Download presentation
Presentation is loading. Please wait.

1
Identifying and responding to deteriorating patients
17th Sept 2012

2
This session ... Harvest learning Create momentum Drive change
Although we are making progress

3
Webex Intro

5
Welcome & introductions Dr Brian Robson Executive Clinical Director
Item Speaker Time Welcome & introductions Dr Brian Robson Executive Clinical Director Healthcare Improvement Scotland 9am (10 mins ) The Australian Approach Dr Nicola Dunbar Program Manager Australian Commission on Safety and Quality in Health Care The national approach – policy and standards 9.10am (30 mins) Dr Tony Burrell Director Patient Safety NSW Clinical Excellence Commission Improving recognition in New South Wales The Scottish Approach Martin Carberry Consultant Nurse – Critical Care NHS Lanarkshire How is my Board improving early recognition, rescue and timely, appropriate treatment? 9.40am (15 mins) Ronnie Dornan Clinical Nurse Specialist, Critical Care Outreach NHS Borders 9.55am Ronnie Monaghan Head of E Health Programmes NHS Fife 10.10am The Amber Bundle Dr Elizabeth Ireland National Clinical Lead for Palliative and End of Life Care Scottish Government Supporting end of life decision making & communication – The Amber Bundle. 10.25am (15 mins ) Discussion on Scotland’s approach. All 10.40 am Close 10.55 am
 The Australian Approach. Dr Nicola Dunbar. Program Manager. Australian Commission on Safety and Quality in Health Care. The national approach – policy and standards. 9.10am. (30 mins) Dr Tony Burrell. Director Patient Safety. NSW Clinical Excellence Commission. Improving recognition in New South Wales. The Scottish Approach. Martin Carberry. Consultant Nurse – Critical Care. NHS Lanarkshire. How is my Board improving early recognition, rescue and timely, appropriate treatment 9.40am. (15 mins) Ronnie Dornan. Clinical Nurse Specialist, Critical Care Outreach. NHS Borders. 9.55am. Ronnie Monaghan. Head of E Health Programmes. NHS Fife am. The Amber Bundle. Dr Elizabeth Ireland. National Clinical Lead for Palliative and End of Life Care. Scottish Government. Supporting end of life decision making & communication – The Amber Bundle am. (15 mins ) Discussion on Scotland’s approach. All am. Close am.")
6
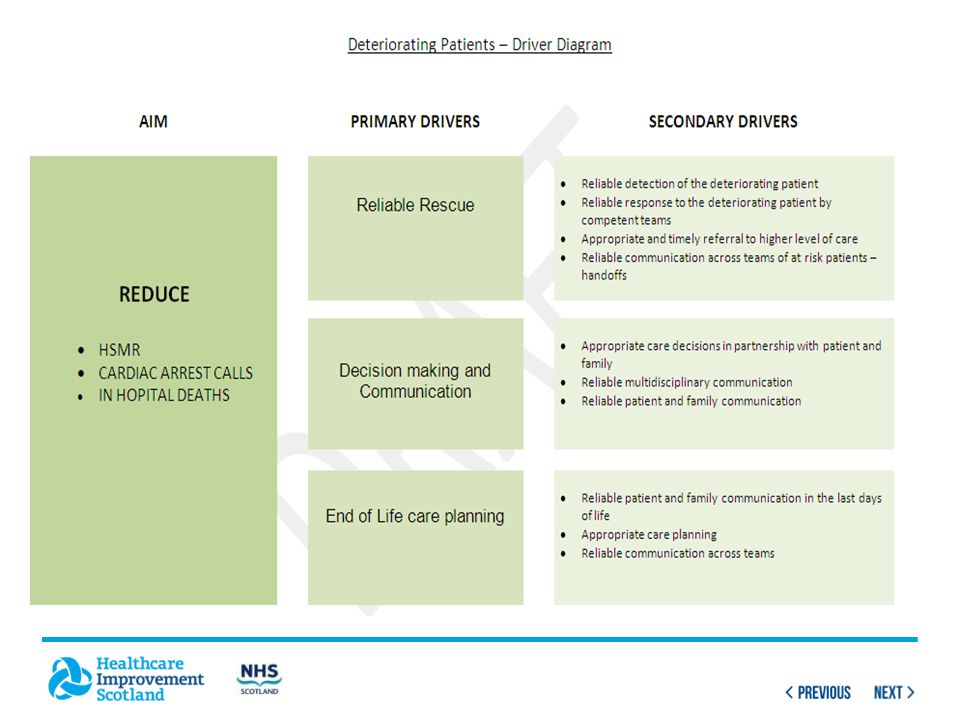
Reliable Rescue in Scotland
Detection, Planning and Response Phase 2 SPSP: the next steps

7
NHSScotland HSMR to March 2012 – ↓10.6%

8
Phase 2 SPSP - reliable rescue is in the wedge
HSMR Trajectory Phase 2 SPSP - reliable rescue is in the wedge Dec 2015 20% Reduction in HSMR 10.6% Reduction in HSMR

9
Learning session 9 8th-9th Nov 2012

10
International learning

11
A national approach to recognising and responding to clinical deterioration
Healthcare Improvement Scotland, 17 September, 2012

12
Where have we come from? METs spread widely and relatively quickly in Australia Source: Jones et al, Critical Care, 2008

13
Evidence base still developing:
increasing focus on recognition of deterioration new questions being identified and answered not yet an agreed best practice approach Failures still occurring Lots of local initiatives Programs at jurisdictional level (eg Between the Flags) International priority
 International priority.")
14
Australian Commission on Safety and Quality in Health Care
Established in 2006 to lead and coordinate safety and quality nationally Public and private sectors, acute and primary care settings Key functions: set national standards develop accreditation schemes data and indicator development monitor, report and publish knowledge and leadership for safety and quality Do this through processes of consultation and collaboration

15
ACSQHC: Recognising and Responding to Clinical Deterioration program
Initial priorities: Consensus Statement regarding essential elements of care for patients whose condition is deteriorating Implementation guide for using the Consensus Statement Evidence-based observation chart to prompt action National Safety and Quality Standard National survey of recognition and response systems

16
National Consensus Statement
Endorsed by Health Ministers in 2010: Measurement and documentation of observations Escalation of care Rapid response systems Clinical communication Organisational supports Education Evaluation, audit and feedback Technological systems and solutions

17
National Safety and Quality Health Service Standards
Health Ministers requested the Commission review safety and quality accreditation standards in 2006 Central components: National Safety and Quality Health Service Standards national coordination of accreditation Objectives: improve safety and quality for patients using the National Safety and Quality Health Services Standards as the focus for action implement coordinated and consistent accreditation via an Australian Health Services Safety and Quality Accreditation Scheme Hospitals and day procedure services to be assessed against NSQHS Standards from January 2013

18
National Safety and Quality Health Service Standards
Governance for Safety and Quality in Health Service Organisations Standard 2 Partnering with Consumers Standard 3 Healthcare Associated Infections Standard 10 Preventing Falls and Harm from Falls Standard 4 Medication Safety Standard 9 Recognising and Responding to Clinical Deterioration in Acute Health Care Standard 5 Patient Identification and Procedure Matching Standard 8 Preventing and Managing Pressure Injuries Standard 7 Blood and Blood Products Standard 6 Clinical Handover 18

19
Standard 9: Recognising and responding to clinical deterioration
Health service organisations establish and maintain systems for recognising and responding to clinical deterioration. Clinicians and other members of the workforce use the recognition and response systems. Two overarching Standards: Standard 1: Governance for Safety and Quality Standard 2: Partnering with Consumers

20
Four criteria Establishing recognition and response systems
Organisation-wide systems consistent with the National Consensus Statement are used to support and promote recognition of, and response to, patients whose condition deteriorates in an acute health care facility Recognising clinical deterioration and escalating care Patients whose condition is deteriorating are recognised and appropriate action is taken to escalate care Responding to clinical deterioration Appropriate and timely care is provided to patients whose condition is deteriorating Communicating with patients and carers Patients, families and carers are informed of recognition and response systems and can contribute to the processes of escalating care

21
Nature of the recognition and response systems can vary depending on:
Standards specify what needs to be achieved – how that occurs depends on context, eg: 9.4.1 Mechanisms are in place to escalate care and call for emergency assistance 9.6.2 A system is in place for ensuring access at all times to at least one clinician, either on-site or in close proximity, who can practise advanced life support Nature of the recognition and response systems can vary depending on: size and location of the health service nature of health services provided (eg ICU vs no ICU) nature and skill mix of workforce (eg no on-site doctors)
 nature and skill mix of workforce (eg no on-site doctors)")
22
Summary Recognising patients whose condition is deteriorating and responding to their needs in an appropriate and timely way are essential components of safe and high quality care – recognised as a national priority Purpose of the Standard is to improve outcomes for patients by ensuring that there is a systematic approach in place for recognising and responding to clinical deterioration

23
Tony Burrell, Mary Fullick, Lisa Coombs, Ann Callaway
SEPSIS KILLS: Partnering with clinicians to improve the recognition and management of sepsis Tony Burrell, Mary Fullick, Lisa Coombs, Ann Callaway

24
Why worry about sepsis? Increasing incidence High costs
Estimated 18 million cases per year worldwide > 17,000 cases per year in Australia NSW expected increase by 60% High costs Sepsis ALOS 11.1 days vs 2.9 days in 2009/10 in NSW1 Difficult to recognise Signs and symptoms of sepsis can be subtle especially in the elderly 40-50% of patients will not have a temperature 1 CEC Cost Effectiveness Analysis: Sepsis Kills – Dec 2011

25
Disease of the elderly

26
Type of physiological abnormality at time of ED patient inclusion in audit (first signs of sepsis) n=626 – median age 73 years Gray et al Emerg Med J 2012

27
In NSW... High number of sepsis adverse events related to delayed or inadequate recognition and management of sepsis CEC Sepsis Clinical Focus Report 2009 No sepsis clinical guidelines in 50% Emergency Departments (CEC, 2010)
")
28
QSA - Challenges in managing septic patients

29
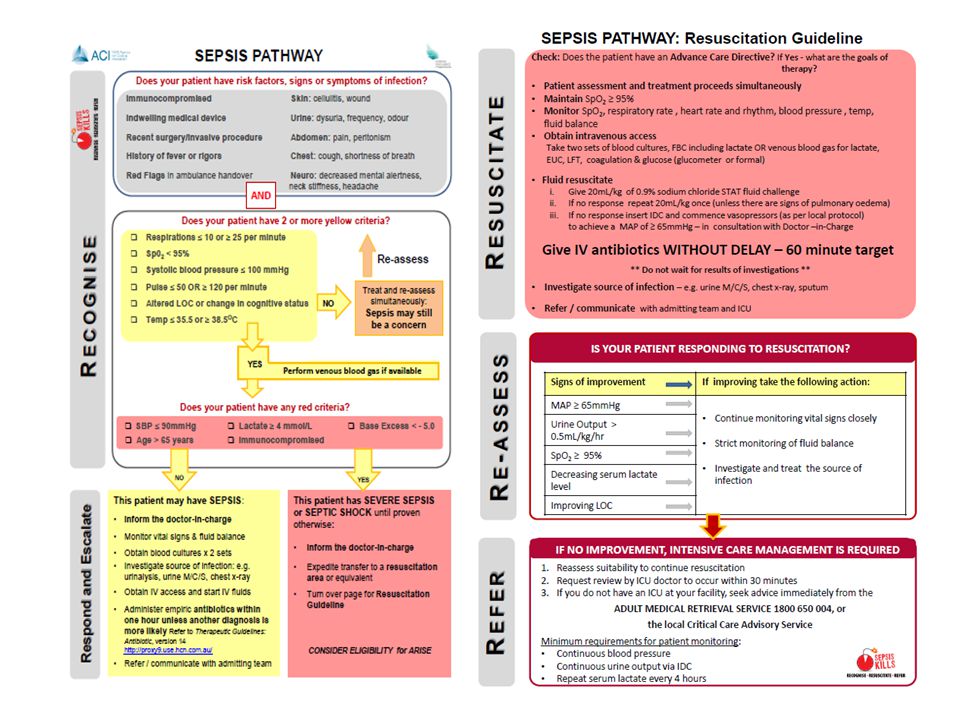
SEPSIS KILLS program RECOGNISE: Improve the early identification of septic patients RESUSCITATE: Implement best practice with rapid antibiotics and IV fluids REFER: Improve communication and transitions of care Sepsis is a medical emergency!

30
‘We recommend the protocolised resuscitation of a patient with sepsis-induced shock, defined as tissue hypoperfusion (hypotension persisting after initial fluid challenge or blood lactate concentration 4mmol/L). This protocol should be initiated as soon as hypoperfusion is recognised and should not be delayed pending ICU admission’ ‘We recommend that IV antimicrobial therapy be started as early as possible and within the first hour of recognition of septic shock (1B) and severe sepsis without septic shock (1C)’. Surviving sepsis 2012 (in draft)
 and severe sepsis without septic shock (1C)’. Surviving sepsis 2012 (in draft)")
31
Phased implementation
Emergency Departments Clinician focused bottom up approach Phase 2.1 Smaller hospitals and Emergency Departments Clinical Governance support, strong clinical leads Bottom up, top down approach Phase 2.2 Large facilities Executive, Clinical governance and clinician support

33
Variations in practice…
Variations in empiric antibiotic prescription guideline for first dose Variations in antibiotic availability particularly in smaller rural hospitals Variations in antibiotic administration - emphasis on infusion - gentamicin particular issue Fluids ?too much caution Awaiting results of ARISE, PROMISE (UK), POCESS (US)
, POCESS (US)")
34
NSW time to initiation of antibiotics Jan 2011 –Sept 2012

35
NSW Sepsis Data 2011 (preliminary)
Mortality No benefit Antibiotics ≤60 minutes = median 5 days >60 minutes = median 5 days no significant difference in median LOS <60 minutes (mean=5.72hrs) with admission to ICU >60 minutes (mean=6.86hrs) with admission to ICU no significant difference
 with admission to ICU. >60 minutes (mean=6.86hrs) with admission to ICU. no significant difference.")
36
NSW Sepsis Data 2011 – lactate
Analysis to date… Confirms value of point of care lactate testing

37
Hypotensive (SBP<90) N=94
NSW Sepsis Data 2011 Cryptic shock (Normotensive (SBP>90) and lactate >3 (N=86) V. lactate ≤3 (N=356)) 4.8 RR of death with lactate >3 (p<0.000) 2.4 RR of admission to ICU with lactate >3 (p<0.011) Hypotensive (SBP<90) N=94 Death 5.1 times more likely than patients with SBP>90 (25.5% - 24/94) (p=0.000) With triage 3-5, death 4.3 times more likely than patients with SBP>90 and triage 3-5 (p=0.018) No significant difference in death using variables SBP and time to antibiotics (p=0.254)
 and lactate >3 (N=86) V. lactate ≤3 (N=356)) 4.8 RR of death with lactate >3 (p<0.000) 2.4 RR of admission to ICU with lactate >3 (p<0.011) Hypotensive (SBP<90) N=94. Death 5.1 times more likely than patients with SBP>90 (25.5% - 24/94) (p=0.000) With triage 3-5, death 4.3 times more likely than patients with SBP>90 and triage 3-5 (p=0.018) No significant difference in death using variables SBP and time to antibiotics (p=0.254)")
38
Lessons learnt from phase 1….
69% > 60 years old Triage category matters 21.5% mortality rate for patients triage 3 Lactate is a valuable investigation Should observations be done routinely at triage? Delay to medical review Delay to antibiotics

39
Phase 2.2 Large facilities Wards complex – diffused responsibility
Pilot site – now working up project in 2 wards in large teaching hospital Wards complex – diffused responsibility Relationship with BTF, ‘In Safe Hands’ Difficult to coordinate Pharmacy Heads of department IC ID Surveillance

40
Cause and effect diagram – SEPSIS KILLS
Knowledge Lack of knowledge in relation to the management of sepsis Pathology People Lack of knowledge in relation to recognition of sepsis Time to pathology results Lack of understanding of blood results Delays in Rapid Response Skill mix Communication JMO’s not aware to take a venous blood gas Timely communication of results Education Lack of venous blood gases in inpatient environment Reduced staffing after hours Lack of knowledge and uncertainty about appropriate antibiotic use Lack of availability of blood culture bottles Skill set Delayed recognition and management of sepsis Lack of SEPSIS KILLS Links with DETECT training Data collection IV cannulation IV antibiotic administration culture Antimicrobial stewardship Failure to take and record vital signs Delayed charting of IV antibiotics Drug committee sign off Failure to escalate deteriorating patients Local pharmacy guidelines Antibiotic availability Delays to stat IV antibiotics administration Measurements Policy Medications

41
Strong Executive Support
Pharmacy Clinical Governance Heads of Department Infectious Diseases Pathology Medical and Nursing staff Rapid Response teams Intensive care Strong Clinical Champions/Leads

42
Questions?

43
“Deteriorating Patients” NHS Lanarkshire
Martin Carberry Consultant Nurse Critical Care

44
Hairmyres Wishaw Monklands 3 DGH acute hospitals 550 000 population
1600 acute beds HECT - look after Hosp at night (2004) and day duty follow up / ward trawls / sick patient support No “ formal ” out reach service Monklands
 and day duty follow up / ward trawls / sick patient support. No formal out reach service. Monklands.")
45
Agenda Brief Overview some work in NHS Lanarkshire
1 Clinical Support Workers Course (CSW): CRASH (Csw Recognition Assessment Support & Help) 2 The use of clinical trigger questions to help identify sick ward based patients
: CRASH (Csw Recognition Assessment Support & Help) 2 The use of clinical trigger questions to help identify sick ward based patients.")
46
CRASH set up Part of a tiered education programme
Four hour course / ran monthly HECT (Hospital Emergency Care Team) faculty Short lectures / workshops / group work - Followed by clinical scenarios - look listen & feel approach HECT follow up CSWs to support competencies
 faculty. Short lectures / workshops / group work. - Followed by clinical scenarios. - look listen & feel approach. HECT follow up CSWs to support competencies.")
47
Why CRASH ? Failure to recognise sick patients
HECT Prospective MEWS audits - inaccurate - infrequent - over reliance on “machines” “Non touch ….. non feel” No support for CSW doing the “Obs” No structured Handover / feedback to RGN Bottom of the bed test ? MEWS Pre CRASH Observed CSW in wards Discussed potential support – what would they want – asked CSWs what they needed No assessment skills – basics – How to record Obs only Bottom of bed – does the MEWS match the patient – does the MEWS match the patient ?

48
CRASH Evaluation CRASH - Evaluations (Data to follow)
CSWs - value system for CSWs - culture change - Follow up and feel supported MEWS - repeat audits pre and post CRASH - improved ? - sustained? “ in it for the long haul ” Two areas – CWs feedback 1 Questionnaire 2 MEWS full audits – two wards improved (limited data to date) identification of sick patients should improve as should handover to RGNs Outcome ? Cardiac arrest ? Pre monitory signs picked up ?
 identification of sick patients should improve as should handover to RGNs. Outcome Cardiac arrest Pre monitory signs picked up")
49
Length of course – some wanted more than 4 hours
- Would mean a greater problem releasing CSW from ward areas Interactive group work – very well received – involved – CSW felt they had a VALUED input Most would recommend CRASH

50
CSW Quotes Re : CRASH “ Why can’t there be more like this”
“ Learned about sepsis ” “ Should be rolled out to all the wards” “ More about Sepsis” “ Importance of respiratory rate ” “ More aware of MEWS ” “ The effective use of SBAR ” “ Small details count make you look at the big picture “ Strong Value and believe they are listened too CSW – felt – investment in them and welcomed help

51
HECT “Clinical Trigger Questions”
HECT nurse will ask ward nurses at every ward trawl: 1. Increasing frequency : Observations / MEWS 2. O2 - high flow 3. Out of hours review (or any ITU) 4. Fast fluids / Blood / Drug Infusions HECT nurse will then decide if the patient requires assessment / intervention / referral Introduced date Jun 2011 HECT nurse will decide if the patient requires HECT intervention / referral / assessment One ward – 3 wards etc amended roll out PDSAs Teaching launch Safety Brief
 4. Fast fluids / Blood / Drug Infusions. HECT nurse will then decide if the patient requires. assessment / intervention / referral. Introduced date Jun HECT nurse will decide if the patient requires HECT intervention / referral / assessment. One ward – 3 wards etc amended roll out. PDSAs. Teaching launch. Safety Brief.")
52
Why Trigger Questions? Examples of good work other Health boards
Evidence base (e.g. NCEPOD) Failure to Flag up on routine trawls “Any patients you are worried about ? ” MEWS only ? - patients compensating - score of < 4 - but sick … or SIRS? Support ward staff - use of O2, IV drug infusions - opportunity for clinical teaching Borders, A & A and Newcastle - No formal outreach SIRS – score 2 but not triggered MEWS Staff not aware fast fluids or high flow FiO2 – potentially sick patient Education too - NHSL ALERT – modified sepsis / monthly - CSWs on crash happy to speak up
 Failure to Flag up on routine trawls. Any patients you are worried about MEWS only - patients compensating. - score of < 4 - but sick … or SIRS Support ward staff. - use of O2, IV drug infusions. - opportunity for clinical teaching. Borders, A & A and Newcastle. - No formal outreach. SIRS – score 2 but not triggered MEWS. Staff not aware. fast fluids or high flow FiO2 – potentially sick patient. Education too. - NHSL ALERT – modified sepsis / monthly. - CSWs on crash happy to speak up.")
53
Trigger Question Evaluation Study (2012)
Aims To determine nursing staff awareness of T/Q To determine nursing staff usefulness & value of T/Q To determine HECT nurse frequency of using T/Q Methods Mail shot questionnaire Three acute hospitals 12 questions - based on content / construct validity

54
Trigger Question Response Rates
Resp Rate overall 61% Majority RGNs ( 65% plus) are experienced at > 6yrs
 are experienced at > 6yrs.")
55
Trigger Question (T/Q) study - some results
Yes % (n) No Not Spec Can you recall all four T/Q 81.2% (n=315) 15.5% (n=60) 2.6% (n=10) Did the T/Q change your perception of what makes a patient at risk of deterioration 56.8% (n=219) 42.0% (n=162) 1.0% (n=4) Do you think the T/Q improve the identification of sick patients 85.7% (n=330) 13.5% (n=52) 0.7% (n=3) Do you think the T/Q improve referral of sick patients to HECT 87.5% (n=337) 12% (n=46) 0.5% (n=2) Are T/Q useful in helping student nurses recognise sick patients 96.1% (n=370) 3.4% (n=13) Q. Are you aware of T/Q = Yes - 98% of staff aware Perception – Think questions are very helpful for junior staff. I would expect senior staff nurses and above to recognise a sick patient. Fantastic tool although clinical judgement comes with experience. Nurses rely too much on trigger questions bud do not look at their patient or listen to them when they are unwell because their MEWS is less than four. As a nurse who rotates onto night duty I feel I often see situations with sick patients who have been unstable throughout the day and it is no until overnight that they are dealt with to a satisfactory conclusion. It is important to understand that a patient can be deteriorating without any of the trigger questions being positive. Sometimes I have seen nurses being to reliant on these questions but overall they are helpful. Do the student nurses really know the trigger questions? Feel the tool is most helpful to less experienced staff. Identification = T/Q - did not improve identification of sick patients = 52 staff Below are the reasons why: 25 staff - They can use clinical judgement and experience to identify sick patients without the use of the trigger questions. (25 members of staff stated this) Unsure if the trigger questions are used in their unit. Some staff do not use the trigger questions. Factors out with trigger questions may influence review. Some patient's answer no to all the questions however still requires review. High MEWS score and observations alert us of sick patients. The questions do not always cover who is at risk. All patients have the potential to deteriorate. Sometimes find that a high number of patients do not answer yes to any of the questions however are still referred to HECT
 No. Not. Spec. Can you recall all four T/Q. 81.2% (n=315) 15.5% (n=60) 2.6% (n=10) Did the T/Q change your perception of what makes a patient at risk of deterioration. 56.8% (n=219) 42.0% (n=162) 1.0% (n=4) Do you think the T/Q improve the. identification of sick patients. 85.7% (n=330) 13.5% (n=52) 0.7% (n=3) Do you think the T/Q improve referral of sick patients to HECT. 87.5% (n=337) 12% (n=46) 0.5% (n=2) Are T/Q useful in helping student nurses recognise sick patients. 96.1% (n=370) 3.4% (n=13) Q. Are you aware of T/Q = Yes - 98% of staff aware. Perception – Think questions are very helpful for junior staff. I would expect senior staff nurses and above to recognise a sick patient. Fantastic tool although clinical judgement comes with experience. Nurses rely too much on trigger questions bud do not look at their patient or listen to them when they are unwell because their MEWS is less than four. As a nurse who rotates onto night duty I feel I often see situations with sick patients who have been unstable throughout the day and it is no until overnight that they are dealt with to a satisfactory conclusion. It is important to understand that a patient can be deteriorating without any of the trigger questions being positive. Sometimes I have seen nurses being to reliant on these questions but overall they are helpful. Do the student nurses really know the trigger questions Feel the tool is most helpful to less experienced staff. Identification = T/Q - did not improve identification of sick patients = 52 staff. Below are the reasons why: 25 staff - They can use clinical judgement and experience to identify sick patients without the use of the trigger questions. (25 members of staff stated this) Unsure if the trigger questions are used in their unit. Some staff do not use the trigger questions. Factors out with trigger questions may influence review. Some patient s answer no to all the questions however still requires review. High MEWS score and observations alert us of sick patients. The questions do not always cover who is at risk. All patients have the potential to deteriorate. Sometimes find that a high number of patients do not answer yes to any of the questions however are still referred to HECT.")
56
T/Q Study Staff Quotes “ Fantastic tool though clinical judgement comes with experience ” “ Feel the tool is most helpful to less experienced staff ” “ I would expect senior staff nurses and above to recognise a sick patient ” “ Factors out with trigger questions may influence review ” “ Do the student nurses know the trigger questions ” “ I find them a really useful prompt ” “ Its becoming a habit to think of them.. ” Note : experience quote - (25 staff) said recognising sick patients comes with experience University – MEWS / Recognition / T/Q teaching to support for junior staff
 said recognising sick patients comes with experience. University – MEWS / Recognition / T/Q teaching to support for junior staff.")
57
T/Q Study Limitations One study one Health Board Hawthorne effect
Hect influence - response rate - bias Although 3 acute hospitals – one board Seen us coming ! Increased response rate due to HECT ?

58
Trigger Questions : referrals HECT and cardiac arrest rates
S/A = Short Assessments performed by the HECT nurse: - Asked to see patients by ward staff - ITU follow up - Planned review (already on case load) Short Assessments – are / interventions - asked to see patients / ITU step down reviews / case load reviews / tracheotomy reviews
 Short Assessments – are / interventions - asked to see patients / ITU step down reviews / case load reviews / tracheotomy reviews.")
59
Thanks to Sanjiv Chohan – work on data
Pilot trigger questions Thanks to Sanjiv Chohan – work on data Short Assessments – are / interventions / asked to see patients / ITU step down reviews / case load reviews / tracheotomy reviews Annotations – pilot Jan / Feb 2011 – Introduced wards May / Jun 2011 – research questionnaire to wards Feb & Mar 2012 HECT – patient referrals from ward staff and interventions increased due to introduction of T/Q Cardiac Arrests – no obvious change during this period 3 hospitals – similar patterns – next slides Working on data collection for breakdown of Asked to see – Q. How many interventions / what type / and outcome – escalation / DNACPR etc

60
Pilot trigger questions

62
In Summary CRASH - hands on approach working well Trigger Questions
- CSW follow up is key to sustainability Trigger Questions - perceived improved identification & handover - perceived as important tool for less experienced staff - staff feel valued & supported - no change in arrest calls during this period - increased referrals & interventions to HECT

63
Thank you … Questions ? Acknowledgement Dr Sanjiv Chohan (Data analysis)
")
64
Borders General Hospital
Population 112,870 Ronnie Dornan Clinical Nurse Specialist Critical Care Outreach Team

66
Critical Care Outreach Referral
SBAR Cards Critical Care Outreach Referral S Situation Immediate Help Name Ward Reason for referral HR, RR,T, WCC, BP, SpO2, GCS, UO Resuscitation Status B Background Admission Date & Time Reason for Admission Treatment A Assessment State what you think the problem is : Respiratory Genitourinary Cardiac Neurological Gastrointestinal Pain R Recommendation State what you want done Time frame ABG, U&E, FBC, Lactate, CXR

67
Nurses Physiotherapists Doctors Critical Care Outreach Hospital at Night Acute Pain Service Patients & Relatives Anaesthetists Critical Care Outreach

68
Review all patients who trigger 2 boxes on SIRS/Shock chart
Non judgemental, non punitive response to all referrals Hospital wide approach to early identification Follow up of all patients discharged from ITU (Discharge Summary) Proactive approach to the identification of the at risk patient Induction programme on the “at risk” early warning scoring system for nurses, doctors and students High Dependency Nursing Skills Course for nurses, midwives, AHP Medical and Nursing Student placements with Outreach Team Monthly case note review of all arrest calls Monthly random case note review (Scottish Patient Safety Programme)
 Proactive approach to the identification of the at risk patient. Induction programme on the at risk early warning scoring system for nurses, doctors and students. High Dependency Nursing Skills Course for nurses, midwives, AHP. Medical and Nursing Student placements with Outreach Team. Monthly case note review of all arrest calls. Monthly random case note review (Scottish Patient Safety Programme)")
70
Patientrack Current Scope
On ward observation capture and real time EWS At a glance ward & hospital(s) view 24 X 7 mobile chart NHS Fife DECT Phones Automated clinical alerts Flexible reports
 view. 24 X 7 mobile chart. NHS Fife DECT Phones. Automated clinical alerts. Flexible reports.")
71
Opportunities Assessments and Screenings
Information sharing “beyond the walls of the hospital” Collaboration and Research

72
Assessments & Screenings
Part of national, regional and local safety and quality initiatives (NHS Scotland Collaborative on Sepsis and VTE, CQUIN, QIPP, Harmfreecare...) Typically, implemented using paper forms and manual processes - tends to be time-consuming and resource-intensive, with the potential for late of missed assessments and errors Sharing of data between assessments, and with teams, is problematic Opportunity to create a database for monitoring, notifications, review, planning, research and improvement is lost
 Typically, implemented using paper forms and manual processes - tends to be time-consuming and resource-intensive, with the potential for late of missed assessments and errors. Sharing of data between assessments, and with teams, is problematic. Opportunity to create a database for monitoring, notifications, review, planning, research and improvement is lost.")
73
Assessments & Screenings
Opportunity - Simple Add-On to the Existing Patientrack System Same on ward devices and log-ons as for Patientrack Composite ward / hospital view of all assessments for patients; when scheduled and when due / missed Pick assessment required based on local rules Timed Events & Workflow Engine Patientrack & Assessments Database Embedded logic and “show hide”. Data gathering easy and quick at the bedside Reports and extracts

74
Assessments & Screenings
VTE Example Use national and local VTE assessment policy to define the clinical workflow and data capture logic Configure the workflow, such as the rules for which patients are to receive assessments, and what events (e.g. on admission) or timings (e.g. 24 hours post admission) initiate the assessment Configure the on-form logic and flow, such as the mandatory fields and the “show hide” for sections of the assessment or individual values Define the internal and external reports and extracts that may be required
 or timings (e.g. 24 hours post admission) initiate the assessment. Configure the on-form logic and flow, such as the mandatory fields and the show hide for sections of the assessment or individual values. Define the internal and external reports and extracts that may be required.")
75
Optional or Trigger Event (e.g. 24 hours following admission)
Assessments & Screenings VTE Example e.g. Report on VTEs required or compliance with VTE protocol e.g. Extract to portal Clerking In Reports and Extracts Optional or Trigger Event (e.g. 24 hours following admission) VTE Assessment On Admission VTE Assessment Patients Details Patientrack Database Discharge GP Discharge Report Allows VTE Assessment to be made on admission and then at any point necessary on the patient journey, using hospitals own rules
 VTE Assessment. On Admission VTE Assessment. Patients Details. Patientrack Database. Discharge. GP Discharge Report. Allows VTE Assessment to be made on admission and then at any point necessary on the patient journey, using hospitals own rules.")
76
Assessments & Screenings
A number of assessments are available “out of the box” VTE, Sepsis, Fluid Balance, Peripheral & Central IV Line Management, Urinary Catheter Management, Blood Sugar & Urinary Ketones, Nutritional (MUST) Assessment, MRSA Screening, Stool Chart & C. Diff Screening New assessments are planned or can be quickly developed Falls, Pressure Ulcers, Dementia Toolkit available for sites to develop their own assessments
 Assessment, MRSA Screening, Stool Chart & C. Diff Screening. New assessments are planned or can be quickly developed. Falls, Pressure Ulcers, Dementia. Toolkit available for sites to develop their own assessments.")
77
Information Sharing Push and Pull Access Services On discharge VTE or Dementia Assessment Community Health Partnership Patientrack & Assesments Database Augmented Discharge Summary GPs Secure Access Information collected in hospital that is appropriate and useful to other organisations is made available; for example to GPs, Community Health Partnerships or other Health Boards

78
Maintained Database Environment
Collaboration and Research Secure Access Central Manchester Extracts & Analyses Maintained Database Environment NHS Fife Research Access Analytics Toolkit Western Sussex Extract, Translate & Load (ETL) Services Academic Institutions Determine research interests alongside other sites Develop joint proposals for funding Share research
 Services. Academic Institutions. Determine research interests alongside other sites. Develop joint proposals for funding. Share research.")
79
Implementing the AMBER care bundle in your hospital
29th March 2012

80
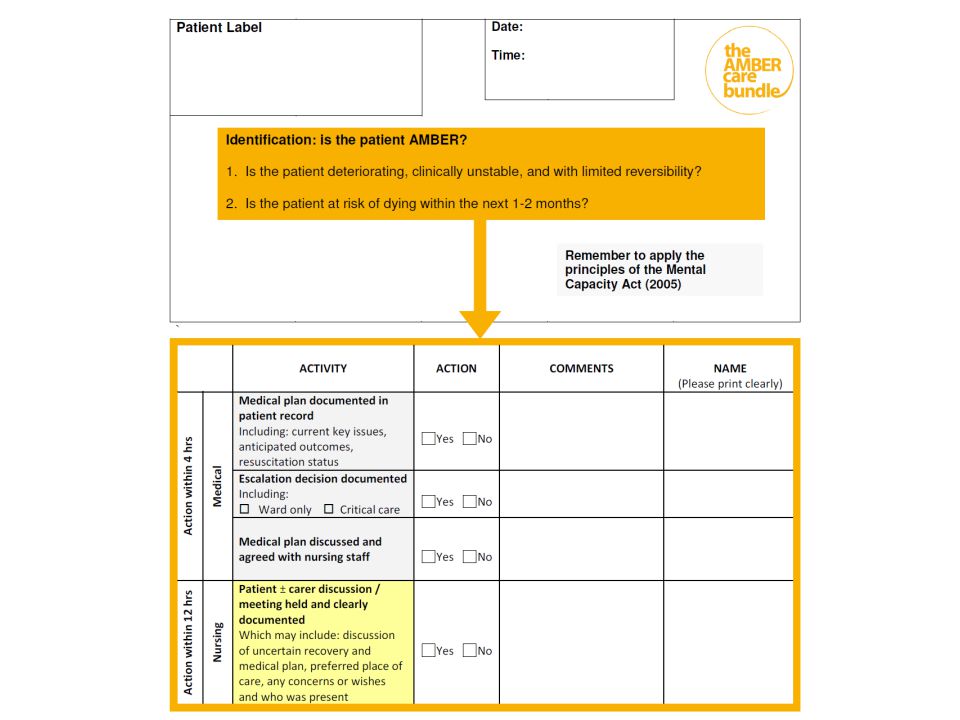
Objectives how to implement and sustain the AMBER care bundle in your hospital build on your experience of implementing LCP / or equivalent be aware of the available materials and resources understand the AMBER network: support and expectations

81
Patients whose recovery is uncertain

83
And daily ACT: Day one: identification and initiation AMBER follow-up
A “Is patient still AMBER?” C “Has medical plan Changed?” T Touch base with carers - Is everything OK?”

84
Impact What we found out: Medical decision making inconsistent
Ineffective communication within team Patient/carer discussions did not include: Preferences Uncertainty What we’re doing differently: Generating multidisciplinary team discussion and understanding Consultant support for escalation framework where uncertainty exists Early pro-active patient/ carer discussions about uncertain recovery and preferences Systematic follow-up Reliability

85
Case study 76 year old man with pulmonary fibrosis and exacerbation of COPD. Deterioration, extreme shortness of breath, poor prognosis, had capacity. Patient aware of illness however was not aware of the severity. Relatives lived far away and had not been informed of admission. Patient identified as AMBER. Discussion with patient and team took place. Following patient consent relatives were contacted.

86
Case study Comments from Patients/Staff/Relatives:
“ AMBER helped us to address issues in a timely manner. It was so great to be able to get the patient home. “ We had no idea that Bill was so unwell. At least now we can help him sort things out” relative “ I have not been well for a while. I didn’t know how to tell my family. I just really want to get home, I do not want to die in hospital. nurse “ I think AMBER has helped staff to escalate decisions and has highlighted the importance of communication at all levels. patient consultant

88
AMBER 1st January ’10 – 29th February ’12
Total AMBER patients Median no. of days on AMBER 757 7.0 Still in ward Died in hospital on AMBER Died in hospital on LCP Discharged to community 6 125 201 415 0.7% 16.5% 26.6% 54.8% Recovered Other 7 3 0.9% 0.4% Hospital survival rate >2 weeks 26% >1 month 10% >2 months 3%

90
Hospital survival rates: Jan 2010-Jun 2011

91
Hospital and community survival rates: Jan 2010-Jan 2011

92
Outcomes Emergency readmissions (30d): 14% vs 35%*
>70% die in their preferred place of care *2010 figures GSTT following discharge Significantly fewer emergency readmission rates for AMBER patients who were discharged: 14% compared to 35% when compared with patients who died within 100 days of discharge in the same wards*

93
In-patient deaths: monthly
Median=91 Median=83 Statistically significant shift p <

94
Interface: the AMBER care bundle, LCP and in-patient mortality

95
Hospital wide implementation
Adrian Hopper

96
Hospital ready for change
Senior leaders demonstrate support Need for AMBER is recognised Fits into hospital initiatives LCP established / palliative care influential Practical support / project support in place

97
Guidance AMBER Network 1. Hospital wide engagement
2. Hospital wide preparation 3. Ward / team implementation 4. Making it stick: ward sustainability 5. Making it stick: hospital sustainability Tools Guidance Resources Experience Website AMBER Network

98
Engagement Who Where 3. How Heat map Enthusiasm Local priority
Specialty (oncology, older person, acute med) 3. How - Patient stories / sentinel events
 3. How. - Patient stories / sentinel events.")
99
Interfaces LCP Critical care outreach Hospital at night
Others: COPD outreach, Older Person’s liaison Productive ward

100
Board Another group to influence - Their duty to improve EOLC
- Patient stories - Data Connect to the strategic agenda Business case

101
Cardiac arrests GSTT (excluding CCU and ICU)
")
102
Contacts

Similar presentations










>")
 LIZ PRICE (CNS, BRADFORD) WENDY LAYCOCK (FACILITATOR, AWC) Clinically Based Education and Training Initiative.>")












![Presented by [Insert name of presenter] [Insert title] [Insert LHD/SHN name] Month 2014 PD2014_030 Using Resuscitation Plans in End of Life Decisions.](/12/3498778/big_thumb.jpg "Presented by [Insert name of presenter] [Insert title] [Insert LHD/SHN name] Month 2014 PD2014_030 Using Resuscitation Plans in End of Life Decisions.>")
