Download presentation
Presentation is loading. Please wait.

2
Lipid Management Standard and Advanced Preview of ATP-IV
Thomas G. Allison, PhD, MPH Mayo Clinic Rochester, MN USA

3
Relevant Financial Relationship(s)
DISCLOSURE Relevant Financial Relationship(s) None Off Label Usage
 None. Off Label Usage.")
4
Treatment Categories, LDL-C Goals and Cut-points: ATP-III
Risk Category LDL-C Goal Consider Drug Therapy CHD or CHD risk equivalent <100 mg/dL 130 mg/dL* 2 Risk Factors 10-yr risk 10–20% 10-yr risk <10% <130 mg/dL 130 mg/dL 160 mg/dL <2 Risk Factors <160 mg/dL 190 mg/dL Treatment categories, LDL-C goals and cutpoints The primary goal of clinical lipid management is reduction of low-density lipoprotein cholesterol (LDL-C) to lower coronary heart disease (CHD) risk. Individuals who do not or cannot achieve this goal with therapeutic lifestyle change (TLC) alone are candidates for drug therapy. TLC is an important component of any lipid-lowering program. It can obviate the need for drug therapy, augment the LDL-C lowering achieved with drug therapy, and provide benefits beyond LDL-C lowering which contribute substantially to CHD risk reduction. As with all considerations in the Adult Treatment Panel III (ATP III) recommendations, the decision to initiate drug therapy should be consistent with the patient’s CHD risk. Those with the highest risk should be offered the most aggressive treatment to reduce the risk optimally. Conversely, in patients with the lowest risk, drug therapy may not be cost-effective. Patients with CHD or a CHD risk equivalent have the highest risk, exceeding 20% in 10 years, and are candidates for lipid-modifying drug therapy. Those with levels above 130 mg/dL can be given drugs simultaneously with TLC as lifestyle change alone is unlikely to achieve the treatment goal. Those with levels between 100 and 129 mg/dL should first be treated with TLC, and after an appropriate trial (e.g., 3 months), lipid-lowering drug therapy (for example, a statin or fibrate) may be initiated. Some clinicians prefer to initiate drug therapy simultaneously with TLC in patients being discharged from the hospital following a CHD event or with a CHD risk equivalent. In this case, the therapy can be adjusted on a subsequent visit if the treatment goal is not achieved or if it is exceeded. For CHD or CHD risk equivalent patients who were given LDL-C–lowering drug therapy and have an on-treatment LDL-C of 100–129 mg/dL, clinical judgment should be applied to choose from a number of options. The majority of participants in the statin endpoint trials had on-treatment LDL-C values in this range. Choices include intensifying TLC, adjusting the dose of the LDL-C–lowering drug, initiating nondrug treatment of the metabolic syndrome if it is present, or intensifying treatment of nonlipid risk factors. Patients with 2 or more major risk factors and a 10-year risk between 10 and 20% have an LDL-C goal of <130 mg/dL and should be given TLC; if it is unlikely that this alone will achieve the treatment goal, drug therapy may be initiated simultaneously. In most cases, TLC is tried for about 3 months before making decisions to advance to drug therapy. After adequate LDL-C reduction has been achieved, other risk factors, including obesity and sedentary lifestyle, should be addressed. Patients with 2 or more risk factors and a 10-year risk of <10% as well as patients with <2 risk factors (who mostly have a 10-year risk of <10%) should be treated with TLC unless LDL-C levels are very high, because drug therapy in these patients is the least cost-effective. If treatment goal cannot be achieved with TLC alone, consideration can be given to using lipid-lowering drug therapy. Reference: Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285: * 100–129 mg/dL = after TLC, consider statin, niacin, or fibrate therapy Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA 2001;285:
 to lower coronary heart disease (CHD) risk. Individuals who do not or cannot achieve this goal with therapeutic lifestyle change (TLC) alone are candidates for drug therapy. TLC is an important component of any lipid-lowering program. It can obviate the need for drug therapy, augment the LDL-C lowering achieved with drug therapy, and provide benefits beyond LDL-C lowering which contribute substantially to CHD risk reduction. As with all considerations in the Adult Treatment Panel III (ATP III) recommendations, the decision to initiate drug therapy should be consistent with the patient’s CHD risk. Those with the highest risk should be offered the most aggressive treatment to reduce the risk optimally. Conversely, in patients with the lowest risk, drug therapy may not be cost-effective. Patients with CHD or a CHD risk equivalent have the highest risk, exceeding 20% in 10 years, and are candidates for lipid-modifying drug therapy. Those with levels above 130 mg/dL can be given drugs simultaneously with TLC as lifestyle change alone is unlikely to achieve the treatment goal. Those with levels between 100 and 129 mg/dL should first be treated with TLC, and after an appropriate trial (e.g., 3 months), lipid-lowering drug therapy (for example, a statin or fibrate) may be initiated. Some clinicians prefer to initiate drug therapy simultaneously with TLC in patients being discharged from the hospital following a CHD event or with a CHD risk equivalent. In this case, the therapy can be adjusted on a subsequent visit if the treatment goal is not achieved or if it is exceeded. For CHD or CHD risk equivalent patients who were given LDL-C–lowering drug therapy and have an on-treatment LDL-C of 100–129 mg/dL, clinical judgment should be applied to choose from a number of options. The majority of participants in the statin endpoint trials had on-treatment LDL-C values in this range. Choices include intensifying TLC, adjusting the dose of the LDL-C–lowering drug, initiating nondrug treatment of the metabolic syndrome if it is present, or intensifying treatment of nonlipid risk factors. Patients with 2 or more major risk factors and a 10-year risk between 10 and 20% have an LDL-C goal of <130 mg/dL and should be given TLC; if it is unlikely that this alone will achieve the treatment goal, drug therapy may be initiated simultaneously. In most cases, TLC is tried for about 3 months before making decisions to advance to drug therapy. After adequate LDL-C reduction has been achieved, other risk factors, including obesity and sedentary lifestyle, should be addressed. Patients with 2 or more risk factors and a 10-year risk of <10% as well as patients with <2 risk factors (who mostly have a 10-year risk of <10%) should be treated with TLC unless LDL-C levels are very high, because drug therapy in these patients is the least cost-effective. If treatment goal cannot be achieved with TLC alone, consideration can be given to using lipid-lowering drug therapy. Reference: Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285: * 100–129 mg/dL = after TLC, consider statin, niacin, or fibrate therapy. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA 2001;285:")
5
Major ATP III Risk Factors
Age Male ≥ 45 years Female ≥ 55 years Family History Male first degree relative < 55 years Female first degree relative < 65 years HDL-C < 40 mg/dL Hypertension Current Smoking

6
CAD Equivalents Coronary Artery Disease (CAD) Diabetes Mellitus
Abdominal Aortic Aneurysm Carotid Artery Disease (>50% stenosis) Prior CVA or TIA Peripheral Arterial Disease Framingham Score >20% 10 yr Risk
 Prior CVA or TIA. Peripheral Arterial Disease. Framingham Score >20% 10 yr Risk.")
7
CAD Risk Equivalents? Chronic Renal Insufficiency
Abnormal Coronary Calcium Scores Agatston score > 400

8
Goals for Therapy: 2004 Addendum
NCEP ATP III guidelines for LDL Therapy LDL-C <160 for 1 or less risk factors LDL-C <130 for 2+ risk factors < 100 is a therapeutic option LDL-C <100 for CAD and CAD equivalents <70 is option for very high risk patients CAD + multiple risk factors, especially diabetes CAD + severe or poorly controlled risk factor(s) CAD + metabolic syndrome Acute coronary syndrome CAD event despite baseline LDL-C < 100
 CAD + metabolic syndrome. Acute coronary syndrome. CAD event despite baseline LDL-C < 100.")
9
LDL-C Therapy Lifestyle Change Statins Bile Acid Sequestrants
Ezetimibe Niacin Plant Stanols, Sterols, Phytosterols

10
Residual Risk: Non-HDL-C
ATP III: Non-HDL-C is a secondary target of drug therapy when TG ≥ 200mg/dL Represents all the triglyceride-rich lipoproteins – considered atherogenic Non-HDL-C = Total Cholesterol – HDL-C Valid even if patient is non-fasting Cost-Effective

11
Targets for Therapy after LDL-C Goal in Patients with TG 200 mg/dL
Patient Category LDL-C target (mg/dL) Non-HDL-C target (mg/dL) CHD or CHD risk equivalent <100 <130 No CHD, 2+ RF <160 No CHD, <2 RF <190 Targets for therapy after LDL-C goal in patients with TG 200 mg/dL Epidemiologic and clinical studies have demonstrated that high blood triglyceride level is an independent risk factor for CHD and that CHD risk is amplified in patients who have elevations in both LDL-C and triglyceride levels. An elevated triglyceride level probably does not contribute to atherogenesis per se but most likely signals the presence of a constellation of lipid abnormalities that increase atherogenic risk, including increased levels of cholesterol-carrying remnant particles, low HDL-C levels, increased numbers of particles, and increased levels of small dense LDL. Patients with these abnormalities often have multiple other CHD risk factors, including central obesity, impaired glucose tolerance, and hypertension. To address these issues and to enhance the potential for CHD risk reduction, ATP III recommends that secondary treatment targets, defined by non-HDL-C (total cholesterol – HDL-C), be established for those who have a triglyceride level 200 mg/dL, after the LDL-C goal has been achieved. Non-HDL-C goals may be achieved by intensifying lifestyle modification, accentuating LDL-C–lowering therapy, or adding a triglyceride-lowering drug to the LDL-C–lowering regimen. Time and additional clinical trials will establish the utility of these various approaches. Reference: Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285: Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA 2001;285:
 Non-HDL-C target (mg/dL) CHD or CHD risk equivalent. <100. <130. No CHD, 2+ RF. <160. No CHD, <2 RF. <190. Targets for therapy after LDL-C goal in patients with TG 200 mg/dL. Epidemiologic and clinical studies have demonstrated that high blood triglyceride level is an independent risk factor for CHD and that CHD risk is amplified in patients who have elevations in both LDL-C and triglyceride levels. An elevated triglyceride level probably does not contribute to atherogenesis per se but most likely signals the presence of a constellation of lipid abnormalities that increase atherogenic risk, including increased levels of cholesterol-carrying remnant particles, low HDL-C levels, increased numbers of particles, and increased levels of small dense LDL. Patients with these abnormalities often have multiple other CHD risk factors, including central obesity, impaired glucose tolerance, and hypertension. To address these issues and to enhance the potential for CHD risk reduction, ATP III recommends that secondary treatment targets, defined by non-HDL-C (total cholesterol – HDL-C), be established for those who have a triglyceride level 200 mg/dL, after the LDL-C goal has been achieved. Non-HDL-C goals may be achieved by intensifying lifestyle modification, accentuating LDL-C–lowering therapy, or adding a triglyceride-lowering drug to the LDL-C–lowering regimen. Time and additional clinical trials will establish the utility of these various approaches. Reference: Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285: Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA 2001;285:")
12
Potential Goal Modifying Factors
Lp(a) High sensitivity CRP Metabolic Syndrome
 High sensitivity CRP. Metabolic Syndrome.")
13
Definition of the Metabolic Syndrome
Defined by presence of >3 risk factors Risk Factor Defining Level Waist circumference (abdominal obesity) >40 in (>102 cm) in men >35 in (>88 cm) in women Triglyceride level >150 mg/dl HDL-C level <40 mg/dl in men <50 mg/dl in women Blood pressure >130/>85 mmHg Fasting glucose >100 mg/dl I Grundy, et al. Diagnosis and management of the metabolic syndrome: an AHA/NHLBI Scientific Statement. Circulation 2005;112:
 >40 in (>102 cm) in men. >35 in (>88 cm) in women. Triglyceride level. >150 mg/dl. HDL-C level. <40 mg/dl in men. <50 mg/dl in women. Blood pressure. >130/>85 mmHg. Fasting glucose. >100 mg/dl. I. Grundy, et al. Diagnosis and management of the metabolic syndrome: an AHA/NHLBI Scientific Statement. Circulation 2005;112:")
14
Dr. Allison Attempts to Call Forth the Contents of ATP-IV

15
Will ATP-IV Signal a New Wave of Lipid Management?

16
Sweeping Changes?

17
Detection, Evaluation, and Treatment
of High Blood Cholesterol in Adults (Adult Treatment Panel IV) Expert Panel Membership Co-Chairs Alice H. Lichtenstein, D.Sc. Tufts University Boston, Massachusetts Neil Stone, M.D. Northwestern University School of Medicine Chicago, Illinois
 Expert Panel Membership. Co-Chairs. Alice H. Lichtenstein, D.Sc. Tufts University Boston, Massachusetts Neil Stone, M.D. Northwestern University School of Medicine Chicago, Illinois.")
18
Daniel Rader, M. D. University of Pennsylvania Jennifer Robinson, M
Daniel Rader, M.D. University of Pennsylvania Jennifer Robinson, M.D, M.P.H. University of Iowa Frank M. Sacks, M.D. Harvard University School of Public Health J. Sanford Schwartz, M.D. University of Pennsylvania Sidney C. Smith, Jr. M.D. University of North Carolina Karol Watson, M.D., Ph.D. University of California at Los Angeles Peter W. F. Wilson, M.D. Emory University School of Medicine C. Noel Bairey Merz, M.D. University of California, Los Angeles Conrad Blum, M.D. Columbia University Robert H. Eckel, M.D. University of Colorado, Denver Anne Carol Goldberg, M.D., FACP, FAHA Washington University Ronald M. Krauss, M.D. Children's Hospital Oakland Research Institute Donald M. Lloyd-Jones, M.D., Sc.M. Northwestern University Patrick McBride, M.D., M.P.H. University of Wisconsin

19
Status Expected Availability for Public Review
and Comment: Spring 2011 Expected Release Date: Fall 2011

20
Issues for ATP-IV Should the goals for LDL-C in primary prevention be lowered? What to do with CRP – routine use in risk stratification, secondary target? What about secondary target? Non-HDL-C, HDL-C, apo B, LDL Particle concentration? Move from 10-year to lifetime risk?

21
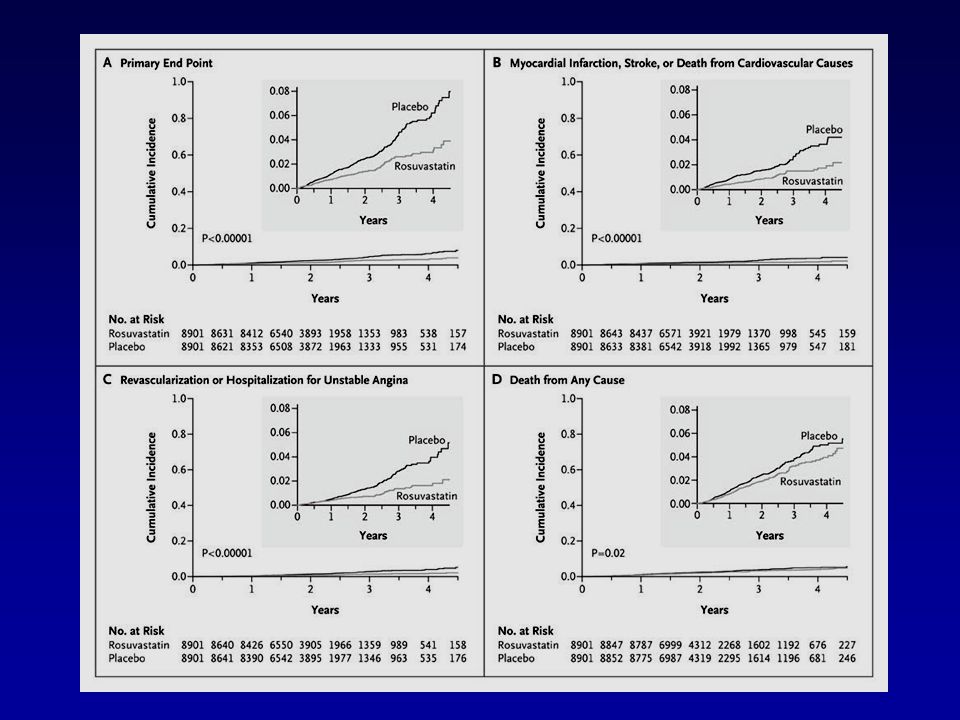
Jupiter Trial To test the hypothesis that statin treatment will reduce CV events in patients without baseline CVD with “normal” LDL-C (< 130 mg/dL) and elevated hsCRP (≥ 2.0 mg/L) The most innovative and potentially important lipid-lowering trial since the 2004 ATP-II Addendum Ridker PM et al. NEJM 2008;359:
 and elevated hsCRP (≥ 2.0 mg/L) The most innovative and potentially important lipid-lowering trial since the 2004 ATP-II Addendum. Ridker PM et al. NEJM 2008;359:")
22
Jupiter Methods 17,802 subjects (38% women)
Men ≥ 50 years; women ≥ 60 years Triglycerides < 500 mg/dL Randomized to Rosuvastatin 20 mg/day or placebo Planned 60 month follow-up Primary outcome was major CV event Including elective revascularization

23
Jupiter Results Study terminated early on with median follow-up of 1.9 years Compliance at study termination was 75% 44% reduction in primary endpoint 0.77% versus 1.36% per year 20% reduction in total mortality 1.00% versus 1.25% per year

24
12-Month Laboratory Results (Medians)
Rosuvastatin Placebo hs-CRP 2.2 3.5 LDL-C 55 110 HDL-C 52 50 TG 99 119

27
JUPITER Questions Would a lower-cost, generic statin show similar benefit? Is measurement of hsCRP necessary for risk stratification in primary prevention Ridker conflict of interest issues Was the benefit due to LDL-C lowering or hsCRP lowering?

28
Risk Factors in Jupiter Subjects
Average age = 66 years Current smokers = 16% Metabolic syndrome = 41% Family history of premature CAD = 11% 25% had fasting glucose > 102 mg/dL 25% had systolic BP > 145 mmHg

29
PROVE IT - TIMI 22: Study Design
4,162 patients with an Acute Coronary Syndrome < 10 days ASA + Standard Medical Therapy Double-blind “Standard Therapy” Pravastatin 40 mg “Intensive Therapy” Atorvastatin 80 mg PROVE IT is a double-blind, randomized trial that has enrolled 4,160 patients, at approximately 400 sites in the US, Europe, Canada, and Australia, who have experienced an acute coronary syndrome (Q wave and non-Q-wave MI or unstable angina) within the previous 10 days. Patients received either 40 mg of pravastatin or 80 mg of atorvastatin within 10 days of their event and were followed for a mean follow-up period of 2 years. To study the role of infection in ACS, one half of the patients in the trial also received gatifloxacin 400 mg in addition to either pravastatin or atorvastatin. Gatifloxacin was started on day 15 after the initial episode of ACS for a treatment period of 14 days. Gatifloxacin was subsequently given as a pulsed dose of 400mg per day for 10 days each month for a mean of 2 years. The other half of the patient population received an antibiotic placebo. 2x2 Factorial: Gatifloxacin vs. placebo Duration: Mean 2 year follow-up (>925 events) Primary Endpoint: Death, MI, Documented UA requiring hospitalization, revascularization (> 30 days after randomization), or Stroke
 within the previous 10 days. Patients received either 40 mg of pravastatin or 80 mg of atorvastatin within 10 days of their event and were followed for a mean follow-up period of 2 years. To study the role of infection in ACS, one half of the patients in the trial also received gatifloxacin 400 mg in addition to either pravastatin or atorvastatin. Gatifloxacin was started on day 15 after the initial episode of ACS for a treatment period of 14 days. Gatifloxacin was subsequently given as a pulsed dose of 400mg per day for 10 days each month for a mean of 2 years. The other half of the patient population received an antibiotic placebo. 2x2 Factorial: Gatifloxacin vs. placebo. Duration: Mean 2 year follow-up (>925 events) Primary Endpoint: Death, MI, Documented UA requiring hospitalization, revascularization (> 30 days after randomization), or Stroke.")
30
Changes from (Post-ACS) Baseline in Median LDL-C
(mg/dL) Median LDL-C (Q1, Q3) 95 (79, 113) 62 (50, 79) 120 100 Pravastatin 40mg 21% 80 60 Atorvastatin 80mg 49% 40 P<0.001 20 <24h Rand. 30 Days 4 Mos. 8 Mos. 16 Mos. Final Note: Changes in LDL-C may differ from prior trials: 25% of patients on statins prior to ACS event ACS response lowers LDL-C from true baseline
 Median LDL-C (Q1, Q3) 95 (79, 113) 62 (50, 79) Pravastatin 40mg. 21% Atorvastatin 80mg. 49% 40. P< <24h. Rand. 30 Days. 4 Mos. 8 Mos. 16 Mos. Final. Note: Changes in LDL-C may differ from prior trials: 25% of patients on statins prior to ACS event. ACS response lowers LDL-C from true baseline.")
31
PROVE IT: Concomitant Therapies
PCI for initial ACS pre-random % Aspirin % Warfarin % Clopidogrel (initial) % (at F/U) % B-blockers % ACE % ARB %
 72% (at F/U) 20% B-blockers 85% ACE 69% ARB 14%")
32
All-Cause Death or Major CV Events in All Randomized Subjects
30 Pravastatin 40mg (26.3%) 25 20 % with Event Atorvastatin 80mg (22.4%) 15 16% relative risk reduction (p = 0.005) 10 5 But absolute residual risk is 22% 3 18 21 24 27 30 6 9 12 15 Months of Follow-up
 % with Event. Atorvastatin 80mg. (22.4%) % relative risk reduction. (p = 0.005) But absolute residual risk is 22% Months of Follow-up.")
33
Sources of Residual Risk
Not providing appropriate medical therapy? Inadequate control of non-lipid risk factors? Not addressing emerging risk factors? CRP, Lp(a) Inadequate control of lipids using LDL target only? Non-HDL HDL or apo A-1 Apo B LDL particle number LDL particle size
 Inadequate control of lipids using LDL target only Non-HDL. HDL or apo A-1. Apo B. LDL particle number. LDL particle size.")
34
Secondary Lipid Target
In ATP-III, non-HDL-C was identified as the secondary lipid target Sum of cholesterol in all atherogenic lipoproteins LDL-C, Lp(a)-C, VLDL-C, IDL-C No major trial since publication of ATP-III in 2001 that specifically treated non-HDL-C
-C, VLDL-C, IDL-C. No major trial since publication of ATP-III in 2001 that specifically treated non-HDL-C.")
35
Lowering non-HDL-C Increase the statin dose Add fibrate Add niacin
High dose fish oil Exercise, CHO restriction, weight loss

36
FIELD Study Fenofibrate to Prevent Cardiovascular Events in Diabetics
FIELD Study Investigators Lancet 2005; 366:

37
FIELD Mortality No significant benefit shown in ACCORD-Lipids
for fenofibrate added to Simvastatin 40 mg/day. NEJM 2010, March 14.

38
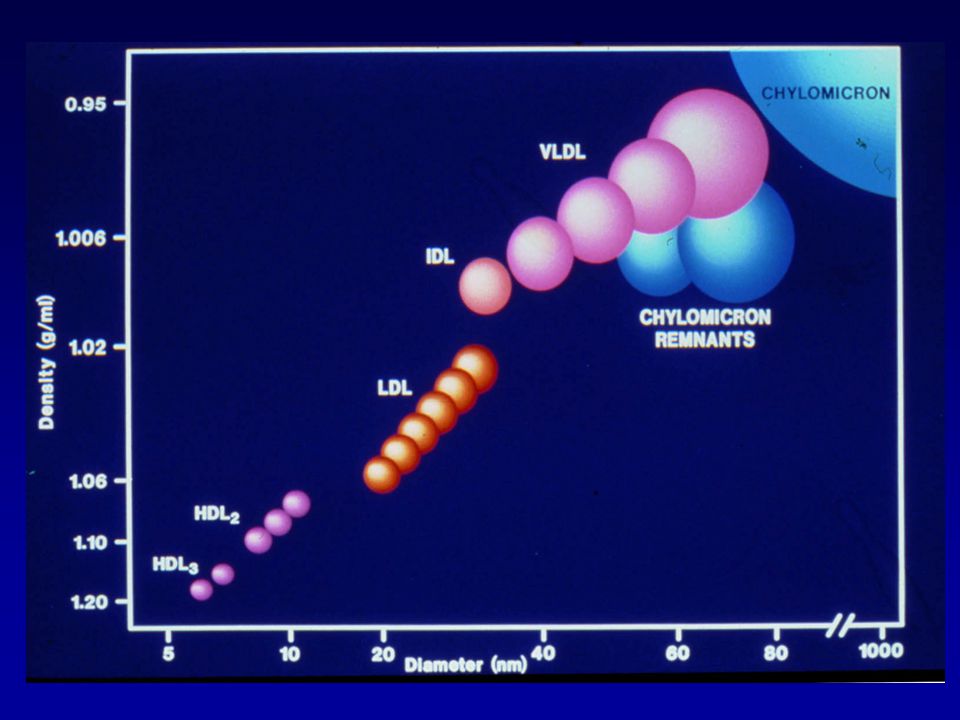
LDL Particles Cause Atherosclerosis
Low Density Lipoprotein particles (LDL) are the causal agents in atherosclerosis.1 The more LDL particles a person has, the higher the risk for plaque buildup that causes heart attacks, regardless of how much cholesterol those particles carry. Atherosclerosis comes from the Greek words athero (meaning gruel or paste) and sclerosis (hardness). It involves deposits of fatty substances, cholesterol, cellular waste products, calcium and other substances in the inner lining of an artery. This buildup is called plaque. The hard truth about cholesterol is, unless there is a lipoprotein particle carrying cholesterol – it can’t make it through the space to cause atherosclerosis. The cholesterol in the green oval will get metabolized by the liver. The cholesterol in the red ovals can kill you. The higher the number of particles, the more cholesterol will be transported through the endothelial gap. 1 Fredrickson et al. NEJM 1967; 276: 148
 are the causal. agents in atherosclerosis.1. The more LDL particles a person has, the higher the risk for plaque buildup that causes heart attacks, regardless of how much cholesterol those particles carry. Atherosclerosis comes from the Greek words athero (meaning gruel or paste) and sclerosis (hardness). It involves deposits of fatty substances, cholesterol, cellular waste products, calcium and other substances in the inner lining of an artery. This buildup is called plaque. The hard truth about cholesterol is, unless there is a lipoprotein particle carrying cholesterol – it can’t make it through the space to cause atherosclerosis. The cholesterol in the green oval will get metabolized by the liver. The cholesterol in the red ovals can kill you. The higher the number of particles, the more cholesterol will be transported through the endothelial gap. 1 Fredrickson et al. NEJM 1967; 276: 148.")
40
LDL-C is not LDL This is LDL This is LDL Cholesterol POLAR Apo B
SURFACE COAT Phospholipid Free cholesterol This is LDL NONPOLAR LIPID CORE Cholesterol Ester Triglyceride This is LDL Cholesterol James Otvos 2007

41
lipoproteins EDTA sugars

43
LDL Particle Number Distribution in MESA
LDL-C <100 mg/dL (n=1,425) 5th th th th percentile 10% (n=141) 42% (n=603) 36% (n=509) 10% (n=150) 2% (n=22) Percent of Subjects What I’m showing you here from MESA is the distribution of LDL particle number among those with low LDL cholesterol (1st quartile; <100 mg/dL). All of these people have low LDL-C and a good number of them in green have correspondingly low numbers of LDL particles, so they are the concordant individuals (ie., no discrepancy between LDL-C and LDL-P). But a lot of individuals (about half) have greater numbers of LDL particles, and some of these have very high numbers of LDL particles. And guess what – the people in the group with the greatest disconnect between LDL cholesterol and the number of LDL particles (in red), have the smallest LDL size. And they have the lowest HDL-C. And they have the highest triglycerides. So yes – people with greater numbers of LDL particles have small LDL particle size, lower HDL-C and higher TG. But it’s the LDL particle number that may be most relevant to the atherosclerotic risk of these individuals. (nmol/L) LDL Size (nm) (0.7) (0.6) (0.5) HDL-C (mg/dL) (18) (15) (11) Triglycerides (mg/dL) (60) (71) (75) AHA/ADA “Metabolic Syndrome/Metabolic Risks” meeting. San Francisco, May 3-5, 2006
 5th 20th 50th 80th percentile. 10% (n=141) 42% (n=603) 36% (n=509) 10% (n=150) 2% (n=22) Percent. of. Subjects. What I’m showing you here from MESA is the distribution of LDL particle number among those with low LDL cholesterol (1st quartile; <100 mg/dL). All of these people have low LDL-C and a good number of them in green have correspondingly low numbers of LDL particles, so they are the concordant individuals (ie., no discrepancy between LDL-C and LDL-P). But a lot of individuals (about half) have greater numbers of LDL particles, and some of these have very high numbers of LDL particles. And guess what – the people in the group with the greatest disconnect between LDL cholesterol and the number of LDL particles (in red), have the smallest LDL size. And they have the lowest HDL-C. And they have the highest triglycerides. So yes – people with greater numbers of LDL particles have small LDL particle size, lower HDL-C and higher TG. But it’s the LDL particle number that may be most relevant to the atherosclerotic risk of these individuals (nmol/L) LDL Size (nm) 21.3 (0.7) 20.5 (0.6) 20.1 (0.5) HDL-C (mg/dL) 58 (18) 47 (15) 41 (11) Triglycerides (mg/dL) 98 (60) 136 (71) 199 (75) AHA/ADA Metabolic Syndrome/Metabolic Risks meeting. San Francisco, May 3-5,")
44
LDL Particle Number Distribution in MESA
LDL-C = mg/dL 5th th th th percentile 1% (n=10) 24% (n=215) 54% (n=484) 19% (n=168) 3% (n=26) MetSyn (-) (n=903) Percent of Subjects 63% 22% (nmol/L) The reason this is important, particularly for people at this meeting, is that there is a greater prevalence of a discrepancy between LDL particle number and LDL cholesterol among those with metabolic syndrome and diabetes. Here’s more data from MESA, this time looking at LDL-P distributions in those with (bottom) and without (top) the metabolic syndrome. The subjects shown here are those with LDL-C in the second quartile ( mg/dL). For individuals with the metabolic syndrome, the LDL-P distribution is clearly shifted to the right. 63% of people with LDL-C in this range (25th -50th percentile) have LDL particle number greater than the 50th percentile, as compared to only 22% of people without metabolic syndrome. So metabolic syndrome is a condition highly enriched in people who have discrepant LDL particle number compared to LDL cholesterol. 0% (n=0) 4% (n=20) 33% (n=153) 46% (n=210) 17% (n=76) MetSyn (+) (n=459) Percent of Subjects (nmol/L) AHA/ADA “Metabolic Syndrome/Metabolic Risks” meeting. San Francisco, May 3-5, 2006
 24% (n=215) 54% (n=484) 19% (n=168) 3% (n=26) MetSyn (-) (n=903) Percent. of. Subjects. 63% 22% (nmol/L) The reason this is important, particularly for people at this meeting, is that there is a greater prevalence of a discrepancy between LDL particle number and LDL cholesterol among those with metabolic syndrome and diabetes. Here’s more data from MESA, this time looking at LDL-P distributions in those with (bottom) and without (top) the metabolic syndrome. The subjects shown here are those with LDL-C in the second quartile ( mg/dL). For individuals with the metabolic syndrome, the LDL-P distribution is clearly shifted to the right. 63% of people with LDL-C in this range (25th -50th percentile) have LDL particle number greater than the 50th percentile, as compared to only 22% of people without metabolic syndrome. So metabolic syndrome is a condition highly enriched in people who have discrepant LDL particle number compared to LDL cholesterol. 0% (n=0) 4% (n=20) 33% (n=153) 46% (n=210) 17% (n=76) MetSyn (+) (n=459) Percent. of. Subjects (nmol/L) AHA/ADA Metabolic Syndrome/Metabolic Risks meeting. San Francisco, May 3-5,")
45
CHD Event Associations of NMR LDL Particle Number (LDL-P) versus LDL Cholesterol (LDL-C)
Cromwell WC et al: J Clinical Lipidology 2007;1:

46
Brief Comments Apo B or Non-HDL versus LDL-P
Apo B and non-HDL are likely better predictors of risk than LDL-C in patients with cardiometabolic syndrome Non-HDL costs nothing extra to measure Apo B measurement does not require unique, expensive technology

47
Apo B gives equal weight to each particle: LDL, Lp(a), VLDL, IDL
Not equal atherogenicity Treatment strategies different for each particle Non-HDL similarly lumps particle types together Example 1 TC=200, HDL=50, TG=200, non-HDL=150 Example 2 TC=170, HDL=20, TG=500, non-HDL=150 Is risk equivalent for these 2 patients?

48
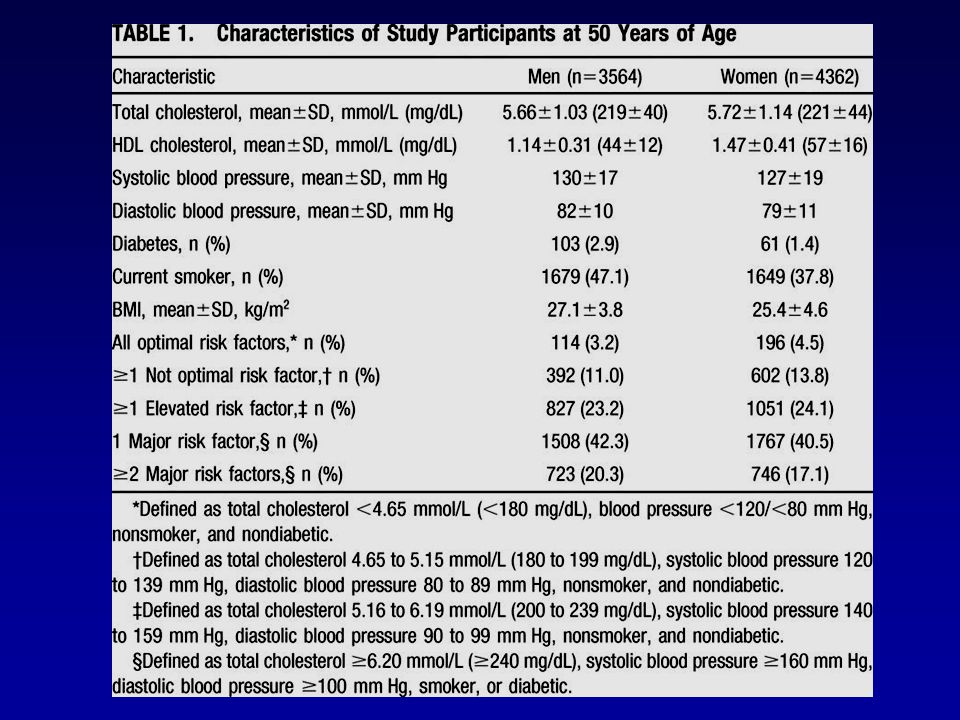
Prediction of Lifetime Risk for Cardiovascular Disease by Risk Factor Burden at 50 Years of Age
Donald M. Lloyd-Jones et al Circulation 2006;113:

51
Generic Prevention Drugs
Drug Monthly Cost Statin $4.00 Beta blocker $4.00 Metformin $4.00 ACE-inhibitor ± HCTZ $4.00 Amlodipine $4.00 All national discount pharmacy chains Lower price ($10) for 3 months supply Can potentially reduce cost further with a pill cutter
 for 3 months supply. Can potentially reduce cost further with a pill cutter.")
52
Living Under the Umbrella of Good Cardiovascular Health
LDL-C <100 FBG <100 SBP <120 Living Under the Umbrella of Good Cardiovascular Health

53
Predictions for ATP-IV
The goals for LDL-C in primary prevention will be lowered. There will be a stronger statement on hsCRP, but routine use in risk stratification or use as secondary target will not be specifically endorsed. Non-HDL-C will remain the secondary lipid target, but optional use of apo B or LDL-P will be endorsed. A new risk calculator providing lifetime risk estimates will be provided.

54
Comments? Questions?

Similar presentations






: 811-822. 1.“Measurement of LDL cholesterol (the cholesterol within.>")






 Launched by National Heart, Lung, and Blood Institute (NHLBI), a part.>")
 atherosclerosis Atherosclerosis could lead to the ischaemic.>")







” 2004 Focus = multiple risk factor assessment.>")
