Download presentation
Presentation is loading. Please wait.

1
Understanding Doppler and its Current Uses in OB
Diana M. Strickland, BSBA, RDMS, RDCS

2
Continuous vs. Pulsed

3
Doppler – Moving structures -Red Blood Cells-
Wall motion – high level NOISE! Scattered waves- low level NOISE! ƒd = 2(ƒt • v • cosθ)/c
/c.")
4
Doppler – Moving structures -Red Blood Cells-
fr fr ft ft Positive shift f Negative shift Time

5
Doppler – Moving structures -Red Blood Cells-
ft ? f time

6
ft f time

7
Doppler – Moving structures -Red Blood Cells-
Optimal ft <20o

9
Doppler modes are differentiated by the way the signal is processed

10
FFT – Fast Fourier Transform
Algorithm to display multiple frequencies in a single time frame – Spectral Doppler Think of a single note versus a chord Color Doppler is an average of the spectral doppler – it can’t show each frequency in a specific time unit Standard display is BART – Blue away, Red towards Density of blood cells displayed as an intensity of gray High density (power) – bright Low density (power) – less bright Is power useful in Spectral Doppler – NO, but it is in Power Doppler Color tone determined by density (#) of cells
 – bright. Low density (power) – less bright. Is power useful in Spectral Doppler – NO, but it is in Power Doppler. Color tone determined by density (#) of cells.")
11
Diastole Plug Flow - Systole Consider spread through sample volume

12
Broadening / Narrowing
Frequency S D Envelope Time

16
Adjusting Parameters Gain Scale Baseline Filter Gate Sweep

17
Adjusting Parameters Gain Scale Baseline Filter Gate Sweep

20
Adjusting Parameters Gain Scale Baseline Filter Gate Sweep

21
Adjusting Parameters Gain Scale Baseline Filter Gate Sweep

22
Adjusting Parameters Gain Scale Baseline Filter Gate Sweep

23
Adjusting Parameters Gain Scale Baseline Filter Gate Sweep

24
Adjusting Parameters Gain Scale Baseline Filter Gate Sweep

25
Adjusting Parameters Gain Scale Baseline Filter Gate Sweep

26
Adjusting Parameters Gain Scale Baseline Filter Gate Sweep

27
Invert Size

28
Other causes for poor Doppler signal…
Frequency of transducer too high for vessel depth Lower frequency Receiver gain too low Increase gain Focal zone not optimized to area of interest – the vessel Move it ;-)
")
29
Fetal Well Being NST BPP Doppler

30
Fetal Well Being Maximum Systole / Minimum Diastole S / D (S-D)
RI (Resistance Index or Pourcelot Index) S (S-D) PI (Pulsatilty Index) A TAMV Time-averaged mean velocity
 S. (S-D) PI (Pulsatilty Index) A. TAMV. Time-averaged mean velocity.")
35
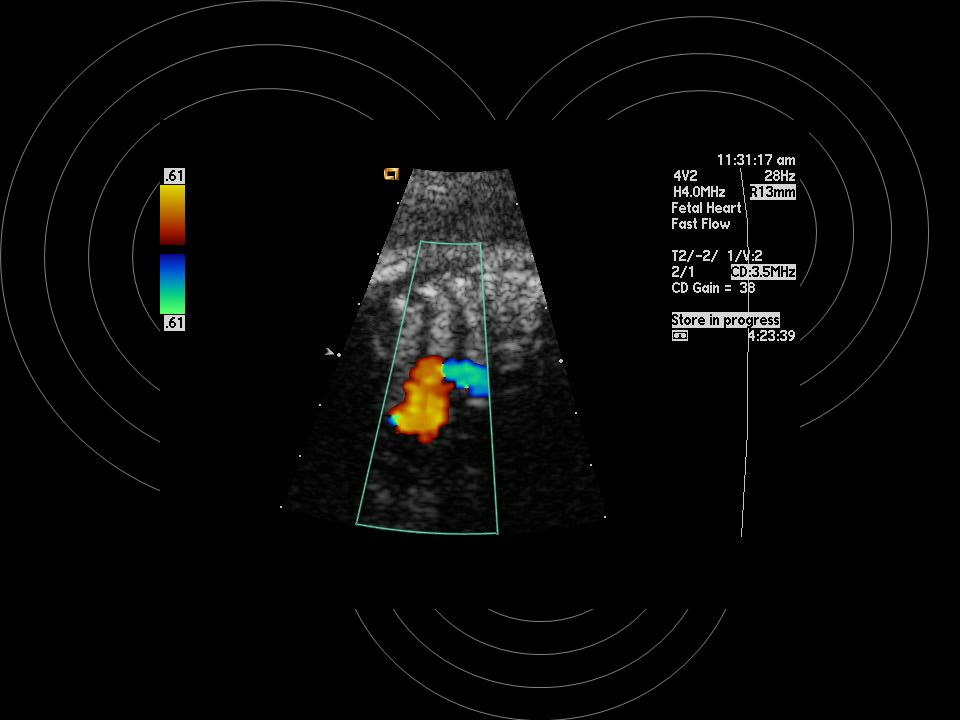
Middle Cerebral Artery MCA
Placental Insufficiency Anemia (Isoimmunization / Parvo)
")
36
MCA – Circle of Willus ACo BA IC ACA PCA PCoA MCA

38
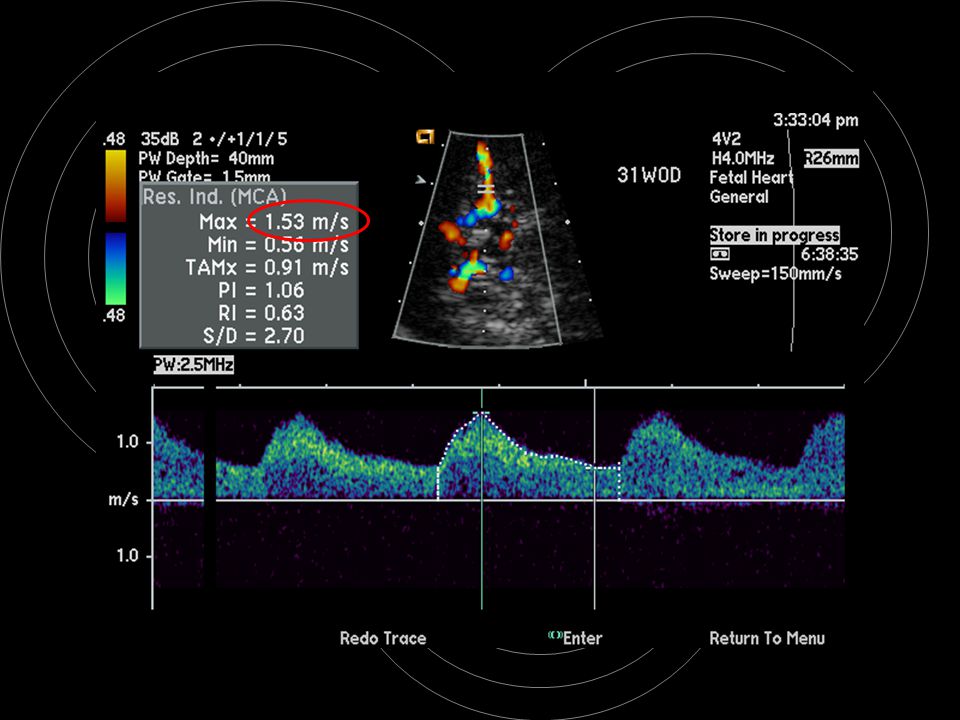
MCA – Placental Insufficiency
CerebroPlacental Ratio – CPR Originally used the anterior cerebral artery Wladimiroff, et al. RI c / RI u >1 Normal, <1 Redistribution MCA RI <70 Indicative of Redistribution Others Umb Artery RI Umb Artery PI MCA PI MCA TAMV Thoracic Aorta PI Thoracic artery TAMV UA/MCA PI ratio MCA/Thoracic Aorta PI ratio MCA PI x Thoracic TAMV

39
MCA – Placental Insufficiency
Valuable when fetus is reacting to hypoxia When physiological responses to hypoxia become exhausted, fetus cannot adapt further Decline of forward cardiac function (increase venous doppler indices) Deregulation of cardiovascular homeostasis may be seen and arterial circulation indices become less reliable.
 Deregulation of cardiovascular homeostasis may be seen and arterial circulation indices become less reliable.")
40
MCA – Placental Insufficiency
Increased diastolic umbilical vein flow = GOOD Increased diastolic cerebral flow - may signal placental problem

41
Viscosity = # of red blood cells
Anemia Viscosity = # of red blood cells

42
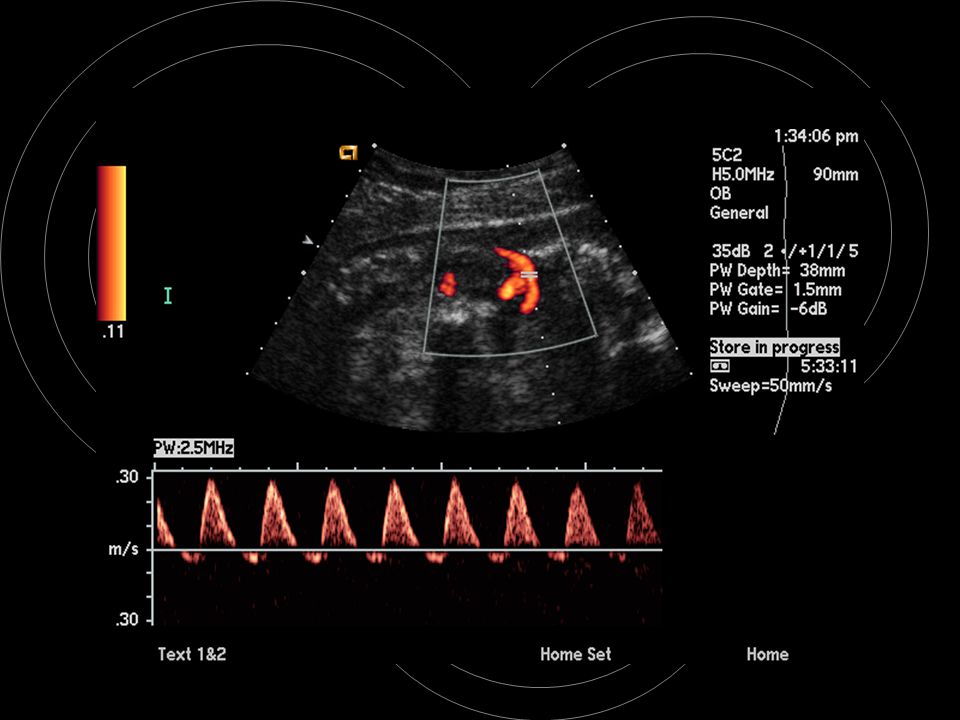
Viscosity - Normal

43
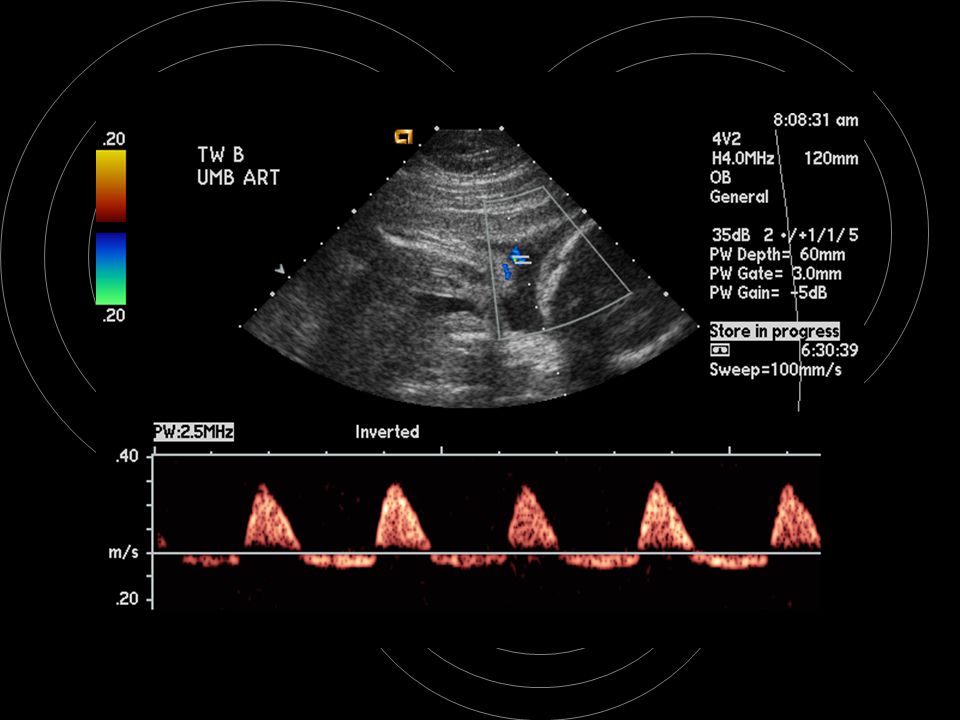
Viscosity - Anemia

45
MCA – Anemia Fetuses healthy and w/ anemia mild, moderate, and severe.
Linear models fitted to data for individual fetuses – slope was determined Average rate of change as a function of GA MCA-PSV – expressed as MoM Healthy vs. Mild anemic – NS Healthy vs. Severely anemic (P=.01) Conclusion – excellent tool to predict which fetuses will become severely anemic Detti, Mari, Moise et al, AJOG Oct 2002
 Conclusion – excellent tool to predict which fetuses will become severely anemic. Detti, Mari, Moise et al, AJOG Oct")
46
MCA - Anemia Peak Velocity (w/fetal blood sampling)
Sensitivity for moderate or severe anemia 100% FPR 12% fetuses w/o hydrops (Mari, et al, NEJM Jan 2000) Fetuses w/Parvo B19 Sens /Spec 100/100% slightly less in alloimmune group (included post transfusion follow-up) (Delle Chiaie, et al, USOG Sep 2001) Correlation between Hemoglobin and MCA-PSV becomes more accurate as severity of anemia increases. (Mari, et al, OG Apr 2002) TAMV (Abdel-Fattah, et al, BJR Sep 2002)
 Fetuses w/Parvo B19 Sens /Spec 100/100% slightly less in alloimmune group (included post transfusion follow-up) (Delle Chiaie, et al, USOG Sep 2001) Correlation between Hemoglobin and MCA-PSV becomes more accurate as severity of anemia increases. (Mari, et al, OG Apr 2002) TAMV (Abdel-Fattah, et al, BJR Sep 2002)")
47
IVC/SVC doppler Influenced by heart rate, RH hemodynamics and function, and AMOUNT of blood flowing through veins Reciprocal shift observed between IVC and SVC velocity waveforms (Smin) Changes another manifestation of blood flow redistribution toward the brain May be good to use prior to 30 weeks when doppler findings more difficult to interpret
 Changes another manifestation of blood flow redistribution toward the brain. May be good to use prior to 30 weeks when doppler findings more difficult to interpret.")
49
Fetal Echo Critical to evaluate flow an GV anomalies
Quantitate flow – Artery size, volume, VTI Direction of flow Presence of flow Quality of flow – turbulence Tei Index – (TI) MV & LV flow in one waveform Tissue Doppler MV LV
 MV & LV flow in one waveform. Tissue Doppler. MV. LV.")
52
Uterine Artery Doppler
Continuous Wave Doppler / Intraplacental IUGR (Chronic Hypertension) and Preeclampsia High AFP Little change seen in doppler indices after 26 weeks More difficult to assess when they are abnormal
 and Preeclampsia. High AFP. Little change seen in doppler indices after 26 weeks. More difficult to assess when they are abnormal.")
55
Ovarian Artery Doppler
Tumor Angiogenesis – limited vascular tone due to absence of the muscular tunica media CD screening optimal in PM women No cyclic change in ovarian volume RI < .40 96.4% Sens., 98.8% Spec., 98.2 PPV in 14,317 patients Kurjak, Fleischer, and Bourne

56
Ovarian Artery Doppler
Impedance values in benign vs. malignant lesions overlap Studies now looking at arrangement and density of vessels Neural Networks and Baysian networks are being developed and tested

Similar presentations





















 Stationary source Stationary observer Moving source>")


 patternCircular (or spherical) pattern >")

>")
 Your Organization (Line #2) Week 4 Update Joe Hoatam Josh Merritt Aaron Nielsen.>")




