Download presentation
Presentation is loading. Please wait.

1
Patient – Ventilator Asynchrony
Dr Vincent Ioos Medical ICU – PIMS APICON 2008 Workshop on Mechanical Ventilation

2
Goal of mechanical ventilation
Do you mechanically ventilate your patient to reverse diaphragmatic fatigue ? or Do you encourage greater diaphragm use to avoid ventilator-induced diaphragmatic dysfunction?

4
Patient triggered ventilation
Assisted mechanical ventilation Avoid ventilator induced diaphragmatic dysfunction Providing sufficient level of ventilatory support to reduce patient’s work of breathing

6
Volume or pressure oriented?

7
Volume oriented modes Inspiratory flow is preset
Inspiratory time determines the Vt The variable parameter is the airway peak and plateau pressure

8
Equation of insuflated gases in flow assist control ventilation
Describes interactions between the patient and the ventilator Pressure required to deliver a volume of gas in the lungs is determined by elastic and resistive properties of the lung Paw = Vt/C +VR + PEP

9
C = Vt / P and P = P Plat - PEEP
Airway Pressure Paw= Po + Vt/C + RV C = Vt / P and P = P Plat - PEEP

10
Flow shapes

11
Pressure oriented modes
Pressure in airway is the preset parameter Flow is adjusted at every moment to reach the preset pressure The variable parameter is Vt

12
Equation of motion in pressure support ventilation
Paw + Pmus = Vt/C + VxR + PEP Pressure = pressure applied by the ventilator on the airway + pressure generated by respiratory muscles Pmus is determined by respiratory drive and respiratory muscle strenght

13
Determinant factors of inspiratory flow in PSV
Pressure support setting Pmus (inspiratory effort) Airway resistance Respiratory system compliance Vt directly depends on inspiratory flow, but also on auto-PEEP (decreases the driving pressure gradient)
 Airway resistance. Respiratory system compliance. Vt directly depends on inspiratory flow, but also on auto-PEEP (decreases the driving pressure gradient)")
15
Look at the curves !

16
A challenge for the intensivist
Discomfort anxiety Increased work of breathing Increased requirement of sedation Increased length of mechanical ventilation Increased incidence of VAP

17
Patient-ventilator asynchrony
Mechanical ventilation: 2 pumps Ventilator controlled by the physician Patient’s own respiratory muscle pump Mismatch between the patient and the ventilator inspiratory and expiratory time time Patient « fighting » with the ventilator

20
Ventilation phases

21
Trigger asynchrony Ineffective triggerring: muscular effort without ventilator trigger Double triggerring Auto-triggering Insensitive trigger: triggering that requires excessive patient effort

22
Ineffective triggering

24
Double triggering Cough Sighs Inedaquate flow delivery

25
Auto-triggering Circuit leak Water in the circuit Cardiac oscillations
Nebulizer treatments Negative suction applied trough chest tube

28
Flow asynchrony Fixed flow pattern (volume oriented)
Variable flow pattern (pressure oriented)
")
29
Volume oriented ventilation (fixed flow pattern)
Inspiratory flow varies according to the underlying condition If patient’s flow demand increases, peak flow should be adjusted accordingly Usually, peak flow is too low Dished-out appearance of the presure-wave-form Importance of flow-pattern

31
Ineffictive triggering at 30 l/mn
Increase in flow rate Subsequent increase of expiratory time Decreased dynamic hyperinflation Subsequent decrease in ineffictive trigerring

32
Importance of flow pattern
Increase in peak-flow setting fron 60 to 120 l/mn eliminated scooped appearance of the airway pressure waveform

33
Pressure oriented ventilation (variable flow)
Peak flow is depending on : Set target pressure Patient effort Respiratory system compliance Adjustement : rate of valve opening = rise time = presure slope = flow acceleration

37
Termination asynchrony
Ventilator should cycle at the end of the neural inspiration time Delayed termination: Dynamic hyperinflation Trigger delay Ineffective triggering Premature termination

40
Set inspiratory time < 1 sec

41
PSV = 10 cmH2O Patient 1 Patient 2
Inspiratoy flow terminate despite continued Pes defelection Double Trigerring

42
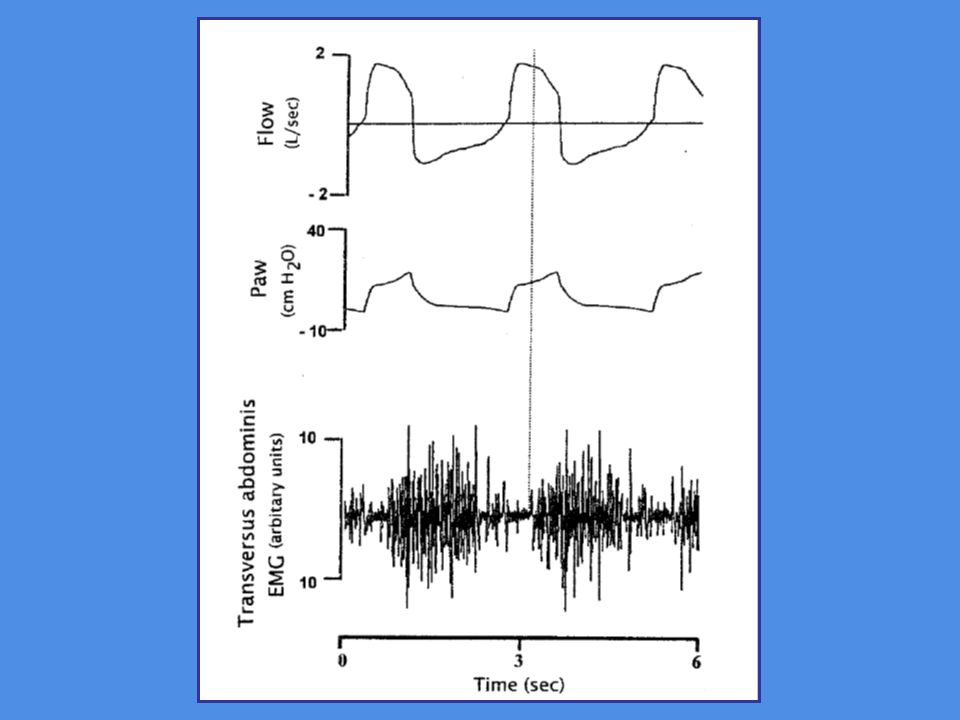
Expiratory asynchrony
Shortened expiratory time: Auto-PEEP trigger asynchrony Delay in the relaxation of the expiratory muscle activity prior to the next mechanical inspiration Overlap between expiratory and insiratory uscle activity Prolonged expiratory time

43
Auto-PEEP created by flow patterns that increases inspiratory time
Lower peak flow during control ventilation Switch from constant flow to descending ramp flow Inadequate pressure slope during presure controlled ventilation Termination criteria that prolong expiratory time during PSV

47
Conclusion Look at your patient ! Look at the curves !
Have a good knowledge of the ventilation modalities of the ventilator you are using Excessive ventilatory support leads to ineffective triggering Do not forget to set trigger sensitivity, to avoid excessive effort and auto-triggering

Similar presentations