Download presentation
Presentation is loading. Please wait.

1
ANTERIOR CERVICAL DISCECTOMY WITH FUSION (ACDF)
Presented by Robert Nelson BSN, MBA, MHA, SCRN, CNRN, ONC Vice President Neuroscience and Orthopedics HCA East Florida Division AHA – evidenced based information Acute treatment options Secondary prevention steps Stroke program JCAHO - Primary Stroke Certification

2
OBJECTIVES Discuss the simple anatomy and physiology of the cervical spine Discuss the Nerve Root Level, Function and Radicular Distribution Discuss the diagnostic studies completed before ACDF surgery Discuss Degenerative Cervical Spine Disorders Discuss surgical treatment of the cervical spine with Anterior approach and fusion (ACDF)
")
3
CERVICAL SPINE Cervical Vertebrae :
The cervical spine has seven vertebrae. The body, or centrum, of the vertebra is located anteriorly The vertebral foramen, referred to as the spinal canal, is behind the vertebral body.

4
CERVICAL DISCS With the exception of C1–C2, an intervertebral disc resides between each of the cervical vertebral bodies. Why?

5
CERVICAL DISC Each intervertebral disc provides support and facilitates movement, while also resisting excessive movement. The disc permits slight anterior flexion, posterior extension, lateral flexion, rotation, and some circumduction (Schnuerer, Gallego, & Manuel, 2003). The disc is the largest avascular structure in the body (Anderson & Albert, 2003).
. The disc is the largest avascular structure in the body (Anderson & Albert, 2003).")
6
CERVICAL DISC Cervical discs are composed of the nucleus pulposus, an inner capsule with tissue the consistency of crabmeat, and the annulus fibrosus, a thick outer ring of tissue much like cartilage. Although the nucleus pulposus is usually soft and spongy in younger people, it tends to dehydrate as people age.

7
LIGAMENTS Ligaments: Are a band of fibrous tissue connecting bones or cartilage. It is instrumental in maintaining cervical spine alignment

8
SPINAL CORD AND NERVES The spinal cord extends from the foramen magnum to the upper lumbar spine (usually L1–L2) and gives rise to 31 pairs of spinal nerves. The eight cervical roots exit through intervertebral foramina, an opening between the vertebrae. The meninges (i.e., dura mater, arachnoid layer, and pia mater) cover the spinal cord. Cerebrospinal fluid bathes the spinal cord and is found in the subarachnoid space
 and gives rise to 31 pairs of spinal nerves. The eight cervical roots exit through intervertebral foramina, an opening between the vertebrae. The meninges (i.e., dura mater, arachnoid layer, and pia mater) cover the spinal cord. Cerebrospinal fluid bathes the. spinal cord and is found in the. subarachnoid space.")
9
NERVE ROOT DISTRIBUTION

10
NERVE ROOT FUNCTION

11
CERVICAL DERMATOME

12
Diagnostic Studies Common diagnostic studies used to evaluate the non-traumatic cervical spine patient: Plain Radiographs Computed Tomography Magnetic Resonance Imaging Bone Scan Myelogram/Postmyelogram CT Electromyography/Nerve Conduction Velocities Somatosensory Evoked Potentials *Neuro Exam compared to diagnostic testing*

13
What is Radiculopathy? Radiculopathy refers to a set of conditions in which one or more nerves is affected and does not work properly (a neuropathy). The emphasis is on the nerve root (radix = "root"). This can result in pain/radicular pain. weakness, numbness, or difficulty controlling specific muscles. The radicular pain that results from a radiculopathy should not be confused with referred pain which is different both in mechanism and clinical features
. This can result in pain/radicular pain. weakness, numbness, or difficulty controlling specific muscles. The radicular pain that results from a radiculopathy should not be confused with referred pain which is different both in mechanism and clinical features.")
14
CERVICAL SPINE DISORDERS
Neck Pain Without Radiculopathy Cervical Radiculopathy: In the cervical spine, the most common cause of radiculopathy is foraminal narrowing and impingement onto the spinal nerve. Cervical Myelopathy: Myelopathy is the result of spinal cord compression, which can stem from clinical entities such as long-standing progressive compression from spondylosis or ossification of the posterior longitudinal ligament. It can also be caused by an acute problem such as acute disc herniation. Myelopathy may be exhibited in a number of ways,

15
CERVICAL SPINE DISORDERS
Intervertebral Disc Herniation—Herniated Nucleus Pulpous

16
CERVICAL SPINE DISORDERS
II. Definitions A. Bulge: Symmetrical extension of the disc beyond the endplates B. Protrusion: Focal area of bulge/disc extension that is still attached to the disc (annulus fibrosis) C. Extruded fragment: Nucleus pulposus no longer connected to the disc D. Sequestered fragment (i.e., free fragment): Nucleus pulposus in the posterior longitudinal ligament E. Radiculopathy: Pain in the distribution of a nerve root resulting from irritation/compression on that nerve root
 C. Extruded fragment: Nucleus pulposus no longer. connected to the disc. D. Sequestered fragment (i.e., free fragment): Nucleus. pulposus in the posterior longitudinal ligament. E. Radiculopathy: Pain in the distribution of a nerve. root resulting from irritation/compression on that. nerve root.")
17
CERVICAL SPINE DISORDERS
Spondylosis Description and Etiology From the Greek word meaning “vertebra,” spondylosis is generally defined as age- and use-related degenerative changes of the spine

18
CERVICAL SPINE DISORDERS
Cervical Spondylotic Myelopathy is defined as “spinal cord dysfunction accompanying typical age-related degeneration of the cervical spine” (Tortolani & Yoon, 2004, p. 701). Spondylosis is the most common etiology, and spondylotic myelopathy is the most common cause of spinal cord dysfunction in persons older than 55 years.
. Spondylosis is the most common etiology, and spondylotic myelopathy is the most common cause of spinal cord dysfunction in persons older than 55 years.")
19
CERVICAL SPINE DISORDERS
Cervical Stenosis Cervical stenosis, classified as either congenital or acquired, is a result of either being born with a narrow spinal canal or developing a narrow spinal canal as a result of degenerative changes.

20
CERVICAL SPINE DISORDERS
Inflamatory: Rheumatoid Arthritis Ankylosing Spondylitis Neoplastic Cervical Spine Disease Metastatic Primary

21
CERVICAL SPINE DISORDERS
Osteoporosis Osteoporosis, the most common metabolic bone disease, is characterized by low bone mass and structural deterioration of bone tissue. Congenital Anomalies Infection

22
Non-Surgical Treatment
Medication Epidural Steroid Injections Physical Therapy Spinal Manipulation (Chiropractic or Osteopathic) Bracing Acupuncture Back School
 Bracing. Acupuncture. Back School.")
23
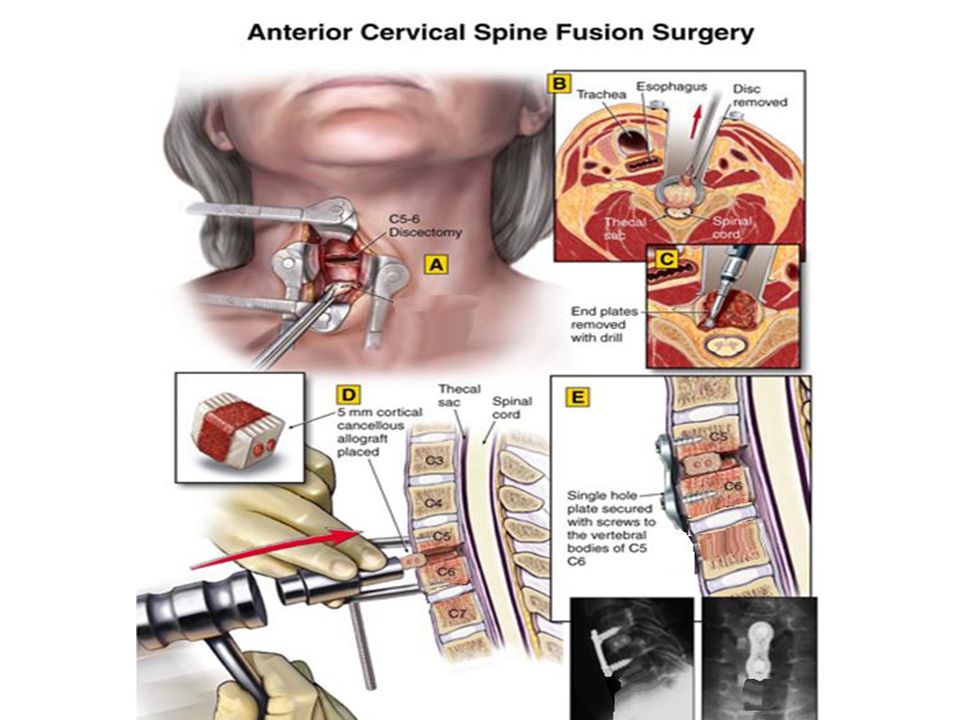
SURGICAL TREATMENT ACDF
Surgical treatment for the patient with a cervical radiculopathy is indicated for patients with (a) persistent signs and symptoms, despite approximately 6 weeks of appropriate nonsurgical treatment or (b) a progressive motor deficit and in whom there is radiographic correlation
 persistent signs and symptoms, despite approximately 6 weeks of appropriate nonsurgical treatment or. (b) a progressive motor deficit and in whom there is radiographic correlation.")
24
SURGICAL TREATMENT ACDF
Cervical Discectomy With and Without Fusion Single/multilevel: The purpose of both anterior cervical discectomy with fusion (ACDF) and without fusion (ACD) is to relieve pressure on the neural elements of the spinal cord and nerve roots More commonly, a fusion is performed utilizing graft material and anterior plate fixation to prevent disc collapse and subsequent kyphosis
 and without fusion (ACD) is to relieve pressure on the neural elements of the spinal cord and nerve roots. More commonly, a fusion is performed utilizing graft material and anterior plate fixation to prevent disc collapse and subsequent kyphosis.")
25
SURGICAL TREATMENT ACDF
Traditionally, an autogenous bone graft is used. This graft typically is harvested from the patient’s iliac crest. Many surgeons now favor the use of interbody fusion devices (e.g., allograft, synthetic spacers, cages)with allograft or other fusion materials. The patient’s length of stay is usually 23 hours or less.
with allograft or other fusion materials. The patient’s length of stay is usually 23 hours or less.")
26
SURGICAL TREATMENT ACDF

29
ACDF Complications Potential Complications–Anterior Cervical Surgery
Complications, although rare, may include nerve root injury (2%–3%), recurrent laryngeal nerve palsy resulting in hoarse voice (2%), spinal cord injury (<1%), esophageal perforation (<1%), or instrumentation failure, including nonunion (<5% for a single level surgery)
, recurrent laryngeal nerve palsy resulting in hoarse voice (2%), spinal cord injury. (<1%), esophageal perforation (<1%), or instrumentation. failure, including nonunion. (<5% for a single level surgery)")
30
POST SURGERY After surgery, pain is managed with narcotic medication. Because narcotic pain pills are addictive, they are used for a limited period (2 to 4 weeks). As their regular use can cause constipation, drink lots of water and eat high fiber foods. Laxatives (e.g., Dulcolax, Senokot, Milk of Magnesia) can be bought without a prescription. Thereafter, pain is managed with acetaminophen (e.g., Tylenol). Hoarseness, sore throat, or difficulty swallowing may occur in some patients and should not be cause for alarm. These symptoms usually resolve in 1 to 4 weeks.
. As their regular use can cause constipation, drink lots of water and eat high fiber foods. Laxatives (e.g., Dulcolax, Senokot, Milk of Magnesia) can be bought without a prescription. Thereafter, pain is managed with acetaminophen (e.g., Tylenol). Hoarseness, sore throat, or difficulty swallowing may occur in some patients and should not be cause for alarm. These symptoms usually resolve in 1 to 4 weeks.")
31
POST SURGERY Activity You may need help with daily activities (e.g., dressing, bathing), but most patients are able to care for themselves right away. Gradually return to your normal activities. Walking is encouraged; start with a short distance and gradually increase to 1 to 2 miles daily. A physical therapy program may be recommended. If applicable, know how to wear a cervical collar before leaving the hospital. Wear it when walking or riding in a car
, but most patients are able to care for themselves right away. Gradually return to your normal activities. Walking is encouraged; start with a short distance and gradually increase to 1 to 2 miles daily. A physical therapy program may be recommended. If applicable, know how to wear a cervical collar before leaving the hospital. Wear it when walking or riding in a car.")
32
POST SURGERY Most Common Restrictions
If you had a fusion, do not use non-steroidal anti-inflammatory drugs (NSAIDs) (e.g., aspirin; ibuprofen, Advil, Motrin, Nuprin; naproxen sodium, Aleve) for 6 months after surgery. NSAIDs may cause bleeding and interfere with bone healing. Do not smoke. Smoking delays healing by increasing the risk of complications (e.g., infection) and inhibits the bones' ability to fuse. Do not drive for 2 to 4 weeks after surgery or until discussed with your surgeon. Avoid sitting for long periods of time. Avoid bending your head forward or backward. Do not lift anything heavier than 5 pounds (e.g., gallon of milk). Housework and yard-work are not permitted until the first follow-up office visit. This includes gardening, mowing, vacuuming, ironing, and loading/unloading the dishwasher, washer, or dryer. Postpone sexual activity until your follow-up appointment unless your surgeon specifies otherwise.
 (e.g., aspirin; ibuprofen, Advil, Motrin, Nuprin; naproxen sodium, Aleve) for 6 months after surgery. NSAIDs may cause bleeding and interfere with bone healing. Do not smoke. Smoking delays healing by increasing the risk of complications (e.g., infection) and inhibits the bones ability to fuse. Do not drive for 2 to 4 weeks after surgery or until discussed with your surgeon. Avoid sitting for long periods of time. Avoid bending your head forward or backward. Do not lift anything heavier than 5 pounds (e.g., gallon of milk). Housework and yard-work are not permitted until the first follow-up office visit. This includes gardening, mowing, vacuuming, ironing, and loading/unloading the dishwasher, washer, or dryer. Postpone sexual activity until your follow-up appointment unless your surgeon specifies otherwise.")
33
ACDF RESULTS What are the results?
Anterior cervical discectomy is successful in relieving arm pain in 92 to 100% of patients [3]. However, arm weakness and numbness may persist for weeks to months. Neck pain is relieved in 73 to 83% of patients [3]. In general, people with arm pain benefit more from ACDF than those with neck pain. Aim to keep a positive attitude and diligently perform your physical therapy exercises.

34
Biblography/ References
AANN Clinical Practice Guideline Series; Cervical Spine; A Guide to Preoperative and Post-Operative Care

Similar presentations