Download presentation
Presentation is loading. Please wait.

1
Vitamin D Adipocytokines ….and GDM pregnancies

2
Objectives: To review the role for Vit D as an insulin-sensitizing hormone, with particular reference to GDM pregnancy To review some of the roles for adipocytokines in insulin resistance and GDM pregnancy To review our local experience with Vit D/adipocytokines in GDM women and their neonates

3
But first….back to med school for a moment

4
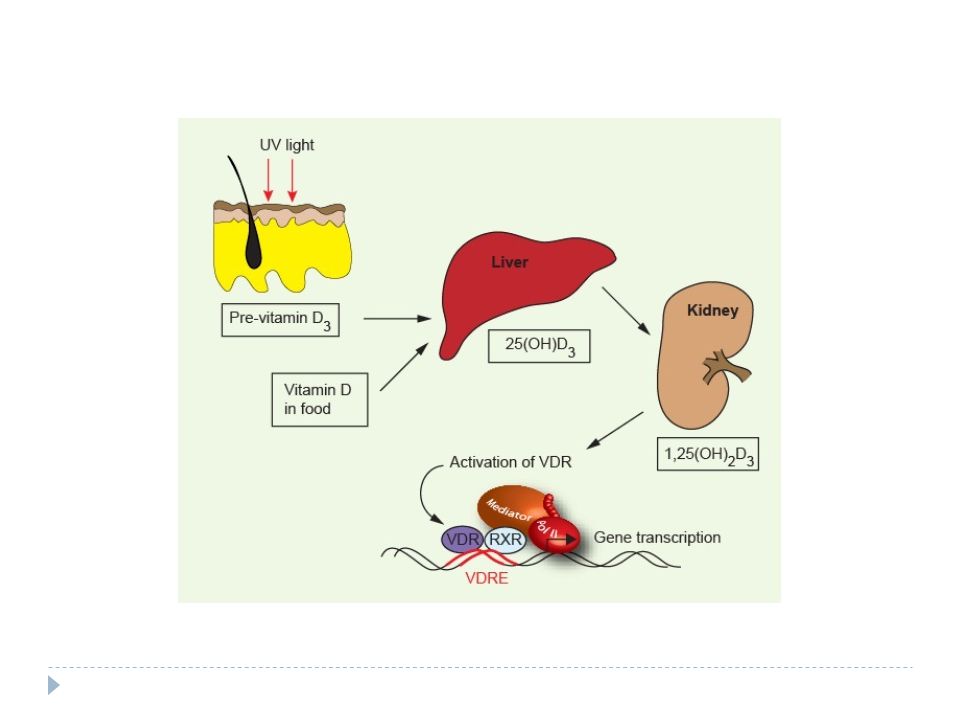
Vitamin D: a few reminders Ergocalciferol (D2): provitamin form Cholecalciferol (D3): inactivated, unhydroxylated form 25(OH) Vit D3: this from is the least variable, and considered best measure of sufficiency. Therefore, most common form measured. 1, 25(OH) Vit D3: this form is variable. Measured in odd rare conditions such as Vit D resistant rickets
 Vit D3: this form is variable. Measured in odd rare conditions such as Vit D resistant rickets.")
5
Vitamin D: a few reminders Ergocalciferol (D2): provitamin form Cholecalciferol (D3): inactivated, unhydroxylated form 25(OH) Vit D3: this form is the least variable, and considered best measure of sufficiency. Therefore, most common form measured. This is the form that will appear in this talk as VitD 1, 25(OH) Vit D3: this form is variable. Measured in odd rare conditions such as Vit D resistant rickets
 Vit D3: this form is variable. Measured in odd rare conditions such as Vit D resistant rickets.")
7
Vitamin D: recent oddities We usually think of Vit D as promoting bone health The last few decades have illustrated that Vit D has hormone properties structural similarities with testosterone, steroids, cholesterol

8
….cholecalciferol

9
…….cholesterol

10
Vit D and GDM: what do we know? Vit D deficiency suspected to be a risk factor for glucose intolerance For instance: 54 GDM, 39 IGT; 11 controls, matched for age, BMI, pregnancy week 24-28 [NB: Iranian study] Soheilykhah Nutr Clin Pract 2012. 25. 524

11
CONCLUSIONS: 83% GDM and IGT women had VitD <20ng/ml vs 71.2% Controls (p=0.03) Lowest VitD levels were in GDM women compared to Controls
 Lowest VitD levels were in GDM women compared to Controls ")
12
Does Vit D status predict GDM risk? 953 pregnant women in USA Nested case/control study VitD level taken at 16 weeks gestation 57 women developed GDM Zhang Plos One 2008.3.e3753

13
CONCLUSIONS VitD at 16 wks in women developing GDM: 24.2 ng/ml vs Controls: 30.1 ng/ml (p<0.001) [Difference remained significant after adjusting for weight, age, race, family history of DM, prepreg BMI]
![CONCLUSIONS VitD at 16 wks in women developing GDM: 24.2 ng/ml vs Controls: 30.1 ng/ml (p<0.001) [Difference remained significant after adjusting for weight, age, race, family history of DM, prepreg BMI]](http://images.slideplayer.com/8/2408620/slides/slide_13.jpg "CONCLUSIONS VitD at 16 wks in women developing GDM: 24.2 ng/ml vs Controls: 30.1 ng/ml (p<0.001) [Difference remained significant after adjusting for weight, age, race, family history of DM, prepreg BMI]")
14
Does VitD predict adverse preg outcomes? Meta-analysis up to Oct 2012 24 studies fit criteria (Vitamin D/status/deficiency/insufficiency/pregnancy) Outcome: women with VitD <50 nm/l: OR 2.09 risk pre-eclampsia (CI: 1.5-2.9) OR 1.38 risk GDM (1.12-1.7) OR 1.57 risk preterm birth (1.08-2.31) OR 1.52 risk SGA (1.08-2.15) Wei.Mat-Fetal Medicine 2013.26.889
 Outcome: women with VitD <50 nm/l: OR 2.09 risk pre-eclampsia (CI: ) OR 1.38 risk GDM ( ) OR 1.57 risk preterm birth ( ) OR 1.52 risk SGA ( ) Wei.Mat-Fetal Medicine")
15
What about interventional studies? ………..wait……………………

16
What links VitD and insulin resistance? 1. No one really knows BUT 2. Perhaps: through inflammation: VitD can be shown to be associated with anti-inflammatory properties; and insulin resistant states are also pro-inflammatory states inflammation endothelial dysfunction pre-eclampsia inflammation immune modulation (IL-1 and IL-6 in particular)
.")
17
Links between VitD and insulin resistance 3. Perhaps: VitD receptors are present in the placenta and fetal tissues VitD regulates genes involved in trophoblast invasion/angiogenesis

18
Links between VitD and insulin resistance 4. Perhaps: pancreatic beta cells have VitD receptors may regulate insulin secretion Vit D stimulates insulin receptor expression promotes insulin sensitivity

19
VitD and inflammatory markers So: holding onto VitD considerations but switching over to thinking about adipocytokines

20
What are Adipocytokines Proteins produced by adipose cells [note: adipose is not just unwanted insulation, but rather a large endocrine organ] Many, many, many known and still unknown associations and effects
![What are Adipocytokines Proteins produced by adipose cells [note: adipose is not just unwanted insulation, but rather a large endocrine organ] Many, many, many known and still unknown associations and effects](http://images.slideplayer.com/8/2408620/slides/slide_20.jpg "What are Adipocytokines Proteins produced by adipose cells [note: adipose is not just unwanted insulation, but rather a large endocrine organ] Many, many, many known and still unknown associations and effects")
21
Adipocytokines You know some of these already: leptin adiponectin TNF- α interleukins resistin …etc….

22
Just a few metabolic associations of adipokines Low adiponectin levels have been associated with an increased incidence of Type 2 DM Adiponectin increased insulin sensitivity, fatty acid oxidation and reduces liver glucose production Leptin reflects total body adipose mass Resistin levels increase with fat mass and correlate with insulin resistance TNF α and IL-6 increased in obesity and are linked to insulin resistance and type 2 DM

23
Functions of Adipokines? Endocrine; paracrine; autocrine roles in: hemostasis lipids metabolism atherosclerosis BP regulation insulin sensitivity angiogenesis immunity inflammation Miehle. Clin Endocrinology 2012.76.2

25
Adipocytokines and GDM TNF- α correlates with insulin resistance in pregnancy TNF- α is released from maternal side of placenta Leptin rises during pregnancy and falls after delivery Leptin correlates with insulin resistance in pregnancy Adiponectin levels are lower in GDM than control preg women Lacroix. Curr Diab Rep 2013. 13. 238

26
For instance: Normal PregGDMPre-eclampsia LEPTIN Rises, peak at 28 wksIncreased ADIPONECTIN Declines thru out pregnancy DecreasedIncreased RESISTIN Higher than nonprgtIncreased VISFATIN Peaks 19-26 weeks then drops Increased

28
..So, cooking up a study in London ON INTERESTING UNKNOWNS: What are VitD levels in offspring of GDM pregnancies? What are the profiles of adipocytokines in GDM women AND their offspring? Are maternal and neonatal VitD levels correlated? Are maternal and neonatal adipokine levels correlated? Do corralations exist between VitD and inflammatory adiokines (maternal and neonatal)?
 .")
29
…..we had the following building blocks… LUCK Kelly Summers’ adipokine assay GDM women

31
PSI grant Maternal, umbilical arterial and umbilical venous 25 hydroxyvitamin D and adipocytokine concentrations in pregnancies with and without gestational diabetes R McManus, K Summers, B DeVrijer, N Cohen, A Thompson, I Giroux Clinical Endocrinology 2014; 80:635-641.

32
Methods Case control GDM diagnosed before clinic referral no recruitment during Nov-Mar months GDM and Controls recruited at 31 weeks Did 48 hour dietary and supplement recall [before GDM saw RD]
![Methods Case control GDM diagnosed before clinic referral no recruitment during Nov-Mar months GDM and Controls recruited at 31 weeks Did 48 hour dietary and supplement recall [before GDM saw RD]](http://images.slideplayer.com/8/2408620/slides/slide_32.jpg "Methods Case control GDM diagnosed before clinic referral no recruitment during Nov-Mar months GDM and Controls recruited at 31 weeks Did 48 hour dietary and supplement recall [before GDM saw RD]")
33
Methods Maternal blood taken/spun/frozen at 31 weeks for Ca Phosphate BG CRP PTH Adipocytokines (adiponectin, resistin, PAI-1, IL-6; Il-8, leptin, TNF α, MCP-1)
")
34
Methods On day of delivery: Neonatal umbilical artery and umbilical vein bloods were taken for DR staff for: Ca Phosphate BG CRP PTH Adipocytokines (adiponectin, resistin, PAI-1, IL-6; Il-8, leptin, TNF α, MCP-1)
")
35
….do you want to guess? Umbilical artery flows: Umbilical vein flows:

36
So umbilical arterial blood would reflect fetal chemistry umbilical vein blood would reflect maternal AND placental chemistry

38
Demographics Maternal age pre-pregnancy weight maternal weight at time of blood taking Infant birth weight infant gestational age apgar scores duration of hospital stay/complications

39
A few stats Sample size of 24 X2=48 would allow for detecting a 30 nm/l difference between [VitD] in GDM women vs C
![A few stats Sample size of 24 X2=48 would allow for detecting a 30 nm/l difference between [VitD] in GDM women vs C](http://images.slideplayer.com/8/2408620/slides/slide_39.jpg "A few stats Sample size of 24 X2=48 would allow for detecting a 30 nm/l difference between [VitD] in GDM women vs C")
40
Results 73 women 36 GDM; 37 C Matched for week of gestation; present weight; pre-preg weight; maternal VitD intake

41
MATERNAL CHARACTERISTICS AND BIOCHEMISTRY CONTROLGDMp N3736 Age (yrs)30.2±4.131.6±5.00.19 Weeks Gestation31.4±3.631.6±2.90.84 Current Weight (kg)85.8±21.389.1±16.00.47 Pre-pregnancy Weight (kg) 74.4±18.977.7±17.40.44 Pre-pregnancy BMI (kg/m 2 ) 27.2±7.228.7±5.50.34 Maternal Vitamin D Intake (ug/day) 14.4±6.415.8±2.90.44 ‡
30.2± ± Weeks Gestation31.4± ± Current Weight (kg)85.8± ± Pre-pregnancy Weight (kg) 74.4± ± Pre-pregnancy BMI (kg/m 2 ) 27.2± ± Maternal Vitamin D Intake (ug/day) 14.4± ± ‡")
42
MATERNAL CHARACTERIST ICS AND BIOCHEMISTRY CONTROLGDMp 25(OH)D (nm/L) [range]93.2±19.2 [55-135]77.3±24.3 [33-128]0.009 PTH (pm/L)4.33±16.571.78±1.100.732 † Calcium (mm/L)2.20±0.132.20±0.090.898 Phosphate (mm/L)1.06±0.181.04±0.170.519 GLUCOSE (MM/L)4.68±0.895.46±1.290.008 Alkaline Phosphatase (u/L)82.2±27.189.5±18.80.234 CRP (mg/L)6.03±4.996.00±5.360.983 ADIPONECTIN ( Μ G/ML) 34.1±20.317.5±11.8<0.001 † RESISTIN (NG/ML)31.9±12.125.4±9.10.045 PAI-1 (NG/ML)21.0±12.613.9±10.00.038 IL-6 (pg/ml)1.93±1.321.76±1.000.627 IL-8 (pg/ml)2.39±0.982.25±1.920.185 † Leptin (ng/ml)41.2±33.740.1±26.40.899 TNF- α (pg/ml) 4.99±2.085.83±2.460.196 MCP-1 (pg/ml)115.6±52.8115.9±81.10.688 †
![MATERNAL CHARACTERIST ICS AND BIOCHEMISTRY CONTROLGDMp 25(OH)D (nm/L) [range]93.2±19.2 [55-135]77.3±24.3 [33-128]0.009 PTH (pm/L)4.33± ± † Calcium (mm/L)2.20± ± Phosphate (mm/L)1.06± ± GLUCOSE (MM/L)4.68± ± Alkaline Phosphatase (u/L)82.2± ± CRP (mg/L)6.03± ± ADIPONECTIN ( Μ G/ML) 34.1± ±11.8<0.001 † RESISTIN (NG/ML)31.9± ± PAI-1 (NG/ML)21.0± ± IL-6 (pg/ml)1.93± ± IL-8 (pg/ml)2.39± ± † Leptin (ng/ml)41.2± ± TNF- α (pg/ml) 4.99± ± MCP-1 (pg/ml)115.6± ± †](http://images.slideplayer.com/8/2408620/slides/slide_42.jpg "MATERNAL CHARACTERIST ICS AND BIOCHEMISTRY CONTROLGDMp 25(OH)D (nm/L) [range]93.2±19.2 [55-135]77.3±24.3 [33-128]0.009 PTH (pm/L)4.33± ± † Calcium (mm/L)2.20± ± Phosphate (mm/L)1.06± ± GLUCOSE (MM/L)4.68± ± Alkaline Phosphatase (u/L)82.2± ± CRP (mg/L)6.03± ± ADIPONECTIN ( Μ G/ML) 34.1± ±11.8<0.001 † RESISTIN (NG/ML)31.9± ± PAI-1 (NG/ML)21.0± ± IL-6 (pg/ml)1.93± ± IL-8 (pg/ml)2.39± ± † Leptin (ng/ml)41.2± ± TNF- α (pg/ml) 4.99± ± MCP-1 (pg/ml)115.6± ± †")
43
DELIVERY OUTCOMES CONTROLGDMp Infant Weight (g) GESTATIONAL AGE (weeks) 3457.8 ± 455.2 39.5±0.9 3384.6 ± 504.2 38.2±1.2 0.547 <0.001 Apgar 18.2 ± 1.78.0 ± 2.10.749 Apgar 28.8 ± 0.58.9 ± 0.60.689 Labour Duration (hours) 8.1 ± 5.87.6 ± 4.00.891 † Placental Weight (g)677.2 ± 169.7746.0 ± 197.60.159 Post partum Stay (hours) 46.8 ± 15.545.5 ± 25.40.353 ‡ Sex – Male (%)19 (59)19 (61)0.877 Induced Labour (%)17 (53)20 (64)0.359 Caesarian Section (%)8 (22)6 (16)0.51
 GESTATIONAL AGE (weeks) ± ± ± ± <0.001 Apgar 18.2 ± ± Apgar 28.8 ± ± Labour Duration (hours) 8.1 ± ± † Placental Weight (g)677.2 ± ± Post partum Stay (hours) 46.8 ± ± ‡ Sex – Male (%)19 (59)19 (61)0.877 Induced Labour (%)17 (53)20 (64)0.359 Caesarian Section (%)8 (22)6 (16)0.51")
44
INFANT ARTERIAL UMBILICAL CHEMISTRY CONTROLGDMp 25(OH)D (nm/L)65.6±17.658.0±20.80.195 Calcium (mm/L)2.54±0.212.46±0.350.420 Glucose (mm/L)3.67±0.813.44±1.500.227 ‡ ADIPONECTIN (ΜG/ML) 100.0±52.257.0±31.70.006 RESISTIN (NG/ML)222.4±456.557.1±34.50.030 ‡ PAI-1 (NG/ML)21.5±22.711.2±6.60.049 † IL-6 (pg/ml)37.8±105.716.9±22.30.779 † IL-8 (pg/ml)20.7±23.011.8±5.80.784 ‡ Leptin (ng/ml)44.7±46.446.1±37.90.910 TNF-α (pg/ml)10.7±2.111.7±3.00.209 MCP-1 (pg/ml)690.6±552.6574.8±275.40.608 †
D (nm/L)65.6± ± Calcium (mm/L)2.54± ± Glucose (mm/L)3.67± ± ‡ ADIPONECTIN (ΜG/ML) 100.0± ± RESISTIN (NG/ML)222.4± ± ‡ PAI-1 (NG/ML)21.5± ± † IL-6 (pg/ml)37.8± ± † IL-8 (pg/ml)20.7± ± ‡ Leptin (ng/ml)44.7± ± TNF-α (pg/ml)10.7± ± MCP-1 (pg/ml)690.6± ± †")
45
INFANT VENOUS UMBILICAL CHEMISTRY CONTROLGDMp 25(OH)D (nm/L)64.8±11.566.3±19.50.952 ‡ Calcium (mm/L)2.62±0.252.50±0.180.086 Glucose (mm/L)3.70±1.243.96±0.840.422 ADIPONECTIN ( Μ G /ML) 109.9±49.564.0±33.70.004 RESISTIN (NG/ML)237.4±529.247.5±17.9<0.001 ‡ PAI-1 (NG/ML)15.5±13.98.4±8.20.009 † IL-6 (pg/ml)38.4±109.411.2±12.40.871 † IL-8 (pg/ml)15.7±18.68.7±5.00.464 ‡ Leptin (ng/ml)49.9±40.155.4±48.60.675 TNF- α (pg/ml) 10.9±2.511.8±2.80.253 MCP-1 (pg/ml)457.4±289.7425.0±247.90.690
D (nm/L)64.8± ± ‡ Calcium (mm/L)2.62± ± Glucose (mm/L)3.70± ± ADIPONECTIN ( Μ G /ML) 109.9± ± RESISTIN (NG/ML)237.4± ±17.9<0.001 ‡ PAI-1 (NG/ML)15.5± ± † IL-6 (pg/ml)38.4± ± † IL-8 (pg/ml)15.7± ± ‡ Leptin (ng/ml)49.9± ± TNF- α (pg/ml) 10.9± ± MCP-1 (pg/ml)457.4± ±")
46
Searching for correlations [we limited correlations to r>0.4 or r<-0.4; p<0.05] Maternal Control VitD levels: + correlated with resistin only Maternal GDM VitD: + correlated with PAI-1; IL-8; TNF- α
![Searching for correlations [we limited correlations to r>0.4 or r<-0.4; p<0.05] Maternal Control VitD levels: + correlated with resistin only Maternal GDM VitD: + correlated with PAI-1; IL-8; TNF- α](http://images.slideplayer.com/8/2408620/slides/slide_46.jpg "Searching for correlations [we limited correlations to r>0.4 or r<-0.4; p<0.05] Maternal Control VitD levels: + correlated with resistin only Maternal GDM VitD: + correlated with PAI-1; IL-8; TNF- α")
47
Searching for Correlations..cont Neonatal VitD levels were not correlated with any of: infant weight placental weight Apgar scores labour duration/hospital stay adipocytokines

49
Admitting our limitations Big picture: no one knows what level of VitD is “ideal” for the non-osteomalacial actions of VitD Our women were not as VitD deficient as in some studies so differing conclusions might occur if there was a wider range of serum levels Our GDM women were generally only mildly hyperglycemic (ie) no one was on insulin when maternal bloods were taken: again a wider range of insulin impairement may have uncovered differing results
 no one was on insulin when maternal bloods were taken: again a wider range of insulin impairement may have uncovered differing results")
51
So…what…? #1: As expected: GDM women had lower adiponectin than Controls however, this finding was present despite being matched for weight and pregnancy week lower adiponectin levels would be consistent with increased GDM maternal inflammation…but….

52
So what #2 GDM had lower resistin and PAI-1 levels [argues against inflammatory biochemical profile] GDM leptin was not different from C GDM CRP, ILs, TNF α, MCP-1 not different as well overall, no conclusive evidence for inflammatory chemistry in GDM women
![So what #2 GDM had lower resistin and PAI-1 levels [argues against inflammatory biochemical profile] GDM leptin was not different from C GDM CRP, ILs, TNF α, MCP-1 not different as well overall, no conclusive evidence for inflammatory chemistry in GDM women](http://images.slideplayer.com/8/2408620/slides/slide_52.jpg "So what #2 GDM had lower resistin and PAI-1 levels [argues against inflammatory biochemical profile] GDM leptin was not different from C GDM CRP, ILs, TNF α, MCP-1 not different as well overall, no conclusive evidence for inflammatory chemistry in GDM women")
53
So what #3: GDM maternal VitD lower than Controls But: Umbilical arterial and venous VitD showed no difference between GDM and C offspring

54
So what #4 Maternal GDM VitD levels were positively (not negatively as expected) correlated with some adipokines thought to be associated with inflammation (PAI-1; IL-8, TNF α) Neonatal VitD levels did not correlate with inflammatory markers
 correlated with some adipokines thought to be associated with inflammation (PAI-1; IL-8, TNF α) Neonatal VitD levels did not correlate with inflammatory markers")
55
So what #5 Neonates born to mothers with GDM also manifested lower adiponectin and resistin levels even in umbilical arterial bloods suggesting that there are adverse adipokine profiles present at birth

57
So what #6 We learned a very important life lesson: Never ever again do a study where blood samples from babies have to be centrifuged and frozen at any time of day, night, holidays……

59
Just an aside Enthusiasm for VitD as THE miracle metabolic hormone has waned Much of what our study was built upon (remember, grant applied for <2008) tantalizing hints and correlations around VitD effects However, interventional studies have suggested perhaps some effect attributable to VitD, although final word not yet in…..
 tantalizing hints and correlations around VitD effects However, interventional studies have suggested perhaps some effect attributable to VitD, although final word not yet in…..")
60
For instance 54 women with GDM (Iran) randomized to placebo or cholecalciferol 50,000 u at study entry and day 21 fasting samples for BG and insulin taken at study onset as well as after 6 weeks
 randomized to placebo or cholecalciferol 50,000 u at study entry and day 21 fasting samples for BG and insulin taken at study onset as well as after 6 weeks")
61
Results: VitD supplementation: was correlated with lower FG (-17.1±14.8 mg/dl vs -0.9±16.6 mg/dl, p<0.001) was correlated with lower serum insulin was correlated with improved QUICKI index Asemi. Am J Clin Nutr 2013.98.1425

62
one more… 120 Iranian women <12 weeks of pregnancy randomized to: 200 u VitD OD; 50,000 u VitD monthly 50,000 u Vit D Q2 weeks until delivery

63
measured: FBG, insulin, Ca, VitD before and after intervention

64
Results Group C receiving 50,000 u every 2 weeks had biggest rise in VitD level FBG dropped 2.02 mg/dl in Group C (NS) Insulin level in group C went up less than Group A (NS) comparing all 3 groups: insulin and HOMA IR were improved with higher doses of VitD supplementation Soheilyhkhah Gynec Endocrinol 2013. 29. 396

65
..one last London connection DALI study Vitamin D and lifestyle intervention for gestational diabetes mellitus (GDM) prevention: an European multicentre, randomized trial-study protocol 9 countries <20 weeks gestation 8 intervention arms (placebo, healthy diet, healthy activity, Vit D combos)
 prevention: an European multicentre, randomized trial-study protocol 9 countries <20 weeks gestation 8 intervention arms (placebo, healthy diet, healthy activity, Vit D combos)")
66
DALI Vit D dose is 1600 u OD until delivery primary outcome: gestational weight gain, fasting glucose and insulin sensitivity, OB outcomes [biorepository blood is being stored at Lawson/David Hill] Jelsma BMC Pregnancy Childbirth 2013. 13.124
![DALI Vit D dose is 1600 u OD until delivery primary outcome: gestational weight gain, fasting glucose and insulin sensitivity, OB outcomes [biorepository blood is being stored at Lawson/David Hill] Jelsma BMC Pregnancy Childbirth 2013.](http://images.slideplayer.com/8/2408620/slides/slide_66.jpg)
67
that’s all ….

Similar presentations























![Ca ++ and P i Homeostasis. Ca ++ in the plasma [Ca ++ ] in plasma: 2.5 mM, of which about ½ is bound and thus physiologically inactive. Ratio of free/bound.](/12/3581741/big_thumb.jpg "Ca ++ and P i Homeostasis. Ca ++ in the plasma [Ca ++ ] in plasma: 2.5 mM, of which about ½ is bound and thus physiologically inactive. Ratio of free/bound.>")


, a common medical complication of pregnancy, is defined as “any degree of glucose intolerance with onset or first.>")