Download presentation
Presentation is loading. Please wait.

1
Beverly Begovich RN, MBA Pat Turbiville February 7 , 2013
An Evidence Based Practice for Patient Centered Care: Discharge Phone Calls Beverly Begovich RN, MBA Pat Turbiville February 7 , 2013 © Baptist Leadership Group, MMX. All rights reserved.

2
Post Visit/Discharge Calls
A best practice to assure continuity of care and a thorough understanding of how to transition safely to home and self care.

3
Post Visit Calls BLG Post Visit Calls Traditional
Focused on improving patient satisfaction only Inconsistent Process Serves as a stop gap for service failure Little follow-up action with learnings Focused on quality and service of the patient experience Follows a detailed protocol and process Confirms compliance and demonstration of understanding of the discharge instructions Has accountability for follow up Ensures a safe transition to home

4
OR

5
Discharge Phone Calls The intent of Discharge Phone Calls is not to increase the patient’s perception of care. Discharge phone calls primary purpose is to impact clinical outcomes. Finally discharge phone calls harvest staff recognition, audit the patient’s perception of care improve processes based on patient feedback.

6
© Baptist Leadership Group, MMX. All rights reserved.
Why is it important? HCAHPS is a call to action to manage patients from the hospital to the discharge process. © Baptist Leadership Group, MMX. All rights reserved.

7
Annals of Internal Medicine February 2003
“Nearly 1 in 5 patients”* Type of Adverse Events 400 patients surveyed Other 76 (19%) had adverse events after discharge Fall 8% Nosocomial Infection 4% 5% Adverse Drug Event Procedure Related 66% 17% * 81 events occurred in 76 patients * “Adverse Events After Discharge from Hospital”, Annals of Internal Medicine, February 2003
 had adverse events after discharge. Fall. 8% Nosocomial Infection. 4% 5% Adverse Drug Event. Procedure Related. 66% 17% * 81 events occurred in 76 patients. * Adverse Events After Discharge from Hospital , Annals of Internal Medicine, February")
8
Video on people understanding
© Baptist Leadership Group, MMX. All rights reserved.

9
Ineffective Communication
This is a tremendous Risk factor for readmissions Only 42% of patients knew diagnosis Only 28% knew medication names Only 37% knew purpose of medication Only 14% knew side effects Discharge Calls can bridge the gaps. State University of New York Study Mayo Clinic Proceedings, August 2005

10
Tactics to support patient centered care:
Words that work Service behaviors such as responsiveness to call lights Hourly rounding Leader rounding on patients Discharge Phone Calls Staff feedback Process Improvements

11
Post-Visit Calls- Big results for 5 minutes!
Confirms compliance and understanding of discharge instructions Reduces complaints and claims, affords opportunity for service recovery Allows for harvesting of positives for reward and recognition Identifies process improvement opportunities Confirms that hospital CARES about patient

12
Implementation Strategy:
Methodology & Consistent Protocol Using the defined script, harvest information Take Action: Address Clinical needs; Reward & coach

13
Timeline for Implementation of Discharge Phone Calls
Each LHP facility to identify a “site administrator” for ED and Inpatients calls who will receive additional training on the D/C call software. This is the first line “troubleshooter” per facility. March 1, 2013 Implement ED D/C Phone call process Each LHP facility will initiate their Inpatient Discharge Phone Call process based on readiness decided by their coach and Senior Leaders.

14
Phased implementation process
Phase 1: Emergency Department call backs Implement based on a specific population Clarify the script to be used including documentation of “notification/schedule of call on DC instructions” Establish who will make the calls Capture the data in the BLG/Eclipse Discharge Call Software

15
Discharge Phone Calls for the Emergency Department
The purpose of Discharge phone calls in the Emergency Department is to assure the patient follows through with their instructions to assure an optimum outcome and to evaluate whether there is any further progression of their condition that may placed them in jeopardy if left untreated. For this reason Baptist Leadership Group recommends the following group of high risk patients be identified for a post visit call at the time of discharge. This list can be adjusted based on the input from the Medical Director of the Emergency Department. High Risk Patient’s discharged to home to be called back within hours post discharge: Abdominal Pain Chest Pain Head Injury Fever of Undetermined Origin Children under the age of 1 Elderly that had fallen Left without seen and AMA Patient’s with severe neurological changes

16
Guidelines for Implementing the Discharge Phone Call Process
Set the Goal : Decide the expected outcome from making the Discharge Calls ie Decrease # of readmissions for COPD; decrease # ED readmits; improve patient satisfaction etc. 2. Decide how many patients you will call and how many attempts you will make to reach the patient. An example of this is to call 100% of all COPD patients up to three attempts within the first 72 hours of discharge.

17
Guidelines Process continued
Who: 1. Decide who will make the phone calls Best Practice is nurse caring for patient at time of discharge or Charge Nurse on unit familiar with patient condition. If the caller is not the nurse who cared for patient, the caller should be a clinical person using a script. The guidelines for questions should be clear and a decision tree should be in place in case of clinical questions. Recommended a clinical person be within the area. 2. Decide who they will call: Identify targeted population to begin the process. Choosing limited population allows you to create a process that works. © Baptist Leadership Group, MMX. All rights reserved.

18
Guidelines for Process cont
When: Decide what the initial timeframe for post-discharge calls should be to make the call. ( Best Practice <24h) 2. Decide how many attempts will be made to contact the patient. Decide what message should be left on voice mail. 3. Decide how to set the expectation for the patient at discharge that they can expect a discharge phone call ( consider documenting and validating on DC instruction sheet) 4. Create plan to inform patient of plan to call at time of discharge using words that work. “ Part of excellent care here at ____- is making sure our patients understand all their instructions so I will be calling you tomorrow afternoon, is this the correct phone number to reach you at?”
 2. Decide how many attempts will be made to contact the patient. Decide what message should be left on voice mail. 3. Decide how to set the expectation for the patient at discharge that they can expect a discharge phone call ( consider documenting and validating on DC instruction sheet) 4. Create plan to inform patient of plan to call at time of discharge using words that work. Part of excellent care here at ____- is making sure our patients understand all their instructions so I will be calling you tomorrow afternoon, is this the correct phone number to reach you at")
19
Guidelines for process cont.
What: 1.Decide how to capture feedback from the phone call and what information is needed to make the call such as having a copy of the discharge instructions available either electronically or hard copy ( front sheet/discharge instructions). 2. Decide what action should be taken if concern or complaint is raised 3. Decide what will be documented in the medical record or in the Discharge Call Software Program. 4. Consider guidelines for documentation when there is a follow up medical need /change in condition that should be added to EMR © Baptist Leadership Group, MMX. All rights reserved.
. 2. Decide what action should be taken if concern or complaint is raised. 3. Decide what will be documented in the medical record or in the Discharge Call Software Program. 4. Consider guidelines for documentation when there is a follow up medical need /change in condition that should be added to EMR. © Baptist Leadership Group, MMX. All rights reserved.")
20
Guidelines for process continued
Where: 1. Decide on where information is shared, how frequently reviewed and how questions/data is interpreted for trends for performance improvement © Baptist Leadership Group, MMX. All rights reserved.

21
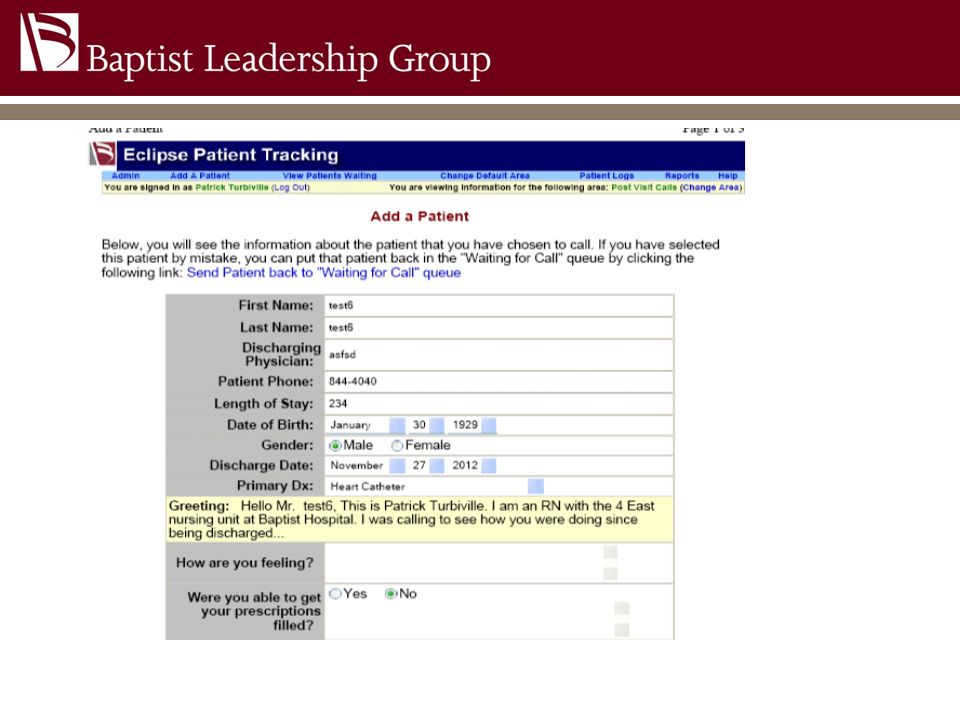
How do we do discharge phone calls?
Review the phone script that includes: Empathy and concern and uses WTW Clinical Outcomes Reward & Recognition Understanding patient’s perception of care Gather process improvement suggestions

22
Emergency Phone Script:
Discharge Phone Call Script for Emergency Rooms: Hello I am ____________, a Nurse from________________ calling you back following your visit to our emergency department on ________________. I want to make sure you are doing ok and answer any questions you may have regarding the instructions that were given to you to care for yourself at home. Have you improved since the visit? ___________________________________ Have you gotten any prescriptions filled that were ordered at the time of discharge?__________________________________________________ Do you have any questions regarding the medications you are taking?_____________________________________________________ Were you able to make arrangements for a follow up appointment if one was recommended?_______________________________________________ Can you share with me how your experience was at the Emergency Department with the Physician and Nursing staff?____________________________________ We like to recognize our employees for providing very good care. Was there anyone you would like us to recognize?____

24
Track findings to include the following:
Patient Name Discharge Date Date and Time of 1st Call Voice Mail/Left Message Date and Time of 2nd Call Date and Time of 3rd Call Empathy and Concern Clinical Outcomes Medications Home Care Follow-up Appointment Reward and Recognition Process Opportunities

25
Next Steps: Finalize process for your Hospital
Discuss plan for implementation with your unit based council or staff Develop 90 day plan to implement discharge phone calls Role model making the discharge phone calls to pilot the process Implement discharge phone calls Communicate back to staff wins and opportunities for improvement from the discharge phone calls Track success rate and evaluate effectiveness of calls.

26
Questions?

27
Thank you!

Similar presentations