Download presentation
Presentation is loading. Please wait.

1
BOTOX® The Real Facts David H. Hammett, M.D. Neurology March 26, 2012

2
4540 Trenholm Road Columbia, SC 29206 (803) 790-4700
")
3
3

4
4

5
Presentation Overview
Introduction to BOTOX® How does BOTOX® Work? BOTOX® in the Treatment of Blepharospasm BOTOX® in the Treatment of Cervical Dystonia BOTOX® for Severe Primary Axillary Hyperhidrosis BOTOX® in the Treatment of Spasticity BOTOX® in the Treatment of Chronic Migraine Important Information About BOTOX® 5

6
History In the 1820s, the biological basis for food poisoning was not understood. Studies began on a batch of improperly prepared sausages responsible for the death of several dozen people in Germany. First suggestion that there was something in the spoiled sausages that brought on the disease. These experiments led to a better understanding of the neurological symptoms of food-borne botulism (ptosis, dysphagia, muscle weakness, and, if left untreated, paralysis and respiratory failure).
.")
7
History More than 70 years later, Dr. Emile Pierre van Ermengem of Belgium was asked to investigate an outbreak of botulism following a funeral dinner where three people died and 23 were paralyzed. Van Ermengem was able to make a connection between botulism and a spore-forming bacterium he named Bacillus botulinus (now known as Clostridium botulinum). Many scientific studies followed, and seven strains of botulinum toxin were eventually identified (A-G).
. Many scientific studies followed, and seven strains of botulinum toxin were eventually identified (A-G).")
8
History In 1978, an Opthalmologist (Dr.Scott) received approval to inject minute amounts of botulinum toxin into human volunteers. In the early 1980s, he published a number of studies including a paper in the Transactions of the American Ophthalmological Society that asserted botulinum toxin “appears to be a safe and useful therapy for strabismus.” Additional research showed the drug’s benefits went beyond ophthalmology, providing patients with temporary relief from facial spasms, neck and shoulder spasms, even vocal cord spasms.

9
History In 1988, drugmaker Allergan acquired the rights to distribute Scott’s batch of botulinum toxin type A (or Oculinum, as it was then known) and a year later, the FDA approved botulinum toxin type A for the treatment of both strabismus and blepharospasm. Shortly thereafter, Allergan acquired Scott’s company and changed the drug’s name to the compact, catchy “Botox.”
 and a year later, the FDA approved botulinum toxin type A for the treatment of both strabismus and blepharospasm. Shortly thereafter, Allergan acquired Scott’s company and changed the drug’s name to the compact, catchy Botox.")
10
Timeline – Development and FDA
1950s Scientists discover that botulinum toxin can reduce muscle spasms. 1960s/1970s Studies explore botulinum toxin as a treatment for strabismus (crossed eyes). Allergan researches other medical uses of botulinum toxin. Allergan introduces BOTOX®, the first botulinum toxin approved by the FDA to treat blepharospasm (eyelid spasms) and strabismus. FDA approves BOTOX® for cervical dystonia 10
 Allergan researches other medical uses of. botulinum toxin. Allergan introduces BOTOX®, the first botulinum. toxin approved by the FDA to treat blepharospasm. (eyelid spasms) and strabismus FDA approves BOTOX® for cervical dystonia. 10.")
11
Timeline – Development and FDA
2002 FDA approves BOTOX® Cosmetic, (same formulation as BOTOX®) for moderate to severe frown lines between the brow. 2004 FDA approves BOTOX® for severe underarm sweating year anniversary of BOTOX®. FDA approves BOTOX® for upper limb spasticity. 2010 BOTOX® is approved by the FDA specifically for the prevention of headaches in adults with Chronic Migraine (15 or more days each month with headache lasting 4 or more hours each day) 2011 FDA approval for neurogenic urinary incontinence 11
 for moderate to severe frown lines between the brow FDA approves BOTOX® for severe underarm sweating year anniversary of BOTOX®. FDA approves BOTOX® for upper limb spasticity BOTOX® is approved by the FDA specifically for the prevention of headaches in adults with Chronic Migraine (15 or more days each month with headache lasting 4 or more hours each day) 2011 FDA approval for neurogenic urinary incontinence. 11.")
12
Glabellar Frown Lines Glabellar frown lines are the most common reason for cosmetic injection of botulinum toxin.

13
NOTE TO PRESENTER: 13

15
It is important to note that blepharospasm is considered to be a disorder of the VII nerve. Blepharospasm involves a dysfunction of the basal ganglia. Blepharospasm has been well studied with appropriately designed and scaled clinical trials. This is one reason the Food and Drug Administration (FDA) granted approval of BOTOX® treatment for blepharospasm in 1989. 15
 granted approval of BOTOX® treatment for blepharospasm in")
16
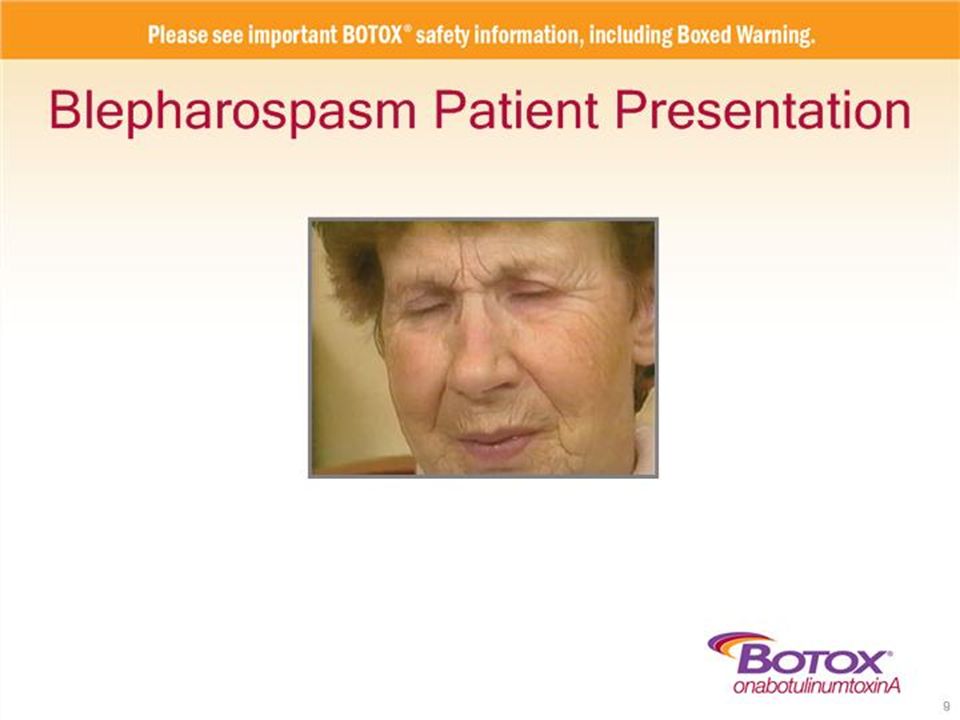
Patients diagnosed with blepharospasm have normal eyes and vision; however, the muscle spasms may leave their eyelids completely closed, causing functional blindness.3,4,6 Daily activities, eg, driving, walking, and reading, are affected.7 Blepharospasm affects about 32 per 100,000 people, predominantly females (3:1).7 The age of onset is usually between the fifth and sixth decade and women are, on average, 4.7 years older than men.5,7 References 3. National Institute of Neurological Disorders and Stroke, National Institutes of Health, US Department of Health and Human Services. Dystonias fact sheet. National Institute of Neurological Disorders and Stroke Web site. Published December Updated April 24, Accessed June 11, 2009. 4. Langlois M, Richer F, Chouinard S. New perspectives on dystonia. Can J Neurol Sci. 2003;30(suppl 1): 34S-44S. 5. Hallett M. Blepharospasm: recent advances. Neurology. 2002;59(9): 6. Benign Essential Blepharospasm Research Foundation (BEBRF). BEBRF blepharospasm pages. Benign Essential Blepharospasm Research Foundation (BEBRF) Web site. Accessed June 11, 2009. 16
.7. The age of onset is usually between the fifth and sixth decade and women are, on average, 4.7 years older than men.5,7. References. 3. National Institute of Neurological Disorders and Stroke, National Institutes of Health, US Department of Health and Human Services. Dystonias fact sheet. National Institute of Neurological Disorders and Stroke Web site. Published December Updated April 24, Accessed June 11, Langlois M, Richer F, Chouinard S. New perspectives on dystonia. Can J Neurol Sci. 2003;30(suppl 1): 34S-44S. 5. Hallett M. Blepharospasm: recent advances. Neurology. 2002;59(9): Benign Essential Blepharospasm Research Foundation (BEBRF). BEBRF blepharospasm pages. Benign Essential Blepharospasm Research Foundation (BEBRF) Web site. Accessed June 11,")
17
Occurs spontaneously, but may be aggravated by stress, reading, driving, fatigue, or other external stimuli such as bright lights, wind, or smoke.4,5 The risk of developing blepharospasm increases with family history of dystonia, prior eye disease, or head trauma with loss of consciousness.5 Risk factors leading to the spread of blepharospasm to other muscles include older age at onset, female gender, and prior head or face trauma.5 References 4. Langlois M, Richer F, Chouinard S. New perspectives on dystonia. Can J Neurol Sci. 2003;30(suppl 1):34S-44S. 17
:34S-44S. 17.")
18
This figure depicts common blepharospasm injection sites for use with BOTOX® neurotoxin.
There are 3 common injection sites: medial and lateral pretarsal orbicularis oculi of the upper lid and the lateral pretarsal orbicularis oculi of the lower lid.1 Note: Although a wide range of injection techniques have been documented, there is no standard protocol for treatment.13 Avoid medial lower lid injections.1 This will reduce diffusion into the inferior oblique and may reduce the complication of diplopia.1 Avoid injection near the levator palpebrae superioris (muscles that retract the upper eyelids).1 This may reduce the complication of ptosis.1 Ecchymosis occurs easily in the soft eyelid tissues.1 This can be avoided by applying pressure at the injection site immediately after the injection.1 References BOTOX® Prescribing Information, 2009. 10. Netter FH. Atlas of Human Anatomy. 4th ed. Philadelphia, PA: Saunders Elsevier; 2006. 11. Kendall FP, McCreary EK, Provance PG, Rodgers MM, Romani WA. Muscles: Testing and Function with Posture and Pain. 5th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2005. 12. Sommer B, Lowe N. Cosmetic indications. In: Moore P, Naumann M, eds. Handbook of Botulinum Toxin Treatment. 2nd ed. Malden, MA: Blackwell Science; 2003: 18
.1 This may reduce the complication of ptosis.1. Ecchymosis occurs easily in the soft eyelid tissues.1 This can be avoided by applying pressure at the injection site immediately after the injection.1. References. BOTOX® Prescribing Information, Netter FH. Atlas of Human Anatomy. 4th ed. Philadelphia, PA: Saunders Elsevier; Kendall FP, McCreary EK, Provance PG, Rodgers MM, Romani WA. Muscles: Testing and Function with Posture and Pain. 5th ed. Baltimore, MD: Lippincott Williams & Wilkins; Sommer B, Lowe N. Cosmetic indications. In: Moore P, Naumann M, eds. Handbook of Botulinum Toxin Treatment. 2nd ed. Malden, MA: Blackwell Science; 2003:")
19
The use of BOTOX® (onabotulinumtoxinA) in the management of blepharospasm is well documented. In the last 10 years, thousands of patients have been effectively treated. This slide shows a woman with blepharospasm before and after BOTOX® treatment. 19

20
This slide shows the results of the open-label study of 27 patients with essential blepharospasm.15
The versatility of BOTOX® treatment allows it to provide reliable efficacy in the small muscles injected to treat blepharospasm. BOTOX® treatment had an improvement rate of 93% within 48 hours postinjection.15 The effect of BOTOX® treatment lasts for approximately 3 months.1 References 1. BOTOX® Prescribing Information, 2009. 20

21
NOTE TO PRESENTER: A thorough explanation of the safety information of BOTOX® (Botulinum Toxin Type A) is a key part of every Leader’s Edge meeting; therefore, a dedicated safety module will be automatically included in your module selection. Please ensure that the safety information slides are covered in full and that you refer back to the safety information when answering related questions. 21
 is a key part of every Leader’s Edge meeting; therefore, a dedicated safety module will be automatically included in your module selection. Please ensure that the safety information slides are covered in full and that you refer back to the safety information when answering related questions. 21.")
22
Dystonia is a syndrome of sustained, involuntary muscular contractions, often causing twisting or repetitive movements, or abnormal postures.1 Cervical dystonia (CD) is a chronic neurological disorder that affects the muscles of the neck, producing patterned, repetitive, and spasmodic or sustained muscle contractions resulting in abnormal movements and postures of the head and neck.2 CD is classified as a focal dystonia because it typically affects 1 area of the body (ie, head and neck).1 References Fahn S. Dystonia. In: Jankovic J, Hallett M, eds. Therapy With Botulinum Toxin. New York, NY: Marcel Dekker, Inc; 1994: 2. Jankovic J. Treatment of cervical dystonia. In: Brin MF, Comella CL, Jankovic J, eds. Dystonia: Etiology, Clinical Features, and Treatment. Philadelphia, PA: Lippincott, Williams & Wilkins; 2004: 22
.1. References. Fahn S. Dystonia. In: Jankovic J, Hallett M, eds. Therapy With Botulinum Toxin. New York, NY: Marcel Dekker, Inc; 1994: Jankovic J. Treatment of cervical dystonia. In: Brin MF, Comella CL, Jankovic J, eds. Dystonia: Etiology, Clinical Features, and Treatment. Philadelphia, PA: Lippincott, Williams & Wilkins; 2004:")
23
This video sequence shows various cervical dystonia patients presenting with a range of symptoms.
23

24
Cervical dystonia is the most common form of focal dystonia.2
It is characterized by involuntary, patterned muscle contractions in the head and neck area that cause the abnormal movements or posturing of the head and neck. The patterned nature of the muscle contractions helps distinguish cervical dystonia from tics and other hyperkinetic disorders. The condition can be spasmodic, with involuntary muscular contractions or convulsive motions, or sustained, with continuous tension or contraction of muscles.2 Most dystonic movements have a directional component and are a combination of the following head positions: backward (retrocollis), lateral (laterocollis), rotational (torticollis), or forward (anterocollis). References 2. Jankovic J. Treatment of cervical dystonia. In: Brin MF, Comella CL, Jankovic J, eds. Dystonia: Etiology, Clinical Features, and Treatment. Philadelphia, PA: Lippincott, Williams & Wilkins; 2004: 3. Van Zandijcke M. Cervical dystonia (spasmodic torticollis). Some aspects of the natural history. Acta Neurol Belg. 1995;95(4): 24
, lateral (laterocollis), rotational (torticollis), or forward (anterocollis). References. 2. Jankovic J. Treatment of cervical dystonia. In: Brin MF, Comella CL, Jankovic J, eds. Dystonia: Etiology, Clinical Features, and Treatment. Philadelphia, PA: Lippincott, Williams & Wilkins; 2004: Van Zandijcke M. Cervical dystonia (spasmodic torticollis). Some aspects of the natural history. Acta Neurol Belg. 1995;95(4):")
25
The clinical features of cervical dystonia vary widely among individual patients.8
Clinical features include involuntary, abnormal head and neck movements and posturing (eg, twisting, turning, tilting, and extending).8 In most patients the abnormal posturing is present about 75% of the time, but can change during the course of the disorder.8 Many patients use sensory tricks or gestes antagonistes that temporarily diminish symptoms.8 Neck pain occurs in up to 80% of patients.8 The pain can be intermittent or continuous. Typically it is diffuse and widespread over the shoulder and neck, with some radiation usually on the side toward which the head is twisted.8 Thirty percent of patients experience head tremor (ie, dystonic tremor).3 Diagnosis is often delayed 1 year or more, and it is common for mild cases of cervical dystonia to go undiagnosed.3 References 3. Van Zandijcke M. Cervical dystonia (spasmodic torticollis). Some aspects of the natural history. Acta Neurol Belg. 1995;95(4): 8. Stacy M. Idiopathic cervical dystonia: an overview. Neurology. 2000;55(12 suppl 5):2S-8S. 25
.8 In most patients the abnormal posturing is present about 75% of the time, but can change during the course of the disorder.8. Many patients use sensory tricks or gestes antagonistes that temporarily diminish symptoms.8. Neck pain occurs in up to 80% of patients.8 The pain can be intermittent or continuous. Typically it is diffuse and widespread over the shoulder and neck, with some radiation usually on the side toward which the head is twisted.8. Thirty percent of patients experience head tremor (ie, dystonic tremor).3. Diagnosis is often delayed 1 year or more, and it is common for mild cases of cervical dystonia to go undiagnosed.3. References. 3. Van Zandijcke M. Cervical dystonia (spasmodic torticollis). Some aspects of the natural history. Acta Neurol Belg. 1995;95(4): Stacy M. Idiopathic cervical dystonia: an overview. Neurology. 2000;55(12 suppl 5):2S-8S. 25.")
26
We are now looking at a photograph of a patient with cervical dystonia.
26

27
We are now looking at a photograph of another patient with cervical dystonia.
27

28
Cervical dystonia can be a lifelong condition.3
Cervical dystonia frequently begins as a pulling or drawing sensation in the neck or an involuntary twisting or jerking of the head.8 Neck pain at onset is also very prominent.3 After onset, symptoms typically worsen for an average of 3 to 5 years, although the time course is highly variable (range, 1 month to 18 years).8 In about one-third of patients, the dystonia spreads beyond the neck but rarely becomes generalized.8 Involvement of the arms, jaw, and trunk are most common.2 Remissions occur in up to 20% of patients, but are usually short-lived and incomplete. Remissions usually occur within the first few years of onset but may occur later in the disease course. Remissions may be sustained but almost all patients relapse within 5 years, and a cycle of remission and relapse may occur.8 References 2. Jankovic J. Treatment of cervical dystonia. In: Brin MF, Comella CL, Jankovic J, eds. Dystonia: Etiology, Clinical Features, and Treatment. Philadelphia, PA: Lippincott, Williams & Wilkins; 2004: 3. Van Zandijcke M. Cervical dystonia (spasmodic torticollis). Some aspects of the natural history. Acta Neurol Belg. 1995;95(4): 8. Stacy M. Idiopathic cervical dystonia: an overview. Neurology. 2000;55(12 suppl 5):2S-8S. 28
.8. In about one-third of patients, the dystonia spreads beyond the neck but rarely becomes generalized.8 Involvement of the arms, jaw, and trunk are most common.2. Remissions occur in up to 20% of patients, but are usually short-lived and incomplete. Remissions usually occur within the first few years of onset but may occur later in the disease course. Remissions may be sustained but almost all patients relapse within 5 years, and a cycle of remission and relapse may occur.8. References. 2. Jankovic J. Treatment of cervical dystonia. In: Brin MF, Comella CL, Jankovic J, eds. Dystonia: Etiology, Clinical Features, and Treatment. Philadelphia, PA: Lippincott, Williams & Wilkins; 2004: Van Zandijcke M. Cervical dystonia (spasmodic torticollis). Some aspects of the natural history. Acta Neurol Belg. 1995;95(4): Stacy M. Idiopathic cervical dystonia: an overview. Neurology. 2000;55(12 suppl 5):2S-8S. 28.")
29
The chart shows the key findings, all of which are statistically significant:
Pain relief, the light purple portion of the chart, occurred at weeks 1 through 8 for the 50-, 100-, and 150-U groups. Muscle contraction relief, the gold overlay of the chart, was concurrent with pain relief at weeks 2 through 8 for the 100- and 150-U groups. As you can see, pain relief began earlier and at lower doses than muscle contraction relief.5 Reference 5. Relja M, Telarovic S. Botulinum toxin type-A and pain responsiveness in cervical dystonia: a dose response study. Presented at: 9th International Congress of Parkinson’s Disease and Movement Disorders; March 5-8, 2005; New Orleans, LA. 29

31
Now let’s examine the disease state known as severe primary axillary hyperhidrosis that is inadequately managed with topical agents. NOTE TO PRESENTER: 31

32
Hyperhidrosis is defined as severe sweating beyond that which is needed to cool the body. Excessive sweating may be exacerbated by anxiety or stress, which in turn can increase anxiety and stress. 32

33
Diagnosis should be made only after excluding secondary causes of excessive sweating.
After secondary causes have been excluded, recommended diagnostic criteria for severe primary axillary hyperhidrosis have recently been defined by a group of internationally recognized experts as follows2: Focal, visible, excessive sweating of at least 6 months’ duration with at least 2 of the following characteristics2: Bilateral and relatively symmetric Impairment in daily activities Age of onset less than 25 years Positive family history Cessation of focal sweating during sleep Reference 33

34
The treatment algorithm listed on this slide was developed by the Multi-Specialty Working Group on the Recognition, Diagnosis, and Treatment of Primary Focal Hyperhidrosis, a multidisciplinary task force of internationally recognized experts in the field, funded in part by Allergan. This algorithm represents evidence-based guidelines that were developed for primary, focal axillary hyperhidrosis through an exhaustive and critical review of the literature; a manuscript containing these recommendations was recently published in the Journal of the American Academy of Dermatology.2 The first recommended step in treatment is to ensure that the patient has appropriately used over-the-counter antiperspirants and to verify that he or she understands the difference between deodorant and antiperspirant.2 The second recommended step in treatment is to initiate therapy with topical aluminum chloride hexahydrate in absolute alcohol or salicylic acid gel. This treatment can cause skin irritation that may be minimized by using a lower concentration of aluminum chloride, applying to dry skin at bedtime, and/or applying hydrocortisone cream to the affected area.2 Patients who have failed to respond to the previously described topical therapies may undergo BOTOX® intradermal injections.2 If patients fail to respond to the aforementioned treatments, surgery may be indicated. Surgical removal of the overactive sweat glands may be performed using subcutaneous curettage, endoscopic thoracic sympathectomy, or other procedures. It is recommended that patients be seen by the surgeon and a dermatologist prior to surgery.2 Reference 34

35
Duration was also measured in a pivotal study, and BOTOX® patients achieved a median duration of response of 6.7 months, or 201 days.1 Duration was calculated as the number of days between BOTOX® injection and the date when patients first returned to level 3 or 4 on the HDSS Among patients who received a second BOTOX® injection, the median duration of response was similar to that observed after the first treatment One to 2 BOTOX® injections were sufficient for most BOTOX® responders Based on these results, follow-up injections for hyperhidrosis should be administered when the clinical effect of a previous injection diminishes Reference 35

37
37

38
The causes of spasticity are heterogeneous
The causes of spasticity are heterogeneous. While spasticity following stroke is a common etiology, spasticity can also occur in adults following head trauma, multiple sclerosis, spinal cord injury, intracranial tumor, and also, on rare occasions, degenerative central nervous system (CNS) disorders. Reference 10. Mostoufi SA. Spasticity and its management. Pain Management Rounds. 2005;2:1-6. 38
 disorders. Reference. 10. Mostoufi SA. Spasticity and its management. Pain Management Rounds. 2005;2:")
39
One typical synergy pattern of upper limb spasticity is flexed wrist
One typical synergy pattern of upper limb spasticity is flexed wrist. The main muscles that potentially contribute to the flexed wrist include flexor carpi radialis and flexor carpi ulnaris.29 Severe flexion of the wrist interferes with ADLs such as dressing and washing. Passive stretching of stiff flexors can be painful. Associated compression of the median nerve can produce carpal tunnel syndrome with hand pain.29 Carpal tunnel syndrome is a condition in which the median nerve, running from the forearm into the hand, is squeezed at the wrist. The carpal tunnel is a narrow passageway at the base of the hand made of ligaments and bones and houses the median nerve. Swelling of this tissue can cause the compression of the nerve, causing pain, swelling, or weakness in the hand and wrist.29,30 References 29. Mayer NH, Esquenazi A, Childers MK. Common patterns of clinical motor dysfunction. Muscle Nerve Suppl. 1997;6:S21-S35. 30. Neurotoxin Institute Web site. UMNS: Muscle Overactivity in the Upper Motor Neuron Syndrome. Accessed May 21, 2009. 39

40
Another typical synergy pattern of upper limb spasticity is “clenched fist,” or “intrinsic plus hand.” Patients with clenched fist have their fingers clasped into the palm. The intrinsics and the extrinsics may both be spastic, but an intrinsic plus posture is not seen because spastic extrinsic flexors dominate. Reduction of spasticity in the extrinsics may unmask spasticity in the intrinsics, potentially converting an extrinsic deformity into an intrinsic plus deformity.29 Muscles that potentially contribute to clenched fist include flexor digitorum profundus, flexor digitorum superficialis, and flexor pollicis longus. Muscles involved in intrinsic plus hand are the lumbricales.29-31 Patients with clenched fist are unable to open their hand. Access to the palm for washing and drying is difficult. Chronically restricted access may lead to skin maceration and breakdown. Fingernails tend to dig into the palm, causing pain. References 29. Mayer NH, Esquenazi A, Childers MK. Common patterns of clinical motor dysfunction. Muscle Nerve Suppl. 1997;6:S21-S35. 30.Neurotoxin Institute Web site. UMNS: Muscle Overactivity in the Upper Motor Neuron Syndrome. Accessed May 21, 2009. 31. Elovic EP, Brashear A, Kaelin D et al. Repeated treatments with botulinum toxin type a produce sustained decreases in the limitations associated with focal upper-limb poststroke spasticity for caregivers and patients. Arch Phys Med Rehabil. 2008;89(5): 40
:")
41
Pronated forearm is another typical synergy pattern of upper limb spasticity. The patient typically presents with a forearm that is pronated fully. It is commonly associated with a flexed elbow.30 Muscles involved include pronator quadratus and pronator teres.29,30 Patients with pronated forearm have difficulty orienting the hand. Many ADLs that depend on active pronation/supination movements of the forearm become restricted. Activities such as turning the hand, using eating utensils, washing face, reaching for objects, and shaking hands become difficult.29,30 References 29. Mayer NH, Esquenazi A, Childers MK. Common patterns of clinical motor dysfunction. Muscle Nerve Suppl. 1997;6:S21-S35. 30. Neurotoxin Institute Web site. UMNS: Muscle Overactivity in the Upper Motor Neuron Syndrome. Accessed May 21, 2009. 41

42
A final typical synergy pattern of upper limb spasticity is adducted or internally rotated shoulder. The patient typically has the arm adducted tightly, with the forearm lying against the middle of the chest.29 Muscles involved include pectoralis major (the upper fiber is involved in adducted shoulder and the lower fiber in rotated shoulder), latissimus dorsi (adduction), teres major (both adduction and rotation), subscapularis (rotation), and anteropr deltoid (both adduction and rotation).29 Patients with adducted/internally rotated shoulder often complain of pain and frozen shoulder. Severe adduction posturing and the resultant restricted motion limit the ability to orient the arm, to reach targets, or to apply force. It also interferes with ADLs such as dressing and bathing. Skin irritation, maceration, and odor in the axilla may occur.29,30 References 29. Mayer NH, Esquenazi A, Childers MK. Common patterns of clinical motor dysfunction. Muscle Nerve Suppl. 1997;6:S21-S35. 30. Neurotoxin Institute Web site. UMNS: Muscle Overactivity in the Upper Motor Neuron Syndrome. Accessed May 21, 2009. 42
, latissimus dorsi (adduction), teres major (both adduction and rotation), subscapularis (rotation), and anteropr deltoid (both adduction and rotation).29. Patients with adducted/internally rotated shoulder often complain of pain and frozen shoulder. Severe adduction posturing and the resultant restricted motion limit the ability to orient the arm, to reach targets, or to apply force. It also interferes with ADLs such as dressing and bathing. Skin irritation, maceration, and odor in the axilla may occur.29,30. References. 29. Mayer NH, Esquenazi A, Childers MK. Common patterns of clinical motor dysfunction. Muscle Nerve Suppl. 1997;6:S21-S Neurotoxin Institute Web site. UMNS: Muscle Overactivity in the Upper Motor Neuron Syndrome. Accessed May 21,")
43
43

44
Targeted therapy with onabotulinumtoxinA has been an approach that provides direct relief from upper limb spasticity. OnabotulinumtoxinA functions through inhibition of acetylcholine release at nerve terminals. Normally during neurotransmission, vesicle membranes fuse with those of the nerve terminals, releasing acetylcholine into the synaptic cleft. A family of proteins collectively called the SNARE proteins mediate this process. OnabotulinumtoxinA, taken up into vesicles, cleaves the SNARE proteins, preventing assembly of the fusion complex. This inhibitory effect reduces the number of presynaptic transmitter vesicles, impeding neuromuscular transmission and reducing the hypertonicity in the muscle.17 The targeted approach of onabotulinumtoxinA for upper limb spasticity therapy allows for a nonsystemic, selective isolation and reduction of hypertonicity of targeted muscles.2,18 Unlike surgery, the toxin effect is not permanent, as the effect only persists until new neuromuscular junction formation, which occurs within weeks or months.17 Physical therapy can be used with treatment.5,18 References 2. O'Brien CF. Treatment of spasticity with botulinum toxin. Clin J Pain. 2002;18(6 suppl):S182-S190. 5. Bergfeldt U, Borg K, Kullander K, Julin P. Focal spasticity therapy with botulinum toxin: effects on function, activities of daily living and pain in 100 adult patients. J Rehabil Med. 2006;38: 17. Rowland LP. Stroke, spasticity, and botulinum toxin. N Engl J Med. 2002;347: 18. Davis EC, Barnes MP. Botulinum toxin and spasticity. J Neurol Neurosurg Psychiatry. 2000;69: . 44
:S182-S Bergfeldt U, Borg K, Kullander K, Julin P. Focal spasticity therapy with botulinum toxin: effects on function, activities of daily living and pain in 100 adult patients. J Rehabil Med. 2006;38: Rowland LP. Stroke, spasticity, and botulinum toxin. N Engl J Med. 2002;347: Davis EC, Barnes MP. Botulinum toxin and spasticity. J Neurol Neurosurg Psychiatry. 2000;69:")
45
In clinical trials, doses ranging from 75 Units to 360 Units were divided among selected muscles at a given treatment session. The recommended dose ranges per muscle are as follows: Biceps Brachii: 100 – 200 Units divided in 4 sites Flexor Digitorum Profundus: 30 – 50 Units in 1 site Flexor Digitorum Sublimis: 30 – 50 Units in 1 site Flexor Carpi Radialis: 12.5 – 50 Units in 1 site Flexor Carpi Ulnaris: 12.5 – 50 Units in 1 site Reference 19. BOTOX® Prescribing Information. Irvine, CA; Allergan, Inc. 45

46
BOTOX® (onabotulinumtoxinA) for Chronic Migraine Patients: A Prophylactic Treatment Paradigm
Please see Indication, Important Limitations, and Important Safety Information, including Boxed Warning, throughout this deck. 46

47
Indication BOTOX® (onabotulinumtoxinA) for injection is indicated for the prophylaxis of headaches in adult patients with chronic migraine (≥15 days per month with headache lasting 4 hours a day or longer). Important limitations Safety and effectiveness have not been established for the prophylaxis of episodic migraine (14 headache days or fewer per month) in seven placebo-controlled studies. 47 47
 for injection is indicated for the prophylaxis of headaches in adult patients with chronic migraine (≥15 days per month with headache lasting 4 hours a day or longer). Important limitations Safety and effectiveness have not been established for the prophylaxis of episodic migraine (14 headache days or fewer per month) in seven placebo-controlled studies")
48
IMPORTANT SAFETY INFORMATION, INCLUDING BOXED WARNING
Distant Spread of Toxin Effect Postmarketing reports indicate that the effects of BOTOX® and all botulinum toxin products may spread from the area of injection to produce symptoms consistent with botulinum toxin effects. These may include asthenia, generalized muscle weakness, diplopia, ptosis, dysphagia, dysphonia, dysarthria, urinary incontinence, and breathing difficulties. These symptoms have been reported hours to weeks after injection. Swallowing and breathing difficulties can be life threatening, and there have been reports of death. The risk of symptoms is probably greatest in children treated for spasticity, but symptoms can also occur in adults treated for spasticity and other conditions, particularly in those patients who have an underlying condition that would predispose them to these symptoms. In unapproved uses, including spasticity in children, and in approved indications, cases of spread of effect have been reported at doses comparable to those used to treat cervical dystonia and at lower doses. Please see additional Important Safety Information throughout this deck. 48 48

49
Diagnostic Criteria for Chronic Migraine
Please see Important Safety Information, including Boxed Warning, on slides Please see Important Safety Information, including Boxed Warning, throughout this deck. Diagnostic Criteria for Chronic Migraine Chronic Migraine is a defined condition1-3 15 or more headache days per month Headaches lasting 4 hours per day or more At least 8 headache days classified as migraine days With or without medication overuse What are migraine characteristics1? 1 / Olesen 2006/ p744 2 / ICHD-2 - HCC; Olesen 2004, p24-25 3/ Lipton 2011/ p80 Patients should experience at least 2 of these pain characteristics: Unilateral Migrainous, pulsating quality Moderate to severe intensity Aggravated by routine physical activity And at least 1 of: Nausea and/or vomiting Photophobia and phonophobia 1 / Olesen 2006/p744 2 / ICHD-2 - HCC; Olesen 2004, p24-25 3/ Lipton 2011/ p80 The criteria used to classify Chronic Migraine, as stated by the International Classification of Headache Disorders, 2nd edition, revised, can be simplified to include1-3: Headache on 15 or more days of headache per month On average, headaches last 4 or more hours per day, and at least 8 headache days are classified as migraine days Headaches may or may not be associated with medication overuse Migraine symptoms include1: Having at least 2 of the following pain characteristics: Unilateral Migrainous pulsating quality Moderate to severe in intensity Aggravated by routine physical activity And at least 1 of the following: Nausea and/or vomiting Photophobia and phonophobia References: Headache Classification Subcommittee of the International Headache Society. International Classification of Headache Disorders, 2nd edition. Cephalalgia. 2004;24(Suppl 1):9-160. Headache Classification Committee; Olesen J et al. New appendix criteria open for a broader concept of chronic migraine. Cephalalgia. 2006;26: Lipton RB. Chronic migraine, classification, differential diagnosis, and epidemiology. Headache. 2011;51(Suppl 2):77-83. 49 Headache Classification Committee; Olesen J et al. Cephalalgia. 2004;24:9-160. Headache Classification Committee; Olesen J et al. Cephalalgia. 2006;26: Lipton RB. Headache. 2011;51(S2):77·83. 49
: Headache Classification Committee; Olesen J et al. New appendix criteria open for a broader concept of chronic migraine. Cephalalgia. 2006;26: Lipton RB. Chronic migraine, classification, differential diagnosis, and epidemiology. Headache. 2011;51(Suppl 2): Headache Classification Committee; Olesen J et al. Cephalalgia. 2004;24: Headache Classification Committee; Olesen J et al. Cephalalgia. 2006;26: Lipton RB. Headache. 2011;51(S2):77·")
50
Case Study: Emily Patient History:
Please see Important Safety Information, including Boxed Warning, on slides Please see Important Safety Information, including Boxed Warning, throughout this deck. Case Study: Emily Patient History: 43-year-old woman is seen for a main complaint of headache She has had headaches since her teens She reports 8 migraine attacks per month, each lasting 2–3 days She has migraine features (nausea, photophobia, and phonophobia) on all headache days She has tried multiple preventive medications Emily is a 43-year-old woman who is being seen for a main complaint of headache. She’s been suffering from headaches since she was a teenager. Currently, she is reporting 8 migraine attacks per month, each of which last 2 to 3 days at a time. On all headache days, she experiences nausea, photophobia, and phonophobia. In the past she has tried multiple types of preventive medications. 50 Case Studies do not involve actual patients 50
 on all headache days. She has tried multiple preventive medications. Emily is a 43-year-old woman who is being seen for a main complaint of headache. She’s been suffering from headaches since she was a teenager. Currently, she is reporting 8 migraine attacks per month, each of which last 2 to 3 days at a time. On all headache days, she experiences nausea, photophobia, and phonophobia. In the past she has tried multiple types of preventive medications. 50. Case Studies do not involve actual patients. 50.")
51
Study Design of Two Phase 3 Studies of Chronic Migraine Patients1,2
Please see Important Safety Information, including Boxed Warning, throughout this deck. Study Design of Two Phase 3 Studies of Chronic Migraine Patients1,2 Large clinical program of Chronic Migraine sufferers (1384 patients) 1/ Aurora p3 2 / Diener p3 Double-Blind Phase Open-Label Phase BOTOX® vs Placebo Primary Time Point All Patients on BOTOX® Baseline Randomization -4 Day 4 8 12 16 20 24 28 32 36 40 44 48 52 56 Weeks 1 2 3 4 5 PREEMPT (Phase 3 REsearch Evaluating Migraine Prophylaxis Therapy) was designed to mirror the Phase 2 headache study by Mathew,1 and was a multicenter, randomized, placebo-controlled, parallel-group, clinical study with an open-label extension phase conducted in 122 sites in North America and Europe.2,3 The studies consisted of: A 28-day baseline phase, A 24-week, double-blind treatment phase to evaluate efficacy and safety, and A 32-week, open-label extension phase to evaluate long-term safety. Study visits occurred every 4 weeks. Key inclusion criteria: During the 4-week baseline period, 15 or more headache days with each day consisting of at least 4 hours of continuous headache with 50% or more of baseline headache days being migraine/probable migraine days and at least 4 distinct headache episodes each lasting 4 or more hours.2-4 In the Phase 3 clinical trials, subjects were randomized 1:1 to BOTOX® or placebo, and randomization was additionally stratified based on the frequency of acute headache pain medication use during baseline (designated as “medication overuse–yes” or “medication overuse–no”), with treatments balanced in blocks of 4 within each medication overuse stratum for each investigator site.2,3 “Medication overuse–yes” was defined as intake of simple analgesics on at least 15 days, or other medication types or combination of types for at least 10 days, with intake at least 2 days/week from the category of overuse.2,3 Fixed-site, fixed-dose IM injections every 12 weeks over 56 weeks (5 cycles; 155 Units) in 7 specific head/neck muscle areas for a total of 31 sites with a total dose of 155 Units BOTOX® or placebo. References: 1. Mathew NT, Frishberg BM, Gawel M, et al. Botulinum toxin type A (BOTOX®) for the prophylactic treatment of chronic daily headache: a randomized, double-blind, placebo-controlled trial. Headache. 2005;45: 2. Aurora SK, Dodick DW, Turkel CC, et al. OnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 1 trial. Cephalalgia. 2010; 30: 3. Diener HC, Dodick DW, Aurora SK, et al. OnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 2 trial. Cephalalgia. 2010; 30: 4. Headache Classification Committee; Olesen J et al. New appendix criteria open for a broader concept of chronic migraine. Cephalalgia. 2006;26: 1/Mathew 2005, p293 BOTOX® vs Placebo (saline) BOTOX® vs Placebo (saline) BOTOX® BOTOX® BOTOX® Phone Interview Treatment 2/Aurora p2-3 3/Diener p2-3 4/ICHD-IIR 2006, p744/Table 1 Headache symptoms and medications were recorded in a daily telephone diary 51 Aurora SK et al. Cephalalgia. 2010;30: Diener HC et al. Cephalalgia. 2010;30: 51
 1/ Aurora 2010 p3. 2 / Diener 2010 p3. Double-Blind Phase. Open-Label Phase. BOTOX® vs Placebo. Primary Time Point. All Patients on BOTOX® Baseline. Randomization. -4. Day Weeks PREEMPT (Phase 3 REsearch Evaluating Migraine Prophylaxis Therapy) was designed to mirror the Phase 2 headache study by Mathew,1 and was a multicenter, randomized, placebo-controlled, parallel-group, clinical study with an open-label extension phase conducted in 122 sites in North America and Europe.2,3 The studies consisted of: A 28-day baseline phase, A 24-week, double-blind treatment phase to evaluate efficacy and safety, and. A 32-week, open-label extension phase to evaluate long-term safety. Study visits occurred every 4 weeks. Key inclusion criteria: During the 4-week baseline period, 15 or more headache days with each day consisting of at least 4 hours of continuous headache with 50% or more of baseline headache days being migraine/probable migraine days and at least 4 distinct headache episodes each lasting 4 or more hours.2-4. In the Phase 3 clinical trials, subjects were randomized 1:1 to BOTOX® or placebo, and randomization was additionally stratified based on the frequency of acute headache pain medication use during baseline (designated as medication overuse–yes or medication overuse–no ), with treatments balanced in blocks of 4 within each medication overuse stratum for each investigator site.2,3. Medication overuse–yes was defined as intake of simple analgesics on at least 15 days, or other medication types or combination of types for at least 10 days, with intake at least 2 days/week from the category of overuse.2,3. Fixed-site, fixed-dose IM injections every 12 weeks over 56 weeks (5 cycles; 155 Units) in 7 specific head/neck muscle areas for a total of 31 sites with a total dose of 155 Units BOTOX® or placebo. References: 1. Mathew NT, Frishberg BM, Gawel M, et al. Botulinum toxin type A (BOTOX®) for the prophylactic treatment of chronic daily headache: a randomized, double-blind, placebo-controlled trial. Headache. 2005;45: Aurora SK, Dodick DW, Turkel CC, et al. OnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 1 trial. Cephalalgia. 2010; 30: Diener HC, Dodick DW, Aurora SK, et al. OnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 2 trial. Cephalalgia. 2010; 30: Headache Classification Committee; Olesen J et al. New appendix criteria open for a broader concept of chronic migraine. Cephalalgia. 2006;26: /Mathew 2005, p293. BOTOX® vs Placebo (saline) BOTOX® vs Placebo (saline) BOTOX® BOTOX® BOTOX® Phone Interview. Treatment. 2/Aurora 2010 p2-3. 3/Diener 2010 p2-3. 4/ICHD-IIR 2006, p744/Table 1. Headache symptoms and medications were recorded in a daily telephone diary. 51. Aurora SK et al. Cephalalgia. 2010;30: Diener HC et al. Cephalalgia. 2010;30:")
52
Efficacy of BOTOX® at Week 24 for Study 1 and Study 2
Please see Important Safety Information, including Boxed Warning, throughout this deck. Efficacy of BOTOX® at Week 24 for Study 1 and Study 2 Efficacy per 28 days Study 1 Study 2 BOTOX® (n=341) Placebo (n=338) BOTOX® (n=347) Placebo (n=358) Change from baseline in frequency of headache days -7.8* -6.4 -9.2* -6.9 Change from baseline in total cumulative hours of headache on headache days -107* -70 -134* -95 1/ Botox Chronic Migraine PI, Table 13 1/ Botox Chronic Migraine PI, Table 13 There were significant differences favoring BOTOX® treatment at Week 24 in these efficacy variables evaluated in both Study 1 and Study 2.1 In clinical studies, patients treated with BOTOX® experienced up to 9 fewer headache days per month at 24 weeks, compared to up to 7 fewer days in the group of patients receiving placebo injections (a treatment containing no medicine). Patients treated with BOTOX® also saw a reduction of up to 134 total cumulative hours of headache on headache days per month, compared to a reduction of up to 95 hours for those receiving placebo at 24 weeks.1 Reference: 1. BOTOX® (onabotulinumtoxinA) Prescribing Information. Irvine, CA: Allergan, Inc., 2011. *Significantly different from placebo (p≤0.05) 52 BOTOX® (onabotulinumtoxinA) Prescribing Information. Allergan, Inc., 2011. 52
 Placebo (n=338) BOTOX® (n=347) Placebo (n=358) Change from baseline in frequency of headache days. -7.8* * Change from baseline in total cumulative hours of headache on headache days. -107* * / Botox Chronic Migraine PI, Table 13. 1/ Botox Chronic Migraine PI, Table 13. There were significant differences favoring BOTOX® treatment at Week 24 in these efficacy variables evaluated in both Study 1 and Study 2.1. In clinical studies, patients treated with BOTOX® experienced up to 9 fewer headache days per month at 24 weeks, compared to up to 7 fewer days in the group of patients receiving placebo injections (a treatment containing no medicine). Patients treated with BOTOX® also saw a reduction of up to 134 total cumulative hours of headache on headache days per month, compared to a reduction of up to 95 hours for those receiving placebo at 24 weeks.1. Reference: 1. BOTOX® (onabotulinumtoxinA) Prescribing Information. Irvine, CA: Allergan, Inc., *Significantly different from placebo (p≤0.05) 52. BOTOX® (onabotulinumtoxinA) Prescribing Information. Allergan, Inc.,")
53
Please see Important Safety Information, including Boxed Warning, throughout this deck.
Adverse Reactions Reported by 2% of Patients Treated With BOTOX (More Frequent Than Placebo) in Two Chronic Migraine Double-Blind, Placebo-Controlled Clinical Trials1 Adverse Reactions by Body Systems BOTOX® (n=687) 155 Units-195 Units Placebo (n=692) Nervous system disorders Headache Migraine Facial paresis 32 (5%) 26 (4%) 15 (2%) 22 (3%) 18 (3%) 0 (0%) Eye disorders Eyelid ptosis 25 (4%) 2 (<1%) Infections and infestations Bronchitis 17 (3%) 11 (2%) Musculoskeletal and connective tissue disorders Neck pain Musculoskeletal stiffness Muscular weakness* Myalgia Musculoskeletal pain Muscle spasms 60 (9%) 24 (4%) 21 (3%) 13 (2%) 19 (3%) 6 (1%) 10 (1%) General disorders and administration site conditions Injection site pain 23 (3%) 14 (2%) Vascular disorders Hypertension 7 (1%) Botox Chronic Migraine PI, Table 9 Aurora 2011, p9, p11 Table 4 This slide shows adverse reactions reported with an incidence of 2% or more. The adverse reactions reported in the BOTOX® group with an incidence of 5% or more were headache (5%) and neck pain (9%), versus 3% for both of these reactions in the placebo group.1 Other adverse reactions that occurred more frequently in the BOTOX® group compared to the placebo group at a frequency less than 1% and potentially related to BOTOX® include: vertigo, dry eye, eyelid edema, dysphagia, eye infection, and jaw pain. Severe worsening of migraine requiring hospitalization occurred in approximately 1% of patients treated with BOTOX® in Study 1 and Study 2, usually within the first week after treatment, compared to 0.3% of placebo-treated patients.1 Reference: 1. BOTOX® (onabotulinumtoxinA) Prescribing Information. Irvine, CA: Allergan, Inc., 2011. 1/Botox Chronic Migraine PI, Table 9, p13 Severe worsening of migraine requiring hospitalization occurred in approximately 1% of patients treated with BOTOX® in Study 1 and Study 2, usually within the first week after treatment, compared to 0.3% of placebo-treated patients. 53 *Aurora et al 2011 reported n=38 (5.5%); 2.2% of the incidences of muscular weakness were facial paresis.2 1. BOTOX® (onabotulinumtoxinA) Prescribing Information. Allergan, Inc., Aurora SK et al. Headache. 2011;51: 53
 in Two Chronic Migraine Double-Blind, Placebo-Controlled Clinical Trials1. Adverse Reactions by Body Systems. BOTOX® (n=687) 155 Units-195 Units. Placebo (n=692) Nervous system disorders. Headache. Migraine. Facial paresis. 32 (5%) 26 (4%) 15 (2%) 22 (3%) 18 (3%) 0 (0%) Eye disorders. Eyelid ptosis. 25 (4%) 2 (<1%) Infections and infestations. Bronchitis. 17 (3%) 11 (2%) Musculoskeletal and connective tissue disorders. Neck pain. Musculoskeletal stiffness. Muscular weakness* Myalgia. Musculoskeletal pain. Muscle spasms. 60 (9%) 24 (4%) 21 (3%) 13 (2%) 19 (3%) 6 (1%) 10 (1%) General disorders and administration site conditions. Injection site pain. 23 (3%) 14 (2%) Vascular disorders. Hypertension. 7 (1%) Botox Chronic Migraine PI, Table 9. Aurora 2011, p9, p11 Table 4. This slide shows adverse reactions reported with an incidence of 2% or more. The adverse reactions reported in the BOTOX® group with an incidence of 5% or more were headache (5%) and neck pain (9%), versus 3% for both of these reactions in the placebo group.1. Other adverse reactions that occurred more frequently in the BOTOX® group compared to the placebo group at a frequency less than 1% and potentially related to BOTOX® include: vertigo, dry eye, eyelid edema, dysphagia, eye infection, and jaw pain. Severe worsening of migraine requiring hospitalization occurred in approximately 1% of patients treated with BOTOX® in Study 1 and Study 2, usually within the first week after treatment, compared to 0.3% of placebo-treated patients.1. Reference: 1. BOTOX® (onabotulinumtoxinA) Prescribing Information. Irvine, CA: Allergan, Inc., /Botox Chronic Migraine PI, Table 9, p13. Severe worsening of migraine requiring hospitalization occurred in approximately 1% of patients treated with BOTOX® in Study 1 and Study 2, usually within the first week after treatment, compared to 0.3% of placebo-treated patients. 53. *Aurora et al 2011 reported n=38 (5.5%); 2.2% of the incidences of muscular weakness were facial paresis BOTOX® (onabotulinumtoxinA) Prescribing Information. Allergan, Inc., Aurora SK et al. Headache. 2011;51:")
54
Discontinuation Rates
Please see Important Safety Information, including Boxed Warning, throughout this deck. Discontinuation Rates BOTOX® (n=687) Placebo (n=692) Discontinuation rate 12% 10% Discontinuations related to adverse events* 4% 1% 1/ Botox Chronic Migraine PI, p12 *The most frequent adverse events leading to discontinuation in the BOTOX® group were neck pain, headache, worsening migraine, muscular weakness, and eyelid ptosis. In double-blind, placebo-controlled Chronic Migraine pivotal efficacy trials (Study 1 and Study 2), the discontinuation rate was 12% in the group treated with BOTOX® and 10% in the placebo-treated group. The discontinuation rates due to adverse events were 4% in the BOTOX® group and 1% in the placebo group. The most common adverse events leading to discontinuation in the BOTOX® group were neck pain, headache, worsening migraine, muscular weakness, and eyelid ptosis.1 Please see Adverse Reactions table on slides 12 and 24. Reference: 1. BOTOX® (onabotulinumtoxinA) Prescribing Information. Irvine, CA: Allergan, Inc., 2011. 1/ Botox Chronic Migraine PI, p12 Please see Adverse Reactions table on slides 12 and 24. 54 BOTOX® (onabotulinumtoxinA) Prescribing Information. Allergan, Inc., 2011. 54
 Placebo (n=692) Discontinuation rate. 12% 10% Discontinuations related to adverse events* 4% 1% 1/ Botox Chronic Migraine PI, p12. *The most frequent adverse events leading to discontinuation in the BOTOX® group were neck pain, headache, worsening migraine, muscular weakness, and eyelid ptosis. In double-blind, placebo-controlled Chronic Migraine pivotal efficacy trials (Study 1 and Study 2), the discontinuation rate was 12% in the group treated with BOTOX® and 10% in the placebo-treated group. The discontinuation rates due to adverse events were 4% in the BOTOX® group and 1% in the placebo group. The most common adverse events leading to discontinuation in the BOTOX® group were neck pain, headache, worsening migraine, muscular weakness, and eyelid ptosis.1. Please see Adverse Reactions table on slides 12 and 24. Reference: 1. BOTOX® (onabotulinumtoxinA) Prescribing Information. Irvine, CA: Allergan, Inc., / Botox Chronic Migraine PI, p12. Please see Adverse Reactions table on slides 12 and BOTOX® (onabotulinumtoxinA) Prescribing Information. Allergan, Inc.,")
55
Please see Important Safety Information, including Boxed Warning, throughout this deck.
Injection Paradigm The phase 3 BOTOX® pivotal studies for Chronic Migraine patients has established a treatment paradigm1 The patient population, recommended dose, and injection paradigm were established based on 10 years of studies assessing various patient types, muscle groups, and doses2-6 155 Units of BOTOX® are administered as 31 fixed-site, fixed- dose injections across 7 specific head/neck muscle areas1 For each injection site, the injection volume will be 0.1 mL (5 Units)1 Each muscle has a fixed1: Total dose Number of injection sites Location of injection sites 1 / Blumenfeld pp 1407,1408 2 / Mathew 2005, p 303 3/ Silberstein 2005, p1135 4 / Silberstein 2000, 449 5/ Binder p675 6/ Freitag p7-8 In phase 3 studies, subjects in the double-blind phase were randomized in blinded fashion (1:1) to BOTOX® (155 Units) or placebo, administered as 31 fixed-site, fixed-dose, intramuscular (IM) injections across 7 specific head/neck muscle areas (frontalis, corrugator, procerus, temporalis, occipitalis, cervical paraspinal, and trapezius).1 Physicians were instructed to adhere to the injection paradigm as follows1: Each 100 Unit vial of onabotulinumtoxinA or placebo was diluted with 2 mL preservative-free normal saline, resulting in a concentration of 5 Units/0.1 mL. Doses of 155 Units or placebo were administered IM using a sterile 30-gauge, 0.5-inch needle as injections of 0.1 mL (5 Units) per site. Reference: Blumenfeld AM, Silberstein SD, Dodick DW, et al. Method of injection of onabotulinumtoxinA for chronic migraine: A safe, well-tolerated, and effective treatment paradigm based on the PREEMPT clinical program. Headache. 2010;50: 1/Blumenfeld Headache pp1408, 1410 1. Blumenfeld AM et al. Headache. 2010;50: Mathew NT et al. Headache. 2005;45: Silberstein SD et al. Mayo Clin Proc. 2005;80: Silberstein SD et al. Headache. 2000;40: Binder WJ et al. Otolaryngol Head Neck Surg. 2000;6: Freitag FG et al. Headache. 2008;48: 55 55
1. Each muscle has a fixed1: Total dose. Number of injection sites. Location of injection sites. 1 / Blumenfeld 2010 pp 1407, / Mathew 2005, p / Silberstein 2005, p / Silberstein 2000, / Binder 2000 p675. 6/ Freitag 2008 p7-8. In phase 3 studies, subjects in the double-blind phase were randomized in blinded fashion (1:1) to BOTOX® (155 Units) or placebo, administered as 31 fixed-site, fixed-dose, intramuscular (IM) injections across 7 specific head/neck muscle areas (frontalis, corrugator, procerus, temporalis, occipitalis, cervical paraspinal, and trapezius).1. Physicians were instructed to adhere to the injection paradigm as follows1: Each 100 Unit vial of onabotulinumtoxinA or placebo was diluted with 2 mL preservative-free normal saline, resulting in a concentration of 5 Units/0.1 mL. Doses of 155 Units or placebo were administered IM using a sterile 30-gauge, 0.5-inch needle as injections of 0.1 mL (5 Units) per site. Reference: Blumenfeld AM, Silberstein SD, Dodick DW, et al. Method of injection of onabotulinumtoxinA for chronic migraine: A safe, well-tolerated, and effective treatment paradigm based on the PREEMPT clinical program. Headache. 2010;50: /Blumenfeld 2010 Headache pp1408, Blumenfeld AM et al. Headache. 2010;50: Mathew NT et al. Headache. 2005;45: Silberstein SD et al. Mayo Clin Proc. 2005;80: Silberstein SD et al. Headache. 2000;40: Binder WJ et al. Otolaryngol Head Neck Surg. 2000;6: Freitag FG et al. Headache. 2008;48:")
56
Case Study: Emily’s Response to Treatment 2 Weeks Post-Injection
Please see Important Safety Information, including Boxed Warning, throughout this deck. Case Study: Emily’s Response to Treatment 2 Weeks Post-Injection Follow-up visit 2 weeks post-injection: Emily is still experiencing headaches due to Chronic Migraine She also now has neck pain She feels dissatisfied and hopeless and is not sure if she wants to continue with BOTOX® treatments At her follow-up visit 2 weeks post-injection, Emily says she is still experiencing headaches due to Chronic Migraine. She has also been having neck pain since her treatment. She feels dissatisfied and hopeless and is not sure she wants to continue BOTOX® injections. In PREEMPT 1 and 2, the first evaluation was 4 weeks post-injection. What are the next steps to take with Emily? Discuss realistic treatment expectations, including the results from the clinical trials. Review the adverse events associated with BOTOX® injections. In PREEMPT 1 and 2, the first evaluation was 4 weeks post-injection. Case Studies do not involve actual patients 56 56

57
Case Study: Monitoring Emily’s Response to Treatment
Please see Important Safety Information, including Boxed Warning, throughout this deck. Case Study: Monitoring Emily’s Response to Treatment Second Injection Cycle: Emily has returned for her second BOTOX® treatment Follow-up with the patient You continue to monitor and document Emily’s response to treatment Emily has returned for her second treatment cycle of BOTOX® injections. You continue to monitor her progress and document her response to treatment. 57 Case Studies do not involve actual patients 57

58
Injection Sites: Corrugator and Procerus
Please see Important Safety Information, including Boxed Warning, on slides Please see Important Safety Information, including Boxed Warning, throughout this deck. Injection Sites: Corrugator and Procerus 5 Units BOTOX® at each site (0.1 mL injected) BOTOX Chronic Migraine PI, section 2.4 Procerus: 5 Units in 1 site The corrugator muscle injection site is located approximately 1 finger’s breadth (~1.5 centimeters) above the medial superior edge of the orbital ridge (bony landmark).1 The procerus muscle injection site is midline on the forehead, approximately 1 finger’s breadth (~1.5 centimeters) above and midline to the medial superior aspect of the orbital ridge of each eye and is approximately midway between the two corrugator injections.1 Reference: 1. Blumenfeld AM, Silberstein SD, Dodick DW, et al. Method of injection of onabotulinumtoxinA for chronic migraine: A safe, well-tolerated, and effective treatment paradigm based on the PREEMPT clinical program. Headache. 2010;50: Blumenfeld, Headache p1413 Corrugator: 10 Units divided in 2 sites 58 BOTOX® (onabotulinumtoxinA) Prescribing Information. Allergan, Inc., 2011. 58
 BOTOX Chronic Migraine PI, section 2.4. Procerus: 5 Units in 1 site. The corrugator muscle injection site is located approximately 1 finger’s breadth (~1.5 centimeters) above the medial superior edge of the orbital ridge (bony landmark).1. The procerus muscle injection site is midline on the forehead, approximately 1 finger’s breadth (~1.5 centimeters) above and midline to the medial superior aspect of the orbital ridge of each eye and is approximately midway between the two corrugator injections.1. Reference: 1. Blumenfeld AM, Silberstein SD, Dodick DW, et al. Method of injection of onabotulinumtoxinA for chronic migraine: A safe, well-tolerated, and effective treatment paradigm based on the PREEMPT clinical program. Headache. 2010;50: Blumenfeld, 2010 Headache p1413. Corrugator: 10 Units divided in 2 sites. 58. BOTOX® (onabotulinumtoxinA) Prescribing Information. Allergan, Inc.,")
59
Injection Sites: Frontalis Region
Please see Important Safety Information, including Boxed Warning, on slides Please see Important Safety Information, including Boxed Warning, throughout this deck. Injection Sites: Frontalis Region 5 Units BOTOX® at each site (0.1 mL injected) BOTOX Chronic Migraine PI section 2.4 Frontalis: 20 Units divided in 4 sites The frontalis injection sites are located approximately 1.5 centimeters superior to the corrugator sites. 1 Reference: 1. Blumenfeld AM, Silberstein SD, Dodick DW, et al. Method of injection of onabotulinumtoxinA for chronic migraine: A safe, well-tolerated, and effective treatment paradigm based on the PREEMPT clinical program. Headache. 2010;50: Blumenfeld, Headache p1414 59 BOTOX® (onabotulinumtoxinA) Prescribing Information. Allergan, Inc., 2011. 59
 BOTOX Chronic Migraine PI section 2.4. Frontalis: 20 Units divided in 4 sites. The frontalis injection sites are located approximately 1.5 centimeters superior to the corrugator sites. 1. Reference: 1. Blumenfeld AM, Silberstein SD, Dodick DW, et al. Method of injection of onabotulinumtoxinA for chronic migraine: A safe, well-tolerated, and effective treatment paradigm based on the PREEMPT clinical program. Headache. 2010;50: Blumenfeld, 2010 Headache p BOTOX® (onabotulinumtoxinA) Prescribing Information. Allergan, Inc.,")
60
Injection Sites: Temporalis
Please see Important Safety Information, including Boxed Warning, throughout this deck. Injection Sites: Temporalis 5 Units BOTOX® at each site (0.1 mL injected) BOTOX Chronic Migraine PI section 2.4 Having the patient clench teeth will produce a palpable anterior bulge to the temporalis muscle, directing the anterior injection site Having the patient clench his or her teeth will facilitate in the location of the anterior aspect of the temporalis muscle. The four injection sites to be administered bilaterally in the temporalis muscle are shown.1 Reference: 1. Blumenfeld AM, Silberstein SD, Dodick DW, et al. Method of injection of onabotulinumtoxinA for chronic migraine: A safe, well-tolerated, and effective treatment paradigm based on the PREEMPT clinical program. Headache. 2010;50: Blumenfeld, Headache p1414 Temporalis: 40 Units divided in 8 sites 60 BOTOX® (onabotulinumtoxinA) Prescribing Information. Allergan, Inc., 2011. 60
 BOTOX Chronic Migraine PI section 2.4. Having the patient clench teeth will produce a palpable anterior bulge to the temporalis muscle, directing the anterior injection site. Having the patient clench his or her teeth will facilitate in the location of the anterior aspect of the temporalis muscle. The four injection sites to be administered bilaterally in the temporalis muscle are shown.1. Reference: 1. Blumenfeld AM, Silberstein SD, Dodick DW, et al. Method of injection of onabotulinumtoxinA for chronic migraine: A safe, well-tolerated, and effective treatment paradigm based on the PREEMPT clinical program. Headache. 2010;50: Blumenfeld, 2010 Headache p1414. Temporalis: 40 Units divided in 8 sites. 60. BOTOX® (onabotulinumtoxinA) Prescribing Information. Allergan, Inc.,")
61
Injection Sites: Occipitalis
Please see Important Safety Information, including Boxed Warning, on slides Please see Important Safety Information, including Boxed Warning, throughout this deck. Injection Sites: Occipitalis 5 Units BOTOX® at each site (0.1 mL injected) BOTOX Chronic Migraine PI section 2.4 Occipitalis: 30 Units divided in 6 sites This illustration shows the six injection sites for the occipitalis muscle.1 The occipitalis injections will be superior to the nuchal ridge on either side of the occipital protuberance.1 Reference: 1. Blumenfeld AM, Silberstein SD, Dodick DW, et al. Method of injection of onabotulinumtoxinA for chronic migraine: A safe, well-tolerated, and effective treatment paradigm based on the PREEMPT clinical program. Headache. 2010;50: Nuchal ridge Blumenfeld, Headache p1414 61 BOTOX® (onabotulinumtoxinA) Prescribing Information. Allergan, Inc., 2011. 61
 BOTOX Chronic Migraine PI section 2.4. Occipitalis: 30 Units divided in 6 sites. This illustration shows the six injection sites for the occipitalis muscle.1. The occipitalis injections will be superior to the nuchal ridge on either side of the occipital protuberance.1. Reference: 1. Blumenfeld AM, Silberstein SD, Dodick DW, et al. Method of injection of onabotulinumtoxinA for chronic migraine: A safe, well-tolerated, and effective treatment paradigm based on the PREEMPT clinical program. Headache. 2010;50: Nuchal ridge. Blumenfeld, 2010 Headache p BOTOX® (onabotulinumtoxinA) Prescribing Information. Allergan, Inc.,")
62
Injection Sites: Cervical Paraspinal Muscle Group and Trapezius
Please see Important Safety Information, including Boxed Warning, on slides Please see Important Safety Information, including Boxed Warning, throughout this deck. Injection Sites: Cervical Paraspinal Muscle Group and Trapezius 5 Units BOTOX® at each site (0.1 mL injected) BOTOX Chronic Migraine PI section 2.4 Cervical paraspinal muscle group: 20 Units divided in 4 sites Trapezius: 30 Units divided in 6 sites This slide illustrates the injection sites for the cervical paraspinal muscle group and trapezius muscles.1,2 Palpation of the cervical spine will aid in the location of the cervical paraspinal muscle group injection sites. The first injection is lateral to the midline approximately 3 to 5 centimeters inferior to the occipital protuberance, and the second injection on the same side 1 centimeter lateral and superior to the first injection.2 The trapezius is a triangular-shaped, superficial muscle that fans from the neck into the shoulder. The injection sites are located in superior portion of this muscle.2 It is important to note that an anatomical overlap exists with respect to the upper portion of the trapezius, rectus capitis, semispinalis capitis, and splenius capitis.3 References: BOTOX® (onabotulinumtoxinA) Prescribing Information. Irvine, CA: Allergan, Inc., 2011. Blumenfeld AM, Silberstein SD, Dodick DW, et al. Method of injection of onabotulinumtoxinA for chronic migraine: A safe, well-tolerated, and effective treatment paradigm based on the PREEMPT clinical program. Headache. 2010;50: Binder W, Blitzer A. Treatment of migraine headache with botulinum toxin type A. Facial Plast Sur Clin N Am. 2003;11: 1/BOTOX Chronic Migraine PI section 2.4 2/Blumenfeld Headache p1415 3/Binder p471 / Fig 5A 62 BOTOX® (onabotulinumtoxinA) Prescribing Information. Allergan, Inc., 2011. 62
 BOTOX Chronic Migraine PI section 2.4. Cervical paraspinal muscle group: 20 Units divided in 4 sites. Trapezius: 30 Units divided in 6 sites. This slide illustrates the injection sites for the cervical paraspinal muscle group and trapezius muscles.1,2 Palpation of the cervical spine will aid in the location of the cervical paraspinal muscle group injection sites. The first injection is lateral to the midline approximately 3 to 5 centimeters inferior to the occipital protuberance, and the second injection on the same side 1 centimeter lateral and superior to the first injection.2. The trapezius is a triangular-shaped, superficial muscle that fans from the neck into the shoulder. The injection sites are located in superior portion of this muscle.2. It is important to note that an anatomical overlap exists with respect to the upper portion of the trapezius, rectus capitis, semispinalis capitis, and splenius capitis.3. References: BOTOX® (onabotulinumtoxinA) Prescribing Information. Irvine, CA: Allergan, Inc., Blumenfeld AM, Silberstein SD, Dodick DW, et al. Method of injection of onabotulinumtoxinA for chronic migraine: A safe, well-tolerated, and effective treatment paradigm based on the PREEMPT clinical program. Headache. 2010;50: Binder W, Blitzer A. Treatment of migraine headache with botulinum toxin type A. Facial Plast Sur Clin N Am. 2003;11: /BOTOX Chronic Migraine PI section /Blumenfeld Headache p /Binder p471 / Fig 5A. 62. BOTOX® (onabotulinumtoxinA) Prescribing Information. Allergan, Inc.,")
63
BOTOX®: The Real Facts Summary Questions
63

Similar presentations







 patients Policy.>")













