Download presentation
Presentation is loading. Please wait.

1
Review of Balance /Falls and Recent studies in Amputee Rehab.
By Nerissa Grebert Westmead Hospital

2
Falls in Amputee Population
Falls pose significant risk in amputee population 20% of people with lower limb amputation fall while in inpatient rehabilitation (Pauley et al, 2006) Greater than 50% of people in the community with LLA fall in previous 12 mths with or without wearing prosthesis (Miller et al, 2001; Kulkarni et al, 1996) Falls in Amputee Population
 Greater than 50% of people in the community with LLA fall in previous 12 mths with or without wearing prosthesis (Miller et al, 2001; Kulkarni et al, 1996) Falls in Amputee Population.")
3
Significant injuries post fall
Significant injuries post fall % sustain a significant injury post fall including hemorrhage, lacerations, head trauma and fractures.(Pauley; Kulkarni; Miller) 49% of community dwellers with LLA report fear of falling, resulting in activity avoidance. Need to identify people who have lower balance and therefore are at high risk of falling. The Berg Balance test has been used in several studies to assess balance but never has been validated for the amputee population.
 49% of community dwellers with LLA report fear of falling, resulting in activity avoidance. Need to identify people who have lower balance and therefore are at high risk of falling. The Berg Balance test has been used in several studies to assess balance but never has been validated for the amputee population.")
4
From our last AustPAR meeting:
Our most routinely used outcome measures for amputees: 10m walk test 2min walk test 6min walk test TUG test AMP-PRO Some discussion on: The use of Berg Balance Test to assess falls risk and improvement in balance Whether the ‘L-test’ would be a more appropriate assessment measure for Amputees. Appropriate exercises to perform in an Amputee exercise group to improve balance, health and mobility. From our last AustPAR meeting:

5
Review of 3 articles Study by Major et al, 2013. Lamberg et al. 2014.
Validity and Reliability of the Berg Balance Scale for Community-Dwelling Persons with Lower-Limb Amputation. Barry Deathe & William C Miller, 2005. The L Test of Functional Mobility: Measurement Properties of a Modified Version of the Timed “Up & Go” Test Designed for People With Lower-Limb Amputations. Lamberg et al Harness-Supported Versus Conventional Training for people with Lower-Limb Amputation: A Preliminary Report. Review of 3 articles

6
New study by Major et al, 2013. ‘Validity and Reliability of the Berg Balance Scale for Community-Dwelling Persons with Lower-Limb Amputation’

7
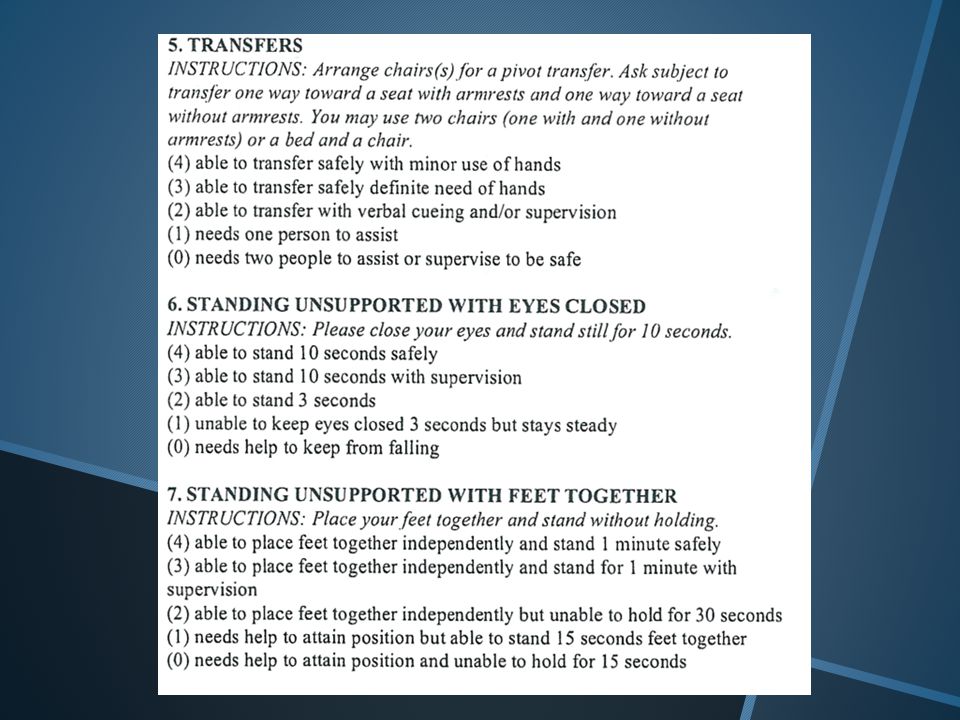
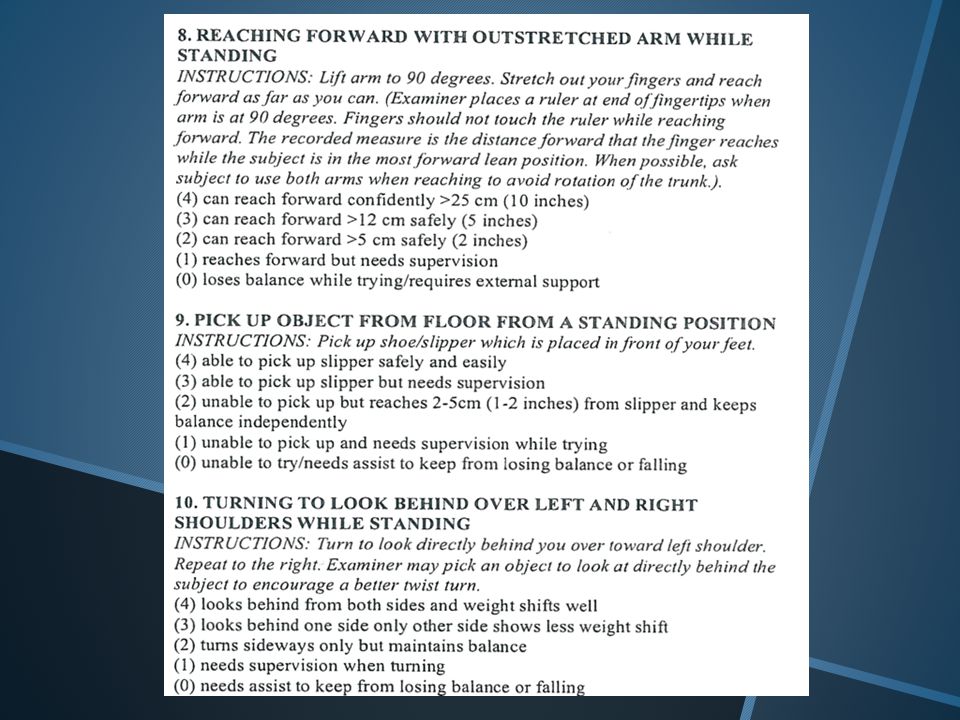
Berg Balance Test 14 item scale to measure balance
Total score out of 56 41-56=low falls risk 21-40= medium falls risk 1-20 = high falls risk Authors support a cut off score of 45 for Independent safe ambulation in non-amputee population. Berg Balance Test

13
Method Inclusion criteria
Unilateral or bilateral lower-limb loss at or proximal to ankle Used a prosthesis for ambulation +\- mobility aid Nil UL amputation Residual limb in good condition

14
Information collected on:
age, sex, height, mass, number of LLA, amputation level, amputation etiology, time since amputation frequency of prosthetic use, experience in using a prosthetic, number of falls in last 12 months, fear of falling, type of mobility aids

15
Participants completed:
Convergent validity for BBS was evaluated by collection of information on several clinical outcome measures that assess constructs related to balance and mobility. Participants completed: Activities –specific Balance confidence scale (ABC) Perceived balance and confidence in 16 ADLs Prosthesis Evaluation Questionnaire –mobility subscale (PEQ-MS) Mobility ability in ADLs while wearing a prosthesis over last 4wks
 Perceived balance and confidence in 16 ADLs. Prosthesis Evaluation Questionnaire –mobility subscale (PEQ-MS) Mobility ability in ADLs while wearing a prosthesis over last 4wks.")
16
Frenchay Activities Index (FAI) BBS x2 with different assessors
Frequency of ADLs over past 3mth and 6mth BBS x2 with different assessors The L-Test Mobility/balance performance Rise from chair, walk 3m forward, turn ®, walk 7m, walk around a floor marker, retrace path to chair, sit down. 2min walk test

17
Results Is it a good test for us to use?????

18
Results 30 participants Correlations between the BBS and other measures were stat sig. 10% achieved max points on BBS 70% achieved >50 –skewed distribution to higher scores

19
BBS -high inter-relater reliability and internal consistency
Performance tests showed stronger relationships with the BBS than questionnaires Participants scored worse on the BBS if classified as: fear of falling * }Stat. sig. Using mobility aid* } Unilat. AKA Dysvascular amputation 2+ falls in 12 months. *only 2 stat. sig.

20
Differences minimal and not sig
Differences minimal and not sig. b/w retrospective fallers- unable to ID LLA with greater risk of falling. 33% of unilateral participants scored 0-3 for standing on one leg despite all standing on intact leg. Unknown whether BBS can identify changes in balance performance resulting from therapeutic interventions.

21
The L Test of Functional Mobility:
Measurement Properties of a Modified Version of the Timed “Up & Go” Test Designed for People With Lower-Limb Amputations. Deathe & Miller, 2005.

22
Designed in Canada to assess lower limb inpatients and outpatient’s mobility.
Wanted a test which was easy to administer in a clinic setting with minimal free space and time, but didn’t have the ceiling effects of TUG test when used with younger patients. Combination of TUG, 10m, and 2min tests. Retains rise from chair and turns to L and R. Stand up, walk 3m, turn 90°, walk 7m, turn 180°, return along same path (L shape) Study to assess reliability and validity. The ‘L-test’
 Study to assess reliability and validity. The ‘L-test’")
23
Method Inclusion 102 consecutive subjects attending amputee clinic 19yrs +, unilateral TT or TF amp Prosthesis minimum 6mths Exclusion Unable to speak/read English or follow instructions Did not complete all tests Medical or prosthetic problem which prevented participation

24
Procedure Demographic data completed Walk tests (1)
Self-report questionnaires (ABC, FAI, PEQ-MS) Walk tests 2 (Different assessor) Re-test 2 weeks later (optional) Minimum 2mins rest between each test. Walk test order TUG, 10m walk test, the L-Test, 2 min walk test
 Walk tests 2 (Different assessor) Re-test 2 weeks later (optional) Minimum 2mins rest between each test. Walk test order. TUG, 10m walk test, the L-Test, 2 min walk test.")
25
Results 93 subjects completed all preliminary tests
27 subjects returned for retesting Mean time for L test 32.6 sec (TT=29.5s, TF=41.7) Excellent Intra-rater reliability and Inter- rater reliability proven Validity-Correlated well with other measures Highest correlations with other walk tests. Followed by FAI, ABC, PEQ-MS. Higher mean times shown for subjects who Were Older (39.7s) Used walking aid (43.3s) Had to concentrate on each step (44.5s) Vascular amputation (42.0s) TF amputation (41.7s) Results
 Excellent Intra-rater reliability and Inter- rater reliability proven. Validity-Correlated well with other measures. Highest correlations with other walk tests. Followed by FAI, ABC, PEQ-MS. Higher mean times shown for subjects who. Were Older (39.7s) Used walking aid (43.3s) Had to concentrate on each step (44.5s) Vascular amputation (42.0s) TF amputation (41.7s) Results.")
26
Results cont. 10 subjects had ceiling effect for TUG and L Test
14 subjects had ceiling effect for TUG but not L-Test 3 subjects had ceiling for L-test but not TUG (younger men with TT due to trauma, > 8yrs) Responsiveness to training (Initial results) 68% sure a true change occurred with 2.6 sec shift 95% sure with a 6.2 sec shift Results cont.
 Responsiveness to training (Initial results) 68% sure a true change occurred with 2.6 sec shift. 95% sure with a 6.2 sec shift. Results cont.")
27
Lamberg et al. 2014 Research questions
Harness-Supported Versus Conventional Training for people with Lower-Limb Amputation: A Preliminary Report. Research questions Can continued gait training for community based TTA with >1yr have functional improvements? Would the use of a harness for support in treadmill training lead to greater improvements in gait symmetry and endurance than no support? Lamberg et al. 2014

28
Methods Participants : Recruited through fliers/advertising 21-70 yrs
Unilateral TTA,TFA or knee disartic. >1 yr Ability to walk with prosthesis >6mths Tolerate mod intensity exercise No current gait physio Exclusion Cardiac or pulmonary disease limiting exercise Discomfort which restricts ability to walk Active wounds on either leg Methods

29
Assigned to Treadmill training with or without harness support
12 sessions (3x / wk for 4 wks) 30 mins walking on treadmill Started at comfortable unsupported walking speed Supported group started training with 30% body weight supported Support reduced by 5% increments with full weight baring at treatment session 10 Speed increased in 0.1mph increments as tol Assessed at baseline, 1 and 4 wks after training 6min walk test, TUG, ABC (self reported balance measure) Intervention
 30 mins walking on treadmill. Started at comfortable unsupported walking speed. Supported group started training with 30% body weight supported. Support reduced by 5% increments with full weight baring at treatment session 10. Speed increased in 0.1mph increments as tol. Assessed at baseline, 1 and 4 wks after training. 6min walk test, TUG, ABC (self reported balance measure) Intervention.")
30
Results 8 participants (7men) with unilateral TTA due to trauma
For all participants the distance walked in 6MWT and time to complete TUG improved 4 to each grp Mode of training found no difference 6MWT increased by 25% at 1wk post (89.6m )and 32% at 4wks post Rx(112.4m) TUG improved by 13% at 1 and 4 wks post Rx No change in ABC scores Results
and 32% at 4wks post Rx(112.4m) TUG improved by 13% at 1 and 4 wks post Rx. No change in ABC scores. Results.")
31
Evidence that treadmill training helps increase velocity and endurance of walking in 1+ years post amputation and benefits are maintained a month post exercise period Small study numbers, only traumatic- may not be generalisable to all LL amputees ? Same benefit for acute rehab phase Discussion

32
Is there a test we as a group could all agree to perform on discharge?
Conclusion

Similar presentations


















:1263-1273.>")

>")

