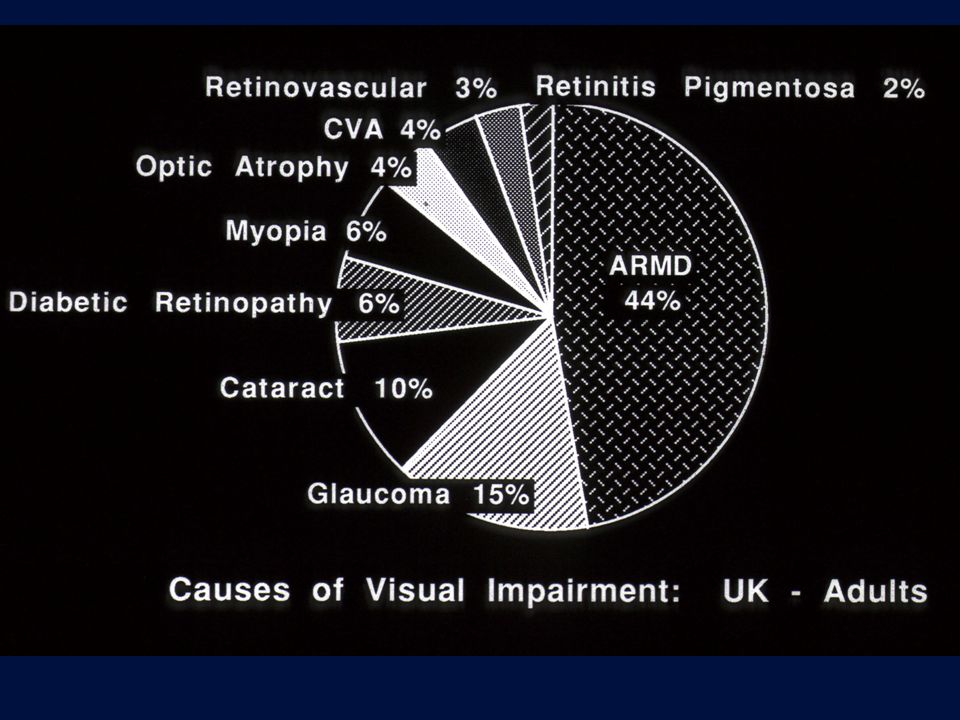
Causes of VI in Working Years Diabetes mellitus Retinitis pigmentosa Glaucoma Trauma Macular degeneration Survival

22
Childhood Visual Impairment Prenatal60% genetic50% intrauterine10% Perinatal23% ROP5-10% asphyxia13% Childhood13% male preponderance Prevalence developed countries0.3/1000 developing countries0.6 to 1.1/1000 Additional disability in 40-70% Preterm birth

23
Impact of Low Birth Weight on the Visual Pathway Severe visual impairment (VI) –all births - 1.25/1000 –<1500 g BW - 25.9/1000 births 1% of all live births, BUT 17.5% childhood VI X 26 for babies 2500-3499 g BW Associated impairments with VI –<1500 g BW 72% –>3500 g BW 44%
 –all births /1000 –<1500 g BW /1000 births 1% of all live births, BUT 17.5% childhood VI X 26 for babies g BW Associated impairments with VI –<1500 g BW 72% –>3500 g BW 44%")
24
Categories of VI Preventable infections - trauma - cataract - ROP anterior segment Partially preventable DR - glaucoma - ROP - ARMD - cataract anterior & posterior segment Non-preventable malformations - genetic - ROP - ARMD glaucoma - cataract anterior & posterior segment

25
Child Who Cannot See Classification Obvious ocular abnormality –Anterior & posterior segment Cataract Optic atrophy ROP + No obvious ocular abnormality –Mainly posterior segment or cerebral Optic nerve abnormalities –Atrophy - hypoplasia Delayed visual maturation Cortical vision impairment Retinal anomalies –Retinoschisis, achromatopsia –Lebers amaurosis –Albinism Nystagmus

35
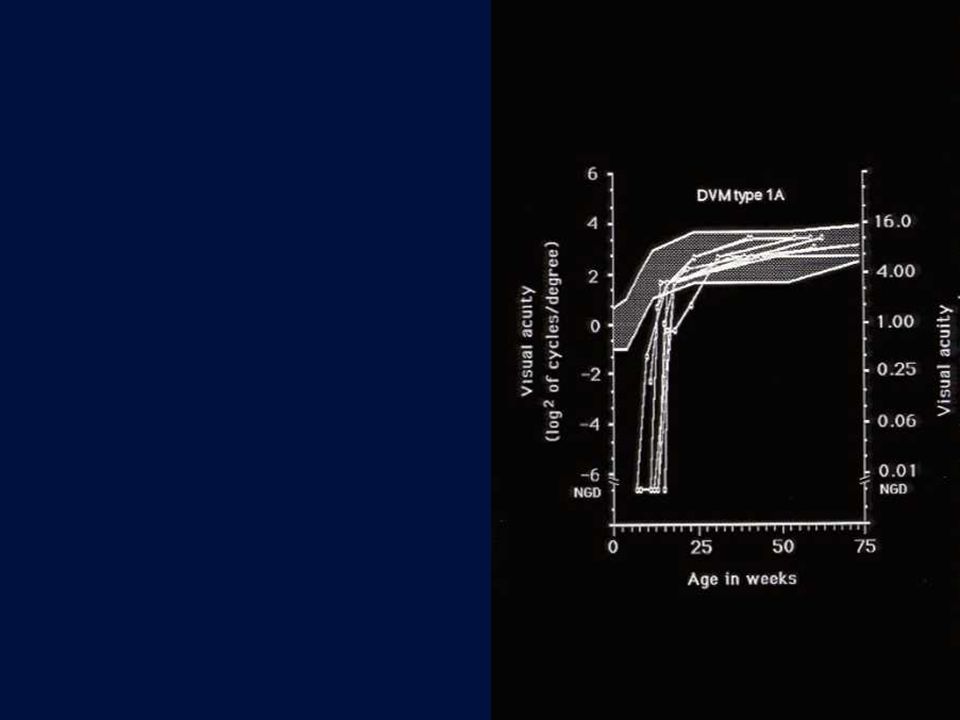
Delayed Visual Maturation Type 1 - isolated abnormality –ANormal perinatal period –BPerinatal problems Type 2 - obvious & permanant neurodevelopmental delay Type 3 - nystagmus (albinism) Type 4 - severe developmental, structural ocular abnormalities (not albinism)
 Type 4 - severe developmental, structural ocular abnormalities (not albinism)")
36
Cerebral Vision Impairment Reduced vision Normal eye examination & pupil responses Absence of nystagmus Natural history –<75% show some improvement –Early improvement more likely to be complete

37
CVI – Aetiology

38
Stage 3: Severe ROP

39
Problems with Screening & Treatment CRYO-ROP study: intervention @ “threshold” (5 continuous or 8 cumulative clock hours of stage 3+) 1988 Cryotherapy or laser Treatment “destroys evidence”
 1988 Cryotherapy or laser Treatment destroys evidence")
40
ROP- End Stage

41
Evaluation I History Overview assessment Full ophthalmic examination including –Vision assessment –Ophthalmic examination Paediatric assessment Investigations –Ophthalmic –Paediatric Children need referring

42
Evaluation II Ophthalmic tests –Electrophysiology VEP ERG EOG –Ultrasound –EUA Other tests - biochemical, etc Neuroimaging Referral(s)
")
43
Electrophysiological test & Neuroimaging

46
Nystagmus Is the pattern of nystagmus informative? Vision Localisation –Anterior –Posterior Aetiology –Ocular –Neurological

47
Patterns of Presentation Sudden & dramatic Insidious Masked effect of attending an ophthalmic unit

48
Predictive Value of Vision Tests

49
Patterns of visual development

50
Patterns of Visual Development

51
Vision deficit resulting from any obstacle to visual development Squint Blurred vision Refractive Opacity Especially of 1 eye

52
Impact of VI on the Child Visual functions Cognitive –Perception of objects in their totality & in environment –Spatial and intermodal interaction impaired Motor development - complex Language Social play, social interaction Poor self-concept & low self-esteem Other behaviours - eg sleep Education, leisure, social, health

53
Sleeping patterns of visually impaired

54
Impact of VI on the Family Diagnosis generated –Phases of grief, anger, loss & fear More care required for daily living tasks Lack of responsiveness by child –Loneliness, anxiety, depression in parents Behavioural problems in siblings Marital stress

55
“Ophthalmologists tell me what I can see, but it has nothing to do with what I can do”

56
VI - Impact on Child & Family The 5 senses interact & are interdependent, so VI has widespread & cumulative impact on development In most instances - VI is not stable during childhood, thus its impact on life’s activities varies

57
Impact of VI on the Child Visual functions Cognitive –Perception of objects in their totality & in environment –Spatial and intermodal interaction impaired Motor development - complex Language Social play, social interaction Poor self-concept & low self-esteem Other behaviours - eg sleep

58
Disability & Divergence from Full Function

59
Impact of VI on the Family Diagnosis generated –Phases of grief, anger, loss & fear More care required for daily living tasks Lack of responsiveness by child –Loneliness, anxiety, depression in parents Behavioural problems in siblings Marital stress

60
Functional Effects of VI VI severity –Total - severe - mild What do these categories mean for each activity of life? –Education, leisure, social, health

61
What is Functional Vision ? Acuity distance & near speed of reading & information processing Contrast Colour Field of vision Illumination Movement What do we measure?

62
Role of Clinician in VI Diagnosis & quantification Treatment? Involve & link other agencies Communication –Client & family, others Registration Monitor Research Maintain contact - be amenable Through the ages

63
VI Support Medical physician ophthalmic Optical spectacles LVAs Rehabilitation Social services Education Registration

64
Disability Through the Ages Diagnosis Infancy Preschool School age After school Adult life Much VI is not stable Info forgotten, misheard, wrong, updatable

65
Communication Between & within –Services - statutory and voluntary –Locations - community & hospital, etc –Professions When? –Depends on individual’s & family requirements Education, occupation, social, leisure, health, etc For whom? –Client & professional

66
Treatment the eye Treatment the child & family

67
Components of Disability Care Specialist expertise Always available & amenable Affordable Communication Link - education, health, social services Involve the client - parents Key worker

Similar presentations





























 ABSTRACT Aims:>")








