Download presentation
Presentation is loading. Please wait.

1
Emergency Preparedness and Response

2
Group Discussion Have you participated in your Country Offices Emergency preparedness Planning Process? What are some identifiable vulnerabilities and risks within your country?

3
Agency Mandate Save the Childrens mandate is to respond to any emergency that puts at great risk the survival, protection, and well-being of significant numbers of children, where addressing the needs and well-being of those children is beyond the indigenous coping capacity, and where SC is able to mobilize the financial and human resources to take urgent action on their behalf. Save the Childrens goal is to respond to major sudden- onset emergencies within 72 hours of the event. Board-Mandated emergency response expectations Country Offices will respond to the needs of children during an emergency (please delete highlighted area)
.")
6
Types of Emergencies NaturalManmade Rapid onset Slow onset drought war earthquake terrorist attack cyclone flood famine epidemic volcano chemical spill plane crash civil unrest

7
Why Emergency Preparedness Planning? Quick and effective action is required during the onset of an emergency Effective action often depends on having plans in place before the disaster strikes If response is delayed, childrens lives maybe needlessly lost

8
To ensure readiness at country/regional level to respond to both natural and complex political emergencies in our programs, through collection of information, analysis and planning. Aim of SCs Emergency Preparedness Planning

9
Principal Elements of Preparedness Risks and Vulnerabilities (the broad profile of a projected emergency) External Preparedness (what other actors are capable of doing) Internal Capacity (what Save the Children is capable of doing) Preparedness Actions (results of the planning process)
 External Preparedness (what other actors are capable of doing) Internal Capacity (what Save the Children is capable of doing) Preparedness Actions (results of the planning process)")
10
Vulnerability The propensity (susceptibility or tendency) of people and things to be damaged by a hazard. A person or groups vulnerability depends on their capacity to anticipate, cope with, resist and recover from the impact of a hazard. Risk The likelihood of a disaster happening to a particular group of people Risks and Vulnerabilities

11
External Stakeholders Identify Gaps: Based on previous experience, what needs of children and their families may be unmet by external stakeholders? External Preparedness

12
What are Save the Children programmatic areas of competence? How do these areas of competence correspond to the likely gaps/weaknesses in emergency response identified above? Internal Capacity

13
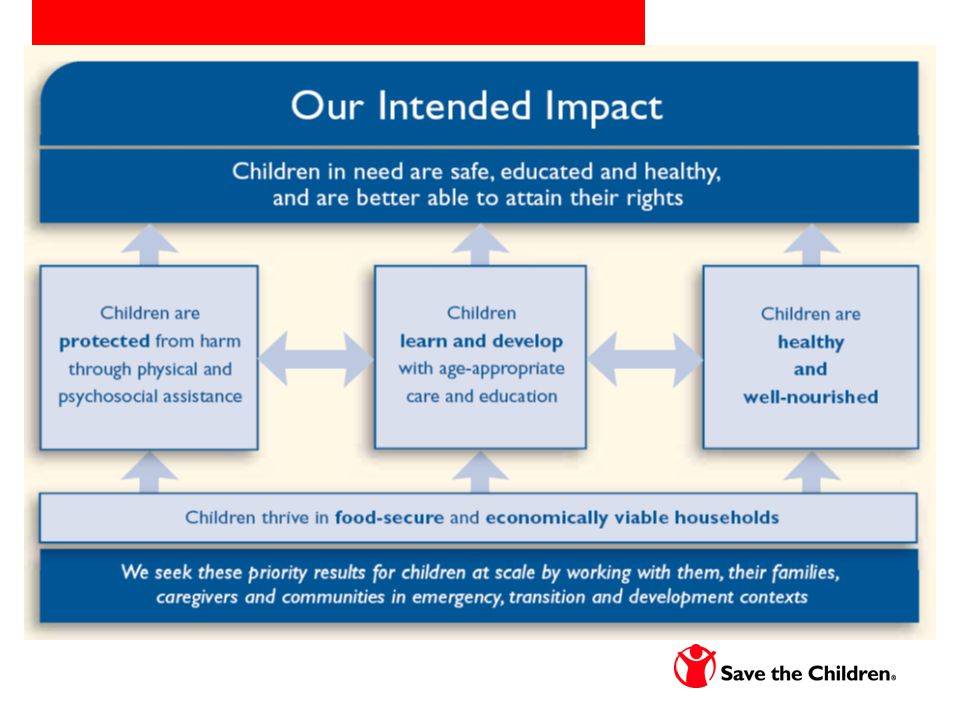
Strategic Areas for Emergency Interventions

14
Save the Children Preparedness Initiatives Country Office Emergency Preparedness and Response Plans Alliance Emergency Preparedness Plans (EPPs) Regional Rapid Emergency Deployment Initiative (REDI) teams Sector-specific trainings - Emergency Health and Nutrition, Safe Spaces Country Office Simulation exercises
 Regional Rapid Emergency Deployment Initiative (REDI) teams Sector-specific trainings - Emergency Health and Nutrition, Safe Spaces Country Office Simulation exercises")
15
Response Resources available: Emergency Response Manual Halaby-Murphy funds Operational Tools – Good Enough Guide, Sphere manual, INEE Go Kits Staff Deployments – emergency responders Technical support for proposals Management and grants support Alliance liaison and grant agreements

16
Facilitate the rapid recovery of communities affected by disaster % affected population reached by SC services % affected children reached by SC services Emergency Response (and Mitigation) Results Framework Health & Nutrition RF 1.Prevent excess morbidity and mortality in children between 1 and 59 months of age affected by crisis 2.Prevent excess morbidity and mortality in women of reproductive age and neonates affected by crisis Provisioning & HH Livelihoods RF 1. Provide for critical survival needs of affected population at HH level 2. Protect and restore household livelihoods Child Protection RF 1.Prevent and reduce physical and psychological harm to separated and vulnerable children affected by crisis Goal Sub-Goal (s) corresponding to PR program areas relevant to emergencies
 corresponding to PR program areas relevant to emergencies.")
17
Emergency Health and Nutrition Results Framework Child Health and Nutrition SO: Utilization of key young child health&nutrition practices & services % vulnerable affected households/population reached with health/watsan* Measles immunization coverage Vitamin A coverage Children ill in past two weeks who received care from appropriate providers* Percent children with acute malnutrition receiving curative service* IR1: Access to Key CHN services and supplies in a timely manner Child health facilities (peripheral health facility) available per 10,000 population In nutritional crisis, number of specialized nutrition management units <1 days return walk Population per water point/latrine IR2: Access to quality CHN services and materials Percent providers adhering to WHO standard case management practices CFR due to cholera, malaria, measles disease outbreaks Recovery rate for acutely malnourished children (moderate, severe) (Sphere) Default rate for acute malnutrition services IR3: Improved knowledge, attitudes, and skills regarding key CHN practices and services Knowledge of appropriate water storage and use Knowledge of hand- washing practices IR4: Enabling social and policy environment for emergency operations as well as the transition into development Barriers limiting universal access to key services addressed (religion, language, gender, political inclination, user fees) Accommodating environment for nutrition programs (OTP) Sub-Goal: Prevent excess morbidity and mortality in children between 1 and 59 months of age affected by crisis Under-five mortality Rate Acute Malnutrition rate (both moderate and severe) Sub-goal and SO indicators include agency indicators. *Note that only service utilization indicators such as this one may be available for response phase in sudden-onset

18
Emergency Child Health and Nutrition Interventions Disease Outbreaks Child HealthNutrition (CTC, etc.) Hand washing at appropriate times Proper disposal of excreta Consumption of adequate quantities of safe water Timely appropriate care for cholera or other disease outbreaks Immunization of all children 6months – 15yrs against measles Timely recognition, care seeking, diagnoses and treatment of Pneumonia, Malaria, Measles, Diarrhea Children sleep under LLITN or residually sprayed rooms Immunization against major vaccine preventable childhood diseases, Timely recognition, care seeking, diagnoses and treatment of acute malnutrition Micronutrient supplementation for children, including vitamin A Timely appropriate complementary feeding and continued BF through age two Exclusive BF through 6 months
 Hand washing at appropriate times Proper disposal of excreta Consumption of adequate quantities of safe water Timely appropriate care for cholera or other disease outbreaks Immunization of all children 6months – 15yrs against measles Timely recognition, care seeking, diagnoses and treatment of Pneumonia, Malaria, Measles, Diarrhea Children sleep under LLITN or residually sprayed rooms Immunization against major vaccine preventable childhood diseases, Timely recognition, care seeking, diagnoses and treatment of acute malnutrition Micronutrient supplementation for children, including vitamin A Timely appropriate complementary feeding and continued BF through age two Exclusive BF through 6 months")
19
Emergency Health and Nutrition Results Framework Maternal and Newborn Health and Nutrition SO: Utilization of key maternal and neonatal practices and services Met needs Obstetrics case fatality rate Deliveries attended by skilled health personnel* Sexual violence victims reporting for treatment within five days Contraceptive prevalence rate IR1: Access to Key MN services and supplies in a timely manner Number of facilities providing EmOC per 50,000 Number of facilities providing essential neonatal care IR2: Access to quality CHN services and materials Percent providers adhering to WHO standard case management practices (EMOC and ENC) Proportion of facilities adhering to universal precautions for preventing HIV/AIDS transmission IR3: Improved knowledge, attitudes, and skills regarding key CHN practices and services Knowledge of immediate and exclusive breastfeeding IR4: Enabling social and policy environment for emergency operations as well as the transition into development Barriers limiting universal access to key services addressed (religion, language, gender, political inclination, security) Breast milk code adhered to within emergency context Sub-Goal: Prevent excess morbidity and mortality in women of reproductive age and neonates affected by crisis *Note that only service utilization indicators such as this one may be available for response phase in sudden-onset
 Proportion of facilities adhering to universal precautions for preventing HIV/AIDS transmission IR3: Improved knowledge, attitudes, and skills regarding key CHN practices and services Knowledge of immediate and exclusive breastfeeding IR4: Enabling social and policy environment for emergency operations as well as the transition into development Barriers limiting universal access to key services addressed (religion, language, gender, political inclination, security) Breast milk code adhered to within emergency context Sub-Goal: Prevent excess morbidity and mortality in women of reproductive age and neonates affected by crisis *Note that only service utilization indicators such as this one may be available for response phase in sudden-onset")
20
Alliance Joint Emergency Preparedness Planning Joint trainings Unified responses

21
Emergency Preparedness and Response Plan Example Save the Children Alliance Indonesia

22
Table of Contents I.Introduction Criteria for responding Management structures II.Threat Analysis Risk mapping III.External and Internal Capacity IV.Preparedness and Response Actions V.Operational Resources and Systems

23
A. Communications B.Transportation C.Finance D.Procurement E.Warehousing F.Customs G.Administration H.Human Resources I.Security

24
Annexes 1.Sitrep format 2.Emergency Response Team structure 3.Alliance secondment agreement 4.Deployment information sheet 5.Contingency plans 6.Difference of staff benefits between Alliance members 7.Emergency Response Team TOR

25
September – November 2006 Emergency Response Team formed, trained Pre-positioning of emergency supplies: 12 safe play area tents and cooperative game kits 45 school tents 3,000 household kits 6,000 hygiene kits 3,000 family tarps and plastic mats Based on previous emergencies, predicted an average of 200,000 IDPs could be affected. Save the Children wanted to be able to reach 10% of that population within the first 7 days (needed enough relief supplies pre-positioned for 20,000 people). Due to budget constraints, had to reduce the coverage to 7.5%.
. Due to budget constraints, had to reduce the coverage to 7.5%..")
26
Aceh Floods December 22, 2006 Immediate actions: Deployment of Emergency Response Team members Moved pre-positioned supplies to impact area Staff stepped up when key decision-makers were on holiday

27
December 23 A team from Save the Children health went to Bireun to conduct a quick assessment and purchased basic medicine Lhokseumawae has been split into three teams, one for procurement and two for assessments. Purchase in Lhokseumawe: blankets, pots, pans, plastic sheeting, rice, noodles and 10,000 bottles for distribution. Apparently Lhokseumawe is flooding as well, 30 cm of water near our office, so it is not going to be easy to shop. The assessment team went to do the field and do distribution according to the most immediate needs Faruque has contacted WFP who are doing assessments for food distribution.

28
December 24 An estimated total of 216,000 people affected Health - our team has listed most common ailments as respiratory infections, stomach complaints – including diarrhea, fevers, skin conditions, rheumatism Save the Children Response to date: North Sumatra -1,300 tarpaulins, 1,658 hygiene kits, 590 household kits Aceh - 10,000 bottles water, 10,000 packs noodles, 10,000 packs high energy biscuits, One temporary clinic

29
December 25 Many areas are still in accessible due to flooding and landslides Total Affected population = 367,220 Save the Children response to-date: North Sumatra: 1,300 tarpaulins, 1,658 hygiene kits, 590 household kits Aceh: 15,000 liters of water, 10,000 packs noodles, One temporary clinic and supplies, Distribution of medical supplies to six health centers SC will be distributing 20.5 MT rice, 1,542 liters oil, 15,000 liters water and 8,000 sanitary napkins on Tuesday and Wednesday in Aceh Utara.

30
Group Discussion Have you responded to an emergency? If so, what was your role?

Similar presentations










 For the Your Picture.>")


 in Humanitarian Situations in the Asia and the Pacific Region Ms Devanna de la Puente Inter-agency Regional Emergency.>")


 – (Date) Session 5.1: Tools for Integrating Protection Needs Adapted from presentation developed by UNDP.>")



