Download presentation
Presentation is loading. Please wait.

1
Donald M. Arnold, MDCM MSc Program Director, Transfusion Medicine McMaster University Canadian Blood Services

2
Speaker’s Topic: “Viruses and Vampires: The History of Transfusion Medicine in Canada” (D. Arnold) Financial Conflicts of Interest: Research funding from CBS Non-Financial Conflicts of Interest: Associate Medical Director CBS Unlabelled/ unapproved Use Disclosure: N/A Disclosures
 Financial Conflicts of Interest: Research funding from CBS Non-Financial Conflicts of Interest: Associate Medical Director CBS Unlabelled/ unapproved Use Disclosure: N/A Disclosures.")
3
The Past:“Tainted blood scandal” The Present:What we learned The Future:Where is TM headed

4
Blood is a life-saving commodity Transfusion Medicine crosses all disciplines There will always be new threats to the blood supply People will continue to be harmed by blood Highly emotional, political business

7
Justice Horace Krever, 1997 “The most influential report on public health in Canadian history” -K. Wilson CMAJ 2007

8
1,000 infected with HIV 30,000 infected with hepatitis C After being transfused blood between late 1970s and 1980s “Arguably the largest public heath catastrophe in the country’s history” -Picard, A. The Gift of Death 1995

9
“Would it not be possible, in time of peace and quiet, to form relief societies for the purpose of having care given to the wounded in wartime by zealous, devoted, and thoroughly qualified volunteers?” Henry Dunant, founder of the Red Cross in 1863

10
1981: First published report of homosexual men in the US infected with PCP pneumonia 1982: First reported case of PCP in patients with hemophilia 1983: 593 people diagnosed with AIDS in the US 1983: US blood bankers defer high risk donors May 1984: HIV virus isolated (Robert Gallo) Mar 1985:HIV test implemented in US Nov 1985: HIV test implemented in Canada
 Mar 1985:HIV test implemented in US Nov 1985: HIV test implemented in Canada")
11
1986: US implements ALT surrogate testing for NANB hepatitis 1990: Test for hepatitis C implemented 1993: Results of the Blajchman-Feinman study presented 1995: Study results published (Lancet) 1997: The Commission of Inquiry on the Blood System in Canada (“Krever Commission”) released 1998: Birth of CBS and Hema-Quebec
 1997: The Commission of Inquiry on the Blood System in Canada ( Krever Commission ) released 1998: Birth of CBS and Hema-Quebec")
12
Copyright ©2006 American Society of Hematology. Copyright restrictions may apply. Arnold, D. M. et al. Blood 2006;108:460-464 Figure 1. Kaplan-Meier survival curves of HIV-positive (n = 660) and HIV-negative (n = 1767) individuals with hemophilia in Canada (1982-2003)
 and HIV-negative (n = 1767) individuals with hemophilia in Canada ( ).")
13
1988 – 1992 (N= 4,588) Recipients randomized to: Surrogate testing NEG (‘withhold’ group) Routine screening (‘no withhold’ group) Outcome: post-transfusion hepatitis: ALT increased to at least 2.5 times ULN Other causes of abnormal liver function excluded HBV DNA HCV ELISA, PCR
 Recipients randomized to: Surrogate testing NEG (‘withhold’ group) Routine screening (‘no withhold’ group) Outcome: post-transfusion hepatitis: ALT increased to at least 2.5 times ULN Other causes of abnormal liver function excluded HBV DNA HCV ELISA, PCR")
15
Transfusion Transmitted HIV and hepatitis was a disaster that affected every country worldwide 8 month lag between implementation of HIV screening In US and in Canada Lack of implementation of surrogate testing for NANB hepatitis

16
1. Compensate the victims 2. Safe, Free, Sufficient, Accessible System 3. Single, public, open, independent operator 4. Promote appropriate use of blood products 5. Funded by hospitals 6. Creation of a national database 7. 10% for Rx&D 8. Mandatory reporting of adverse events

17
1. Precautionary Measures 2. Governance

18
“…action to reduce risk should not await scientific certainty. When there was reasonable evidence that serious infectious diseases could be transmitted by blood, the principal actors in the blood supply system in Canada refrained from taking essential preventive measures until causation had been proved with scientific certainty. The result was a national public health disaster.” Krever H. Government of Canada 1997

19
To ensure public safety, precautionary measures should be adopted despite incomplete scientific information.

20
Wilson K, CMAJ 2007

21
“Responsibility for the blood system is fragmented… the various functions integral to the supply of blood, such as regulation, funding and planning, are undertaken by different stakeholders… This lack of definition may affect accountability within the system, and ultimately its safety.” Krever H. Government of Canada 1997

22
Canadian Blood Services and Hema-Quebec CBS is insulated (arms-length, not-for-profit) from provincial funders Highly structured, organized company
 from provincial funders Highly structured, organized company")
23
Transfusion Medicine Residency Training Program Funding for TM research Health Advocacy

24
Unique approach to cost-effectiveness in Transfusion Medicine Custer TMR 2009 Less attention paid to higher risks (e.g. non- infectious transfusion reactions) Address shaken public confidence
 Address shaken public confidence.")
26
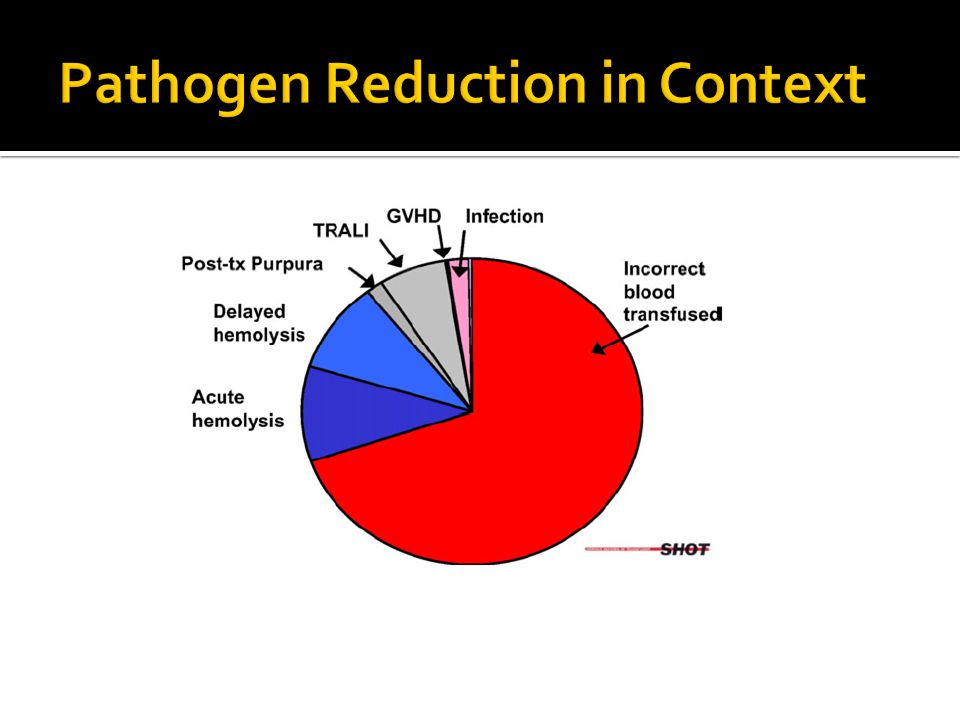
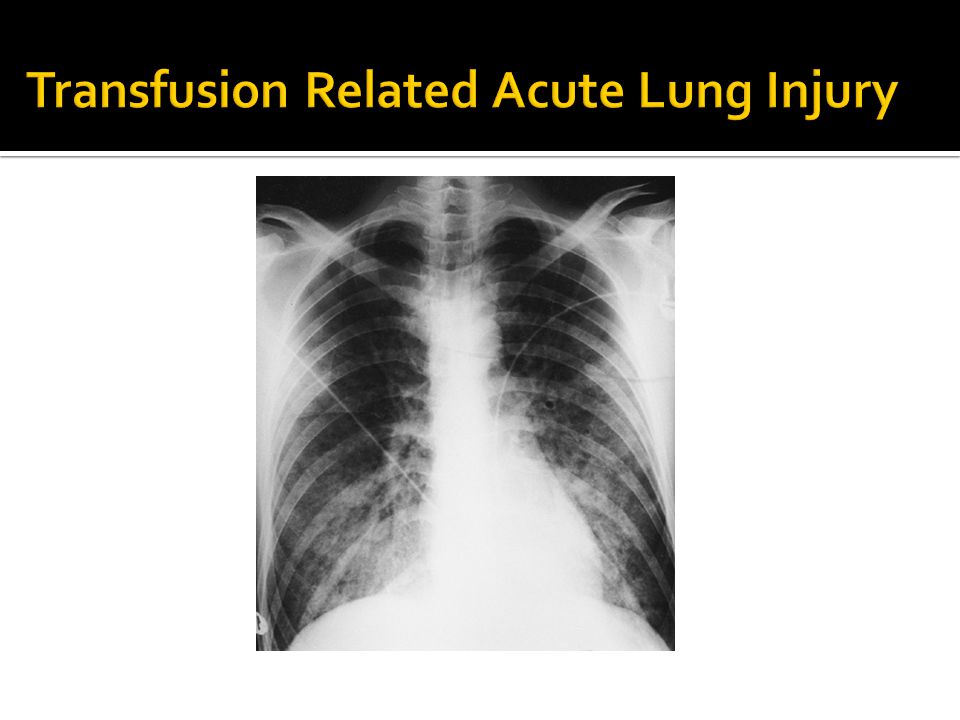
Pathogen Inactivation TRALI deferrals Blood conservation

27
Custer TMR 2009

28
Donor deferral Donor self-exclusion Transmissible disease testing HIV (antibody, NAT) HCV (antibody, RNA) Hepatitis B (surface antigen, DNA) Hepatitis B core Antibody Syphyllis HTLV I/II Chagas disease (implementation phase) Diversion pouch
 HCV (antibody, RNA) Hepatitis B (surface antigen, DNA) Hepatitis B core Antibody Syphyllis HTLV I/II Chagas disease (implementation phase) Diversion pouch")
29
HIV1: 2 – 3 million Hepatitis C1: 1 – 2 million Hepatitis B1: 150,000 HTLV1: 4.3 million 29

30
“It could therefore be argued that the PI of blood products represents the quintessence of the precautionary principle: almost all potential for transfusion-transmissible disease is eradicated often before the responsible agent is even recognized…” Alter, TMR 2008

32
Webert et al, Transfusion Medicine Reviews 2008

33
For plasma products only Effective against all enveloped viruses

38
Pooled platelets and plasma prepared with plasma from male donors (2007) Female donors with prior pregnancy are excluded from donating platelets (2009)
 Female donors with prior pregnancy are excluded from donating platelets (2009)")
39
Optimal use of Blood Products Autologous Transfusions Blood Substitutes

40
RBC transfusion trigger 70 g/dL (n= 418) vs. 100 g/dL (n= 420) in critically ill patients (Hebert, NEJM 1999)
 in critically ill patients (Hebert, NEJM 1999).")
41
PLT transfusion trigger of 10 x10 9 /L (n=135) vs 20 x10 9 /L (n=125) in patients with acute leukemia (Rubella, NEJM 1997)
 vs 20 x10 9 /L (n=125) in patients with acute leukemia (Rubella, NEJM 1997)")
42
Bone Marrow Transplantation, 2006

43
1091 units of plasma transfused for INR 1.1 – 1.85; follow up testing available on 324 units (Dzik, Transfusion 2006)
")
44
0 10 20 30 40 50 60 70 Phase IPhase IIPhase III FFP Orders (%) Inconsistent/ Inappropriate Inconsistent/ Appropriate Consistent P= 0.07 P= 0.03 P= 0.87 Arnold et al, ASH 2009
 Inconsistent/ Inappropriate Inconsistent/ Appropriate Consistent P= 0.07 P= 0.03 P= 0.87 Arnold et al, ASH 2009")
47
CBS to manage donors for solid organ transplantation. Merge clinical and laboratory TM. Unified approach to donors (CBS) and recipients (hospitals). Need for rigorous RCTs with meaningful clinical endpoints. Determination of reasonable cost-effectiveness. Re-evaluation of Krever recommendations; optimal utilization of blood products.
 and recipients (hospitals). Need for rigorous RCTs with meaningful clinical endpoints. Determination of reasonable cost-effectiveness. Re-evaluation of Krever recommendations; optimal utilization of blood products..")
48
Fundamental changes to TM in Canada since Krever 1997 Precautionary Principal Arms-length governance From “reactive” to “proactive” Blood conservation, optimal utilization continues to be a key safety issue

Similar presentations




















:>")






