Download presentation
Presentation is loading. Please wait.

1
Management of Advanced Head & Neck Squamous Cell Carcinoma in The Molecular Era
Mohamed Abdulla (M.D.) Department of Clinical Oncology Kasr El-Aini School of Medicine Cairo University Alexandria, 15/01/09
 Department of Clinical Oncology. Kasr El-Aini School of Medicine. Cairo University. Alexandria, 15/01/09.")
2
Epidemiology of SCCHN Squamous cell carcinoma of the head and neck (SCCHN): new cases in Europe annually SCCHN: mortality in Europe is annually SCCHN accounts for 6% of all malignancies Worldwide annual incidence of SCCHN: new patients; deaths GLOBOCAN 2002 (

3
Challenging Issues: Stages III & IV SCCHN Patients:
2/3 of Patients at Presentation. 5-Year OAS = 30-35%. 20% will develop failures below the clavicles. Many Modalities of Treatment with Different Sequencing Matters. Impact of Innovations in Loco-regional Management upon Patient’s Survival.

4
Treatment Modalities in SCCHN
Early stage Locally advanced Recurrent and/or metastatic Refractory RT alone CT Palliation RT + CT Surgery

5
Lessons Learned from Meta-Analysis of Chemotherapy Trials over Years
Investigator No. of Trials No. of Patients Sequencing Survival Advantage Stell, 1992 28 3977 All Concurrent 2.8% 7% Browman, 1994 10 1626 Neoadjuvant Negative Munro, 1995 54 7443 6.5% 12.1% El-Sayed & Nelson, 1996 25 -- 4% 8% Bourhis & Pignon, 1999 10741 2.8 – 6.5% 7 – 12.1%

6
Lessons Learned from Meta-Analysis of Chemotherapy Trials over Years
Cancer Care Ontario Practice Guidelines, 2000: 18 Randomized Controlled Trials. 3192 Patients. Absolute Mortality Risk Reduction with Concurrent Cth = 11%. Absolute Mortality Risk Reduction with Monotherapy Platinum Based Cth = 12%. The Cost of Incremental Acute Toxicity.

7
Lessons Learned from Meta-Analysis of Chemotherapy Trials over Years
ASCO 2004: 87 Trials. 16000 Patients. Survival Advantage: All: 5% at 5 y. Concurrent: 11% at 5 y. Platinum Monotherapy ASCO 2007

8
Lessons Learned from Meta-Analysis of Chemotherapy Trials over Years
Concurrent Chemotherapy Improves Survival by 8-11%. Platinum Monotherapy is Preferred. Little Role in Pure Neoadjuvant or Adjuvant Fashions.

9
Molecular Biology of Head & Neck SCC.

11
EGF Pathway EGFR family EGFR HER2 HER3 HER4 Adapted from:
The ErbB family of Proteins comprises 4 structurally related receptor tyrosin kinases EGFR HER2 HER3 HER4 Adapted from: Ciardiello F, et al. N Engl J Med. 2008;358:

12
Tyrosine Kinase Domain
EGF Pathway EGFR: transmembrane protein Extracellular Domain Transmembrane Domain Intracellular Domain Tyrosine Kinase Domain Adapted from: Ciardiello F, et al. N Engl J Med. 2008;358:

13
EGF Pathway Receptor specific ligands NRGs β-cellulin HB-EGF
EGF TGFα β-cellulin HB-EGF Epiregulin Amphiregulin NRGs And about 13 polypeptide extracellular ligands EGFR HER2 HER3 HER4 Adapted from: Ciardiello F, et al. N Engl J Med. 2008;358:

14
EGF Pathway EGFR activation mediates multiple processes Shc PI3K Grb2
AKT Sos-1 Ras mTOR Raf MEKK-1 MEK MKK-7 JNK ERK Adapted from: Ciardiello F, et al. N Engl J Med. 2008;358:

15
TGFα Interleukin-8 bFGF VEGF
EGF Pathway Metastasis Angiogenesis Shc PI3K Raf MEKK-1 MEK MKK-7 JNK ERK Ras mTOR Grb2 AKT Sos-1 TGFα Interleukin-8 bFGF VEGF Proliferation Apoptosis Resistance Transcription

16
Prognostic & Predictive Importance of EGFR Over expression:
> 90% of all HNSCC Patients. Poor Response to ttt with Chemo-Radiotherapy Through Repopulation of Clonogenic Cells during ttt. Compromised L.C., DFS, OAS. Associated with Cisplatin-Resistance.

18
Cetuximab Experience:
ERBITUX + RT in locally advanced SCCHN: Phase III study design RT (n=213) Stage III and IV non-metastatic SCCHN (n=424) R ERBITUX + RT (n=211) ERBITUX initial dose (400 mg/m2) 1 week before RT ERBITUX (250 mg/m2) + RT (weeks 2–8) Stratified by KPS Nodal involvement Tumor stage RT regimena To date the only targeted therapy that has demonstrated significant improvement in the outcome of patients with locally advanced HNSCC patients compared with standard therapy alone in a controlled phase III is the EGFR targeting monoclonal antibody Cetuximab (Erbitox) Primary endpoint: Duration of locoregional Control Secondary endpoints: OS, PFS, RR, and safety aInvestigators’ choice Bonner J, et al. N Engl J Med 2006;354:567–578
 Stage III and IV non-metastatic SCCHN. (n=424) R. ERBITUX + RT (n=211) ERBITUX initial dose (400 mg/m2) 1 week before RT. ERBITUX (250 mg/m2) + RT (weeks 2–8) Stratified by. KPS. Nodal involvement. Tumor stage. RT regimena. To date the only targeted therapy that has demonstrated significant improvement in the outcome of patients with locally advanced HNSCC patients compared with standard therapy alone in a controlled phase III is the EGFR targeting monoclonal antibody Cetuximab (Erbitox) Primary endpoint: Duration of locoregional Control. Secondary endpoints: OS, PFS, RR, and safety. aInvestigators’ choice. Bonner J, et al. N Engl J Med 2006;354:567–578.")
19
Cetuximab Experience:
ERBITUX + RT improves significantly long term survival, with nearly half of the patients alive at 5 years 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0.0 ERBITUX + RT RT p-value 5-year OS rate 46% 36% 0.02 ERBITUX + RT Probability of Overall Survival RT HR=0.73 (0.56–0.95) p = 0.02 Months Treatment Total Death Alive Median Erbitux + RT RT Bonner J.A, et al. as presented ASTRO 2008
 p = Months. Treatment Total Death Alive Median. Erbitux + RT RT Bonner J.A, et al. as presented ASTRO")
20
Bonner Trial Overview:
Significant Increase in Durability of Locoregional Control (HR = 0.68, P = 0.05). Better Median Duration for Locoregional Control (24.4 vs 14.9 months). Significant Reduction in Risk of Death (26%) (HR 0.74, P = 0.03). Independent Clinical Benefit. No Significant Increase in Grade 3 Co-morbid Events Apart From Acniform Rash & Fusion Reactions. No Significant Adverse Affection of Quality of Life. Incorporation of Molecularly Targeted Agents in The Primary Treatment of Squamous Cell Carcinoma of The Head & Neck Jacques Bernier. Hematol Oncol Clin N Am. 22(2008)
. Better Median Duration for Locoregional Control (24.4 vs 14.9 months). Significant Reduction in Risk of Death (26%) (HR 0.74, P = 0.03). Independent Clinical Benefit. No Significant Increase in Grade 3 Co-morbid Events Apart From Acniform Rash & Fusion Reactions. No Significant Adverse Affection of Quality of Life. Incorporation of Molecularly Targeted Agents in The Primary Treatment of Squamous Cell Carcinoma of The Head & Neck. Jacques Bernier. Hematol Oncol Clin N Am. 22(2008)")
21
Benefit under CTX + ERBITUX
Forest Plot of the Hazard Ratios by Pre-Treatment Characteristics – 5-year Update Subgroup Primary tumor site Oropharynx Larynx Hypopharynx Tumor stage T1–T3 T4 RT regimen Once daily Twice daily Concomitant boost Overall stage Stage I-III Stage IV Nodal stage N0 N1–N3 KPS 50–80 90–100 Gender Male Female EGFR status ≤50% positive >50% positive Unknown Age <65 years ≥65 years 0.0 0.6 1.2 1.8 Benefit under CTX + ERBITUX Benefit under CTX alone Bonner J.A, et al. as presented ASTRO 2008

22
ERBITUX + RT: Overall Survival by Severity of Acne/Rash
1.00 0.75 0.50 0.25 0.00 ERBITUX + RT Grade 2-4 Acne/Rash Probability of survival (%) grade 0–1 grade 2-4 n Median p=0.002 HR (CI)= 0.49 (0.34 – 0.72) ERBITUX + RT Grade 0-1 Acne/Rash Time (Month) Bonner J.A, et al. as presented ASTRO 2008
 grade 0–1 grade 2-4. n Median p= HR (CI)= 0.49 (0.34 – 0.72) ERBITUX + RT Grade 0-1 Acne/Rash Time (Month) Bonner J.A, et al. as presented ASTRO")
23
ERBITUX + RT: Relevant grade 3–5 adverse events
RT (n=212) ERBITUX + RT (n=208) p-valuea Mucositis/stomatitis 52% 56% 0.44 Dysphagia 30% 26% 0.45 Radiation dermatitis 18% 23% 0.27 Xerostomia 3% 5% 0.32 Fatigue/malaise 4% 0.64 Acne-like rash 1% 17% <0.001 Infusion-related reactionsb 0% 0.01 aFisher’s exact test bListed for its relationship to ERBITUX Bonner J, et al. N Engl J Med 2006;354:567–578
 ERBITUX + RT (n=208) p-valuea. Mucositis/stomatitis. 52% 56% Dysphagia. 30% 26% Radiation dermatitis. 18% 23% Xerostomia. 3% 5% Fatigue/malaise. 4% Acne-like rash. 1% 17% < Infusion-related reactionsb. 0% aFisher’s exact test. bListed for its relationship to ERBITUX. Bonner J, et al. N Engl J Med 2006;354:567–578.")
24
No Phase III Direct Head to Head Comparison.
Cetuximab + Rth CRT No Phase III Direct Head to Head Comparison. Between-Study Comparison of Phase III Studies 20 & months Survival Advantages. Discretion of The Treating Physician.

25
Disease Specific Survival
Cetuximab + Rth vs CRT?? Retrospective Analysis at ONE Center. 29 Patients (Cetuximab + Rth) vs 103 Patients (CRT). Caudell JJ, Sawrie SM, Spencer SA, et al. Locoregionally advanced head and neck cancer treated with primary radiotherapy: a comparison of the addition of cetuximab or chemotherapy and the impact of protocol treatment. Int J Radiat Oncol Biol Phys 2008 [E-pub]. Item Cetuximab + Rth CRT P-Value 3-Y L.C. 71% 75% NS Distant Metastases FS 92% 87% Disease Specific Survival 79% 77% 3-Y OAS 76% 61% 0.02
 vs 103 Patients (CRT). Caudell JJ, Sawrie SM, Spencer SA, et al. Locoregionally advanced head and neck cancer treated with primary radiotherapy: a comparison of the addition of cetuximab or chemotherapy and the impact of protocol treatment. Int J Radiat Oncol Biol Phys 2008 [E-pub]. Item. Cetuximab + Rth. CRT. P-Value. 3-Y L.C. 71% 75% NS. Distant Metastases FS. 92% 87% Disease Specific Survival. 79% 77% 3-Y OAS. 76% 61%")
26
Considerable Number of Non-Protocol Patients in CRT Arm.
Inclusion of Higher Number of T-4 Patients in CRT Arm.

27
CT or Erbitux effect (p-value)
Comparison of overall survival advantage of different combinations (MACH-NC meta-analyses, Bonner study) Hazard ratio (95% CI) CT or Erbitux effect (p-value) Absolute benefit At 2 yearsa At 5 yearsa Adjuvant CT+RT1 0.98 (0.85–1.19) 0.74 1% Neoadjuvant CT +RT1 0.95 (0.88–1.01) 0.10 2% Concomitant CT + RT1 0.81 (0.76–0.88) <0.0001 7% 8% ERBITUX + RT2 0.73 (0.56–0.95) 0.02 10% aAssuming survival rates of 50% at 2 years and 32% at 5 years in control groups Pignon JP, et al. Lancet 2000;355:949–955 Bonner J.A, et al. as presented ASTRO 2008
 Hazard ratio (95% CI) CT or Erbitux effect (p-value) Absolute benefit. At 2 yearsa. At 5 yearsa. Adjuvant CT+RT (0.85–1.19) % Neoadjuvant CT +RT (0.88–1.01) % Concomitant CT + RT (0.76–0.88) < % 8% ERBITUX + RT (0.56–0.95) % aAssuming survival rates of 50% at 2 years and 32% at 5 years in control groups. Pignon JP, et al. Lancet 2000;355:949–955. Bonner J.A, et al. as presented ASTRO")
28
ERBITUX+RT provides a high reduction in the risk of death at 5 years
Comparison of the reduction in the risk of death (MACH-NC meta-analyses, Bonner study) ERBITUX+RT provides a high reduction in the risk of death at 5 years Adjuvant CT+RT1 Neoadjuvant CT+RT1 Concomitant CT+RT1 ERBITUX +RT2 0% -5% -2% -5% -10% -15% -20% -19% -25% -30% -27% 1) Pignon JP, et al. Lancet 2000;355:949–955 2) Bonner J.A, et al. ASTRO 2008
 ERBITUX+RT provides a high reduction in the risk of death at 5 years. Adjuvant CT+RT1. Neoadjuvant CT+RT1. Concomitant CT+RT1. ERBITUX +RT2. 0% -5% -2% -5% -10% -15% -20% -19% -25% -30% -27% 1) Pignon JP, et al. Lancet 2000;355:949–955. 2) Bonner J.A, et al. ASTRO")
29
Cetuximab + CRT in Phase III Trials in Advanced HNSCC:
Radiation Therapy Oncology Group: Cisplatin-Based CRT +/- Cetuximab. Groupe Oncologie Radiotherapie Tet et Cou: Rth + Cetuximab vs Cetuximab + Carboplatin/5-Fu-Based CRT. Also there is some published data about the incorporation of Cetuximab into neoadjuvant chemotherapy protocols as Paclitaxel/Carboplatin and TPF with reported higher response rates as well as pathologic complete remissions. Pfister DG, Su YB, Kraus DH, et al. Concurrent cetuximab, cisplatin, and concomitant boost radiotherapy for locoregionally advanced, squamous cell head and neck cancer: a pilot phase III study of a new combined-modality paradigm. J Clin Oncol 2006;24(7):1072–8
:1072–8.")
30
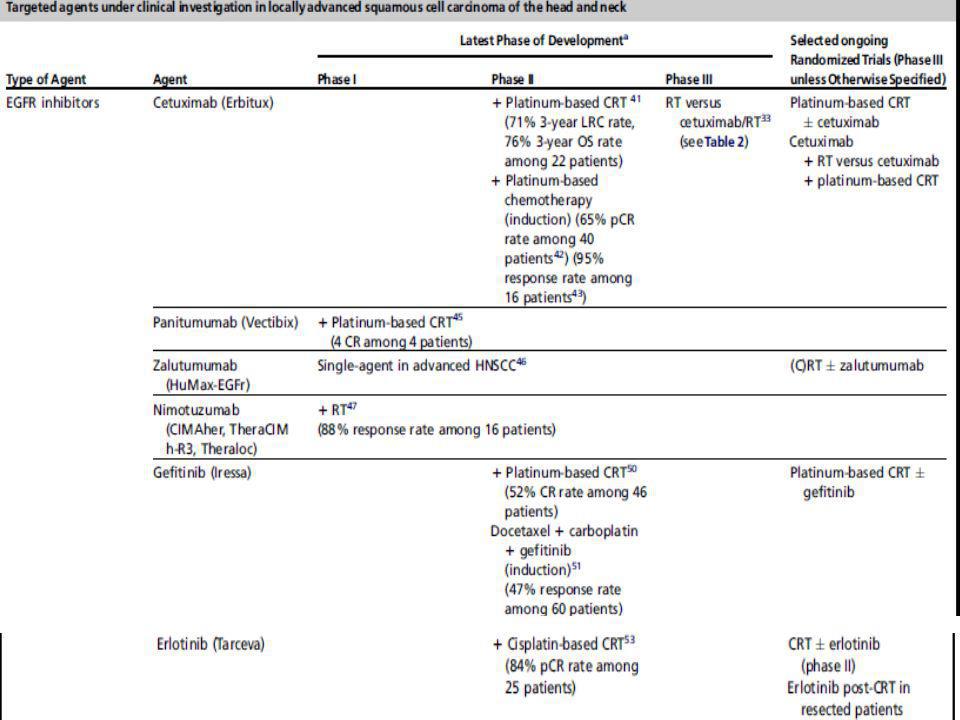
Epidermal Growth Factor Tyrosin Kinase Inhibitors Phase I/II Trials:
Other Epidermal Growth Factor Receptor-Targeted Monoclonal Antibodies Phase I/II: Panitumumab (Vectibix). Zalutumumab (Humax-EGFr). Nimotuzumab (Theraloc). Epidermal Growth Factor Tyrosin Kinase Inhibitors Phase I/II Trials: Gefitinib (Iressa) + Cisplatin + Accelerated Rth: CR in 52% (46 Patients). Erlotinib (Tarceva) + Cisplatin-Based CRT: CR in 84% (25 Patients).
. Zalutumumab (Humax-EGFr). Nimotuzumab (Theraloc). Epidermal Growth Factor Tyrosin Kinase Inhibitors Phase I/II Trials: Gefitinib (Iressa) + Cisplatin + Accelerated Rth: CR in 52% (46 Patients). Erlotinib (Tarceva) + Cisplatin-Based CRT: CR in 84% (25 Patients).")
31
VEGF Inhibitor, Bevacizumab (Avastin):
Phase I/II trials. Significant Morbidity included; Fistula Formation (11%) & Ulceration/Tissue Necrosis (9%). Agents Directed at Multiple Molecular Targets: Lapatinib (Tycerb): Phase II Trial; Cisplatin-Based CRT +/- Lapatinib. Vandetanib (Zactema): Phase II Vandetanib and Docetaxel in Locally Advanced HNSCC not amenable to Surgery or Rth.
 & Ulceration/Tissue Necrosis (9%). Agents Directed at Multiple Molecular Targets: Lapatinib (Tycerb): Phase II Trial; Cisplatin-Based CRT +/- Lapatinib. Vandetanib (Zactema): Phase II Vandetanib and Docetaxel in Locally Advanced HNSCC not amenable to Surgery or Rth.")
Similar presentations




 experience.>")









 in patients with T3-4 rectal.>")





