Download presentation
Presentation is loading. Please wait.

1
Patent Ductus Arteriosus in the Preterm Infant (PDA)
Clinical dilemma Burnard ED. The cardiac murmur in relation to symptoms in the newborn. Br Med J. 1939;1:134 Rudolph AM, Drorbaugh JE, Auld PAM, et al. Studies on the circulation in the neonatal period. Pediatrics. 1961;27: 551–556

3
What is PDA?

4
Fetal DA maintain by PGE2 +NO

5
Functional closure Fetal circulation & PDA Patency (PGE2, No ) After Birth INCREASE PaO2 , Cytochrome-P450, inhibits K+) Pulmonary Vascular resistance Circulating PGE2 and Its receptors Bouayad et al, am J physiol Heart Circ 380:2001 Antenatal Steroid Am J Physiol Heart Circ Physiol, Sep 1981; 241: H415 - H420 Vitamin A Wu GR et al, pediat res 49,: ; 2001 ,

6
Anatomical closure & Remodeling
Constrictive effect of O2 Loss of responsiveness to PGE2 Obliteration of vessel lumen Reduction in intramural vasa vasorum blood flow Ductus wall hypoxia lead to reduction PGE2 and NO production (Apoptosis VEGF) Preterm infant fail in this remodeling mechanism Kajino et al, Factors that increase the contractile tone of DA Am j physiol 281 ;2001
 Preterm infant fail in this remodeling mechanism. Kajino et al, Factors that increase the contractile tone of DA Am j physiol 281 ;2001.")
7
Patency of the preterm fetal ductus arteriosus
The preterm DA is morphologically and biochemically immature Edward M 2007 Poorly responsive to contractile stimuli Low oxygen tension Vasodilators ( adenosine, PGE, NO ) The excessive inhibitory effects of endogenous PGE and NO + a weaker intrinsic DA tone With increasing ductal dependency on NO inhibition of prostaglandin production woul;d become less likely to produce ductal constriction Am J Physiol 287: R652–R660, 2004.
 The excessive inhibitory effects of endogenous PGE and NO + a weaker intrinsic DA tone. With increasing ductal dependency on NO inhibition of prostaglandin production woul;d become less likely to produce ductal constriction. Am J Physiol 287: R652–R660,")
8
INCIDENCE (%) 0-24 hours 24-48 hours 48-72 hours 72-96 hours
GEST (WEEK) Healthy RDS >40 55 38-40 85 50 5 34-37 96 42 12 4 30-33 87 31 56 13 25 11 < 29 80 88 40 84 20 77 7 65 Reller et al, J pediatr 122: ; 1993
 Healthy. RDS. > < Reller et al, J pediatr 122: ;")
9
Spontaneous permanent closure of the DA in ELBW neonates
Koch, J. et al. Pediatrics 2006;117:

10
The cumulative permanent closure rate of the DA by serial ECHO in 42 ELBW neonates during the first 10 days postnatally Koch, J. et al. Pediatrics 2006;117:

11
Incidence of PDA in different GA At AFHSR 2006-2007
35/140 29/244 37/1183

12
The usual story PRETERM MALE INFANT WITH HMD
Treated with mechanical ventilation, and SURFACTANT Improved, with lower inspired oxygen requirements and ventilation support Aminophyline started in preparing for extubation 2-3 days, when discussions ensued about EXTUBATION FiO2 requirement and pressure support increased

13
Hemodynamic alteration
Magnitude of L R shunt ( >50% COP) Increase pulmonary venous pressure and Pulmonary congestion Increaser HR and stroke volume Blood flow rearrangement lead to organ hypoperfusion Pulmonary hemorrhage Pediatr Res 35:331A, 1994
 Increase pulmonary venous pressure and Pulmonary congestion. Increaser HR and stroke volume. Blood flow rearrangement lead to organ hypoperfusion. Pulmonary hemorrhage. Pediatr Res 35:331A,")
15
Chest X-ray

16
Course Left-to-right shunting through the ductus.
Increased pulmonary blood flow & pulmonary congestion Hemorrhagic pulmonary Edema Worsening respiratory status with ventilation difficulties surfactant dysfunction Reduced organ perfusion Metabolic Acidosis PDA affects key outcome variables of early preterm life. Lung Biology in health and Disease vol84.,p ,1995

17
Clinical Diagnosis Failure to wean ventilator pressures and O2
Systolic murmur at the left upper sternal edge radiating to the back Increased precardial impulses Widened pulse pressure Prominent or bounding peripheral pulses J Paediatr Child Health. 1994;30:406–411

18
How good is clinical examination at detecting a significant patent ductus arteriosus in preterm neonate ?

19
Is It diagnostic ? Homodynamic significance PDA
Very low sensitivity for diagnosis Most significant PDA did not produce clinical signs. Davis P . Arch Pediatr Adolesc Med. 1995;149:1136–1141

20
Arch. Dis. Child. 2003;88;85-86

21
CLINICAL BOTTOM LINE Clinical evaluation of PDA, either by auscultation or by palpation of pulses, is of limited value Reliance on clinical signs results in a delayed diagnosis of PDA. Doppler flow echocardiography is required to confidently rule in or rule out the diagnosis of PDA. J Perinat Med. 2005;33(2):161-4.
:")
22
Do I need to confirm ? No pediatric cardiologist ! What I will do ?
PDA Do I need to confirm ? No pediatric cardiologist ! What I will do ?

23
Echocardiographic Diagnosis
The consequence is accurate but rarely timely diagnosis Availability of Pediatric cardiologist & ECHO Does this baby have a structurally normal heart? Requires neonatologists to develop the skills to perform the imaging. NeoReviews Vol.5 No.3 March 2004

24
ECHO Anatomy of the Great Vessels Is the Ductus Arteriosus Patent?
Direct Imaging OF DA TURBULENCE IN THE MPA Is the Ductal Shunting Hemodynamically Significant? VOLUME OF DUCTAL SHUNTING (Qp:Qs)
")
25
Echocardiographic tracing with pulsed Doppler of normal pulmonary artery flow, showing systolic forward flow and minimal turbulence in diastole.

26
NeoReviews Vol.5 No.3 March 2004

27
Echocardiographic tracing with pulsed Doppler of bidirectional shunting that can occur as right-sided pressures of the duct increase (before exceeding systemic pressures).
.")
28
Case 1 PRETERM MALE INFANT WITH HMD
Treated with mechanical ventilation, and SURFACTANT Improved, with lower inspired oxygen requirements and ventilation support Aminophyline started in preparing for extubation 2-3 days, when discussions ensued about EXTUBATION FiO2 requirement and pressure support increased

29
Case 2 Female, Preterm infant 850gm
HMD, Received one dose of surfactant Extubated To nasal CPAP with FiO after aminophylin loading and maintained N. Gastric Feeding initiated Third day a loud systolic murmur heard with widing pulse pressure ABG Norma, maintain normal hemodynamic status

30
Do I confirm The diagnosis?
PDA Do I confirm The diagnosis? Shall I treat? Which one I will treat? How I will treat?

31
Conservative treatment for patent ductus arteriosus in the preterm
It is important to make distinguish between a clinically significant and non-significant PDA Fluid restriction (maximum 130 ml/kg a day beyond day 3 Adjustment of ventilation by lowering inspiratory time to as low as 0.35 s, and giving higher PEEP Arch Dis Child Fetal Neonatal Ed 2007;92:F244–F247.

32
Occurrence of patent ductus arteriosus (PDA) in 109
conservatively managed preterm neonates (30 weeks’ gestation, requiring ventilation and surfactant treatment (retrospective analysis). Arch. Dis. Child. Fetal Neonatal Ed. 2007;92; ;
. Arch. Dis. Child. Fetal Neonatal Ed. 2007;92; ;")
34
Conclusion: The managed care plan resulted in an overall ductal closure rate of 100%. These results suggest that conservative treatment of PDA is a worthy alternative to medical treatment.

36
Impact of patent ductus arteriosus cerebral oxygenation in preterm infants.
A hemodynamically significant patent ductus arteriosus has a negative effect on cerebral oxygenation in the premature infant. Subsequent and adequate treatment of a PDA may prevent diminished cerebral perfusion and reduces the change of damage to the vulnerable immature brain. PEDIATRICS Vol. 121 No. 1 January 2008, pp

37
Markers may identify preterm with PDA at high risk
It is difficult to predict which infants with a PDA go on to develop major complications Conventional echocardiographic markers applied at 48 hours of life do not predict outcome Serum cardiac Troponin T (cTnT) B-type natriuretic peptide (BNP) NTpBNP and cTnT in conjunction with echocardiography may provide a basis for trials of targeted medical treatment in infants with a PDA. Arch. Dis. Child. Fetal Neonatal Ed. published online 19 Feb 2008;
 B-type natriuretic peptide (BNP) NTpBNP and cTnT in conjunction with echocardiography may provide a basis for trials of targeted medical treatment in infants with a PDA. Arch. Dis. Child. Fetal Neonatal Ed. published online 19 Feb 2008;")
38
Shall I treat? Yes

39
Treatment PGE2 appears to be the most important factor regulating ductal patency Inhibition of PG synthesis by inhibition of the enzyme cyclooxygenase (COX) produces constriction of the DA
 produces constriction of the DA.")
40
Indomethacin Over the years, therapy with indomethacin has been accepted as effective in mediating ductal closure in preterm neonates. Little consensus regarding proper dosage, treatment duration, and optimal timing of treatment. NeoReviews Vol.4 No.8 August 2003 e215

41
Indomethacin Dose & Timing
The response of the ductus to indomethacin depends on the size of the dose and the number of doses administered. 3 doses regimen Vs 5-6 doses (at 0 hours, 12 hours, 24 hours, 48 hours, and 72 hours). Continuous infusion (17 mcg/kg per hour over 36 h)
. Continuous infusion (17 mcg/kg per hour over 36 h)")
42
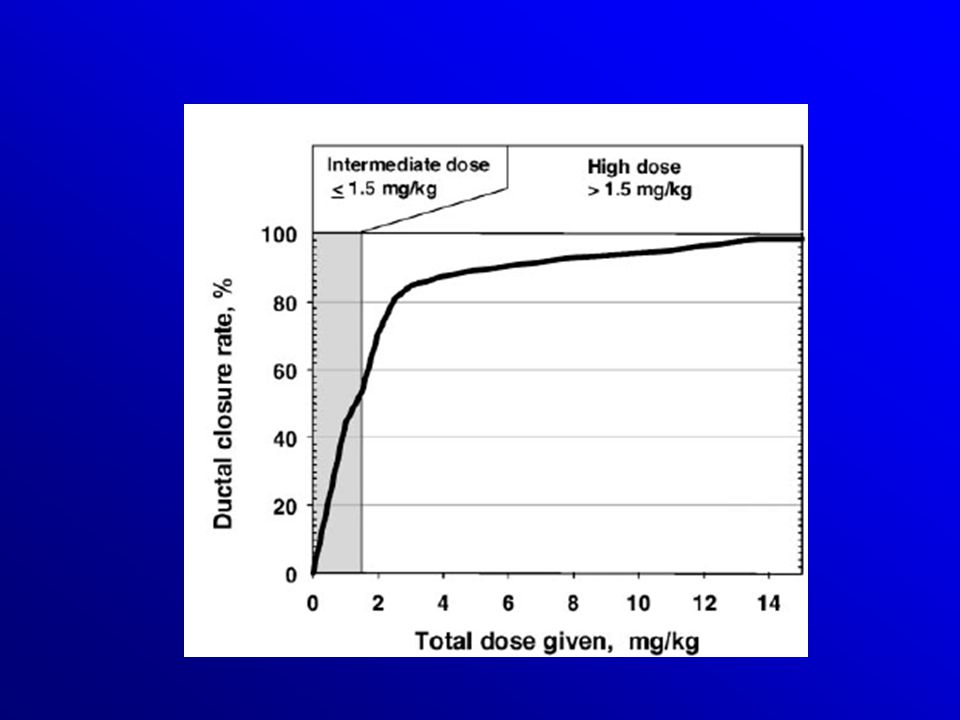
Indomethacin Treatment for Symptomatic Patent Ductus Arteriosus in
Effectiveness and Side Effects of an Escalating, Stepwise Approach to Premature Infants Below 33 Weeks of Gestation Pediatrics 2005;116;

44
Conclusions. High-dose indomethacin after intermediate- dose therapy resulted in an overall closure rate of 98.5% Pediatrics 2005;116;

47
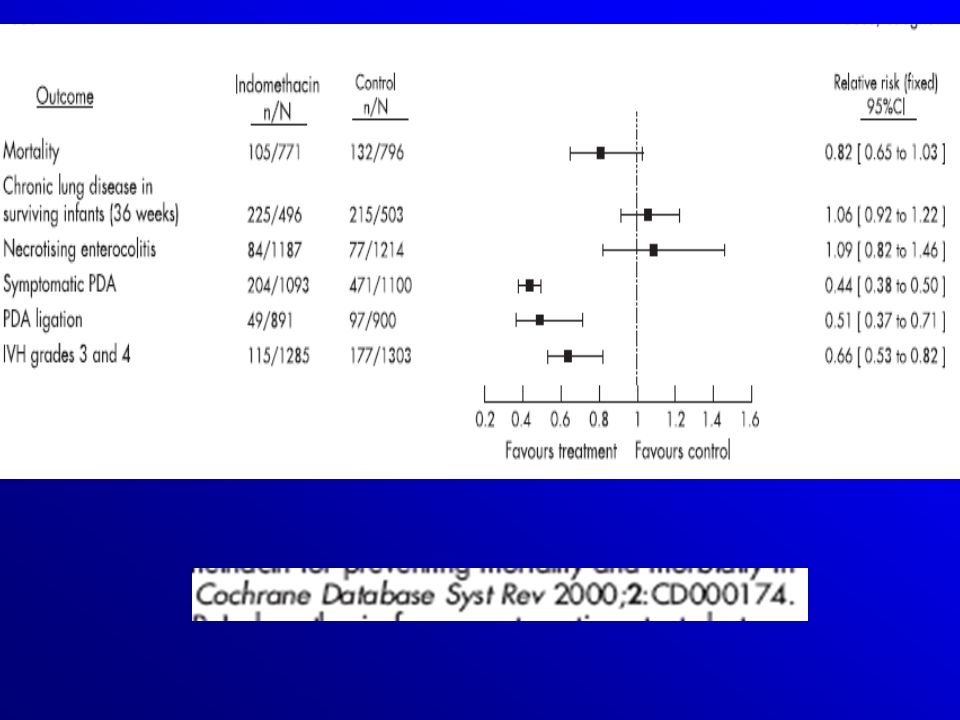
Authors’ conclusions Prolonged indomethacin course does not appear to have a significant effect on improving important outcomes, such as PDA treatment failure, CLD, IVH, or mortality. The reduction of transient renal impairment does not outweigh the increased risk of NEC associated with the prolonged course.

48
Timing Post-natal age Near term infant PGE2 is not the dominant factor maintain ductus patency CottonBiol Neonate 60: ,1991 Reopening of the duct 23% in <26wks Early prophylaxis (90% borne <30 wk with NO PDA only 40% will develop significant PDA)
")
51
Complications of Indomethacin
Decrease in glomerular filtration rate Inhibits platelets and prolongs the bleeding time Frank renal or gastrointestinal bleeding are contraindications to the use of indomethacin. Isolated cases of localized intestinal perforation & NEC ? Sepsis NeoReviews Vol.4 No.8 August 2003

52
Ibuprofen It is emerging rapidly as a potential alternative to indomethacin Causing less vascular compromise Mesenteric blood flow Renal perfusion. CBF

53
Safety and efficacy of ibuprofen
Ibuprofen is as effective as indometacin for PDA treatment in extremely premature infants No increasing in the incidence of complications NEC, CLD Fewer doses of drugs were needed to achieve acceptable closing rates. Arch Dis Child Fetal Neonatal Ed 2008;93:F94–F99. doi: /adc

56
Conclusion No statistically significant difference in the effectiveness of ibuprofen compared to indomethacin in closing the PDA. Ibuprofen reduces the risk of oliguria. ibuprofen may increase the risk for CLD, and pulmonary hypertension Indomethacin should remain the drug of choice for the treatment of a PDA. The Cochrane Collaboration 2007.

57
EBM Wyllie J. Treatment of patent ductus arteriosus. Semin Neonatol2003;8: Thomas RL, Parker GC, Van Overmeire B, et al. A meta-analysis of ibuprofen versus indomethacin for closure of patent ductus arteriosus. Eur J Pediatr2005;164: Shah SS, Ohlsson A. Ibuprofen for the prevention of patent ductus arteriosus in preterm and/or low birth weight infants [Cochrane Review]. In: The Cochrane Library; Issue 2, Oxford: Update Software. Gournay V, Roze JC, Kuster A, et al. Prophylactic ibuprofen versus placebo in very premature infants: a randomised, double-blind, placebo-controlled trial. Lancet 2004;364: Van Overmeire B, Allegaert K, Casaer A, et al.; Multicentre Ibuprofen Prophylaxis Study (MIPS) Investigators. Prophylactic ibuprofen in premature infants: a multicentre, randomised, double-blind, placebo-controlled trial. Lancet2004;364: Van Overmeire B, Smets K, Lecoutere D, et al. A comparison of ibuprofen and indomethacin for closure of patent ductus arteriosus. N Engl J Med2000;343: Gournay V, Savagner C, Thiriez G, et al. Pulmonary hypertension after ibuprofen prophylaxis in very preterm infants. Lancet2002;359:
 Investigators. Prophylactic ibuprofen in premature infants: a multicentre, randomised, double-blind, placebo-controlled trial. Lancet2004;364: Van Overmeire B, Smets K, Lecoutere D, et al. A comparison of ibuprofen and indomethacin for closure of patent ductus arteriosus. N Engl J Med2000;343: Gournay V, Savagner C, Thiriez G, et al. Pulmonary hypertension after ibuprofen prophylaxis in very preterm infants. Lancet2002;359:")
58
Undesirable adverse effect
Increased vascular resistant Increase the free fraction of bilirubin by a factor of four & the risk of bilirubin encephalopathy BPD and PPHN Speziale MV, Allen RG, Henderson CR, Barrington KJ, Finer NN. Effects of ibuprofen and indomethacin on the regional circulation in newborn piglets. Biol Neonate. 1999;76:242–252

59
Concurrent Use of Furosemide
It increases PG production It could decrease ductal response to indomethacin. Consequently, furosemide may have conflicting physiologic effects in the preterm infant who has PDA Used only with signs of congestive HF and pulmonary congestion not with fluid restriction and indomethacin or Ibu. Cochrane review 2004

60
Surgical Closure It is usually reserved for PDA refractory to medical management Proposed as a primary treatment of PDA and the treatment of PDA that responds poorly to indometacin Little DC, Pratt TC, Blalock SE, et al. Patent ductus arteriosus in micropreemies and full-term infants: the relative merits of surgical ligation versus indometacin treatment. J Pediatr Surg 2003;38:492–6.

62
AFHSR 17/35 12/35 6/45

63
Complication And Mortality AFHSR 2006-2007

64
Future Directions NO Inhibition PGE2 Receptor Manipulation Vitamin A
Other COX Inhibitors Less effective

65
Summary PDA is a common complication of very low-birthweight infants who is recovering from RDS Early diagnosis (ECHO)and treatment of homodynamic significant duct prevent major morbidity Conservative treatment is visible Either indo. Or IBU you need the duct closed with out the hand of surgeons
and treatment of homodynamic significant duct prevent major morbidity. Conservative treatment is visible. Either indo. Or IBU you need the duct closed with out the hand of surgeons.")
66
Thanks

Similar presentations


























 Respiratory Distress Syndrome.>")


