Download presentation
Presentation is loading. Please wait.

1
Volume Optimization in Surgical Patients Philippe Van der Linden MD, PhD CHU Brugmann-HUDERF, Free University of Brussels

2
Intraoperative Fluid Management and Outcome Randomized controlled study Elective abdominal surgery (N=152) Intraoperative fluid regimen: - Restrictive: 4 ml/kg.h - Liberal: 10 ml/kg + 12 ml/kg.h Strict algorithm for additional intraoperative fluids Fewer complications in the restrictive group (13vs23: p=0.046) Passed fecesHospital LOS 0 4 8 12 16 20 24 Days Restrictive (N=77)Liberal (N=75) p< 0.001 p< 0.01 From Nisanevich V et al. Anesthesiology 103:25-32, 2005.

5
Perioperative Fluid Strategy In many cases, fluids are administered without adequate monitoring to guide volume This may result in adverse outcomes relating to either inadequate or excess fluid administration

6
Complications associated with fluid therapy: 17% Fluid overload: 7% Hypovolemia: 11%

7
Perioperative Fluid Strategy Excessive fluid administration: Increased demand on cardiac function Increased risk of respiratory failure and pneumonia Inhibition of gastro-intestinal motility Decreased tissue oxygenation with delayed wound healing Increased risk of urinary retention Coagulation disturbances

8
Perioperative Fluid Strategy Inadequate fluid administration: Reduced effective circulating volume Diversion of blood toward vital organs Under-perfusion of « non vital » organs: gut, kidneys, skin Activation of the sympathetic nervous and renine angiotensin systems Increased inflammatory response

9
Perioperative Fluid Strategy

10
Volume « optimization » will depend: Type of surgery Importance of the surgical insult Patient’s clinical conditions Cardiorespiratory reserve Medical treatment Preoperative volume status Preoperative preparation

11
Volume «Optimization » in Surgical Patients Avoidance of dehydration Maintenance of an « effective » circulating blood volume Prevention of « inadequate » tissue perfusion

12
Fluid Administration Strategies The « recipe » book approach From Grocott MPW et al. Anesth Analg 100:1093-106, 2005.

13
Peroperative Fluid Management: « The cook book approach »

14
Fluid Administration Strategies The « recipe » book approach Intravascular pressure measurements From Grocott MPW et al. Anesth Analg 100:1093-106, 2005.

15
Fluid Administration Strategies The « recipe » book approach Intravascular pressure measurement Systolic and pulse pressure variation From Grocott MPW et al. Anesth Analg 100:1093-106, 2005.

16
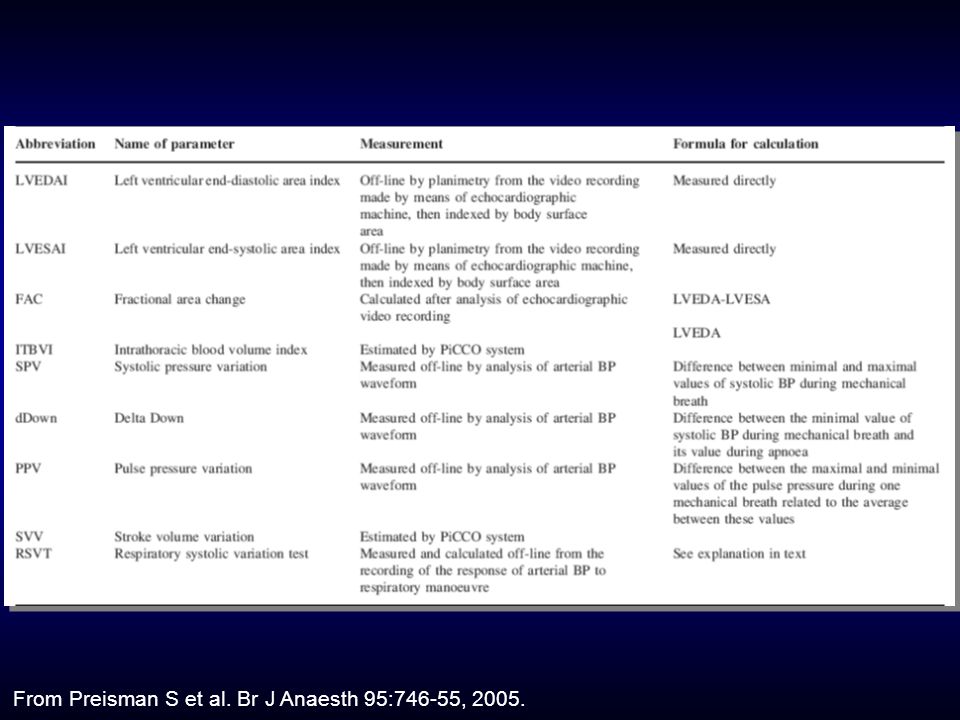
Systolic and Pulse Pressure Variations Observation of systolic and pulse pressure variation in relation to variations of intrathoracic pressure resulting from mechanical ventilation

17
From Preisman S et al. Br J Anaesth 95:746-55, 2005.

21
Fluid Administration Strategies The « recipe » book approach Intravascular pressure measurement Systolic and pulse pressure variation « Fluid » challenge Intravascular pressure measurement Blood flow measurement From Grocott MPW et al. Anesth Analg 100:1093-106, 2005.

22
Fluid Challenge and Intravascular Pressure Measurement Observation of the cardiac filling pressures (CVP and/or PAOP) response to a « fluid challenge » (fixed volume of colloid infused over 10 to 15 min)
 response to a « fluid challenge » (fixed volume of colloid infused over 10 to 15 min)")
23
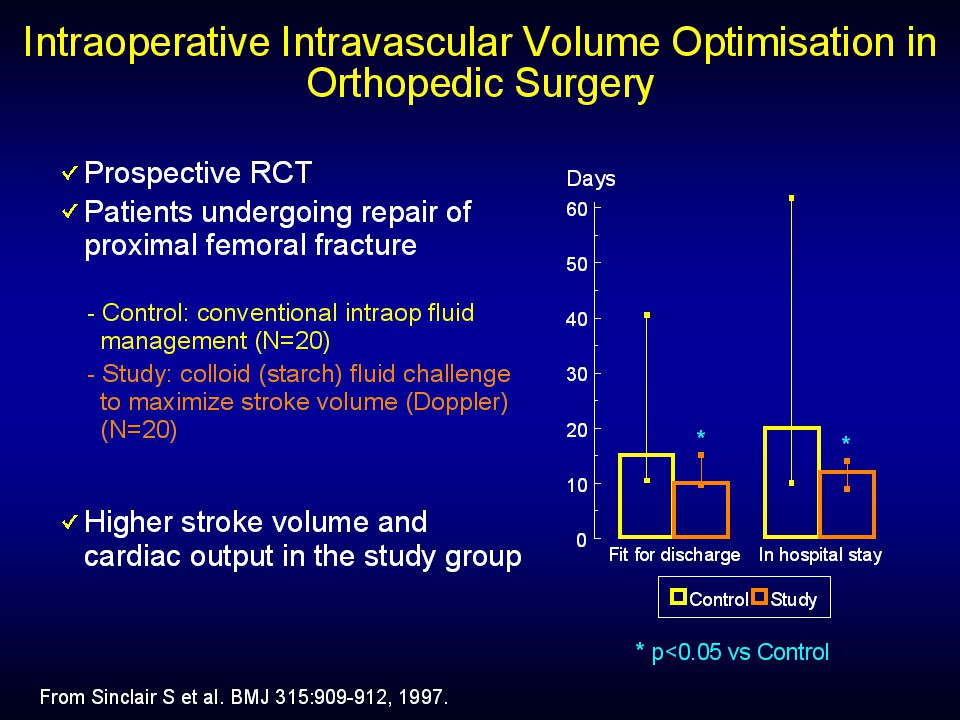
Intraoperative Intravascular Volume Optimisation in Orthopedic Surgery Prospective RCT Elderly patients undergoing repair of proximal femoral fracture - Control: conventional intraop fluid management (N=29) - Protocol 1: colloid (4% MF gelatin) fluid challenge guided by CVP (N=31) - Protocol 2: colloid (4% MF gelatin) fluid challenge guided by Doppler (N=30) Fit for discharge 0 5 10 15 20 Days ControlProtocol 1Protocol 2 From Venn R et al. Br J Anaesth 88:65-71, 2002. * * p<0.05 vs Control * Fewer patients in the protocol groups experienced severe intraoperative hypotension

24
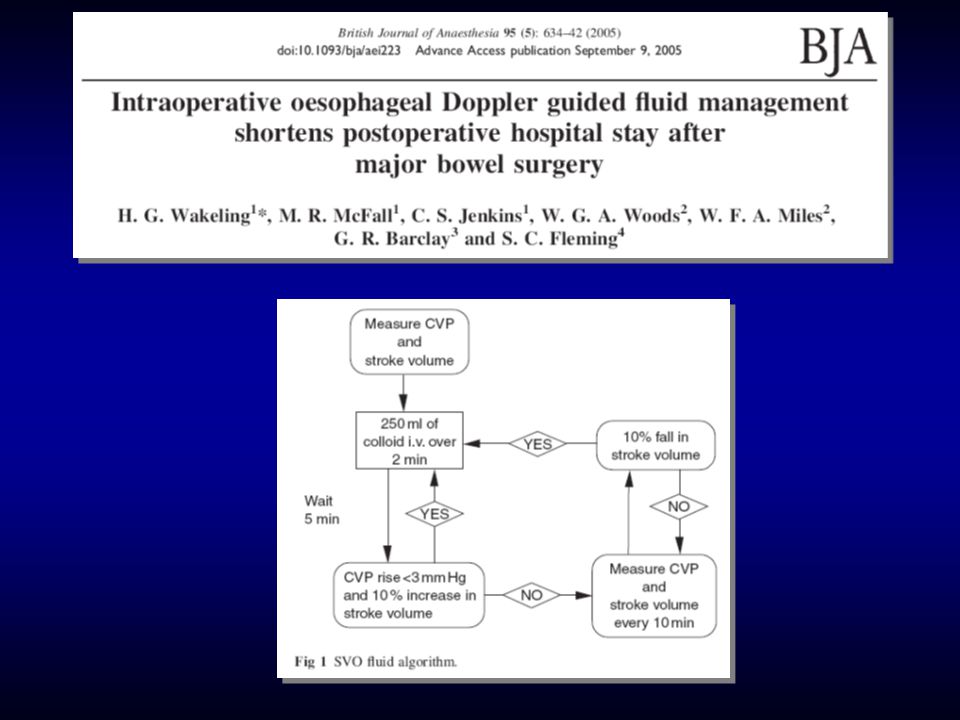
Fluid Challenge and Measurement of Blood Flow Observation of the blood flow (cardiac output or stroke volume) response to a « fluid challenge » (fixed volume of colloid infused over 10 to 15 min)
 response to a « fluid challenge » (fixed volume of colloid infused over 10 to 15 min)")
27
Perioperative Fluid Administration: The Goal-Directed Approach Medline search from 1996 to 2006 Nine studies Hospital stay (7 studies) Postoperative complications (4 studies) PONV and ileus (3 studies) Only oesophageal Doppler has been tested adequately From Bundgaard-Nielsen M et al. Acta Anaesthesiol Scand 51:331-340, 2007.

28
Perioperative Fluid Administration: The Goal-Directed Approach From Bundgaard-Nielsen M et al. Acta Anaesthesiol Scand 51:331-340, 2007.

29
Peroperative Fluid Management: « The Goal-Directed Therapy »

32
Fluid Administration Strategies The « recipe » book approach Intravascular pressure measurement Systolic and pulse pressure variation « Fluid » challenge Intravascular pressure measurement Blood flow measurement Measurement of tissue perfusion From Grocott MPW et al. Anesth Analg 100:1093-106, 2005.

33
Measurement of Tissue Perfusion Gastrointestinal tonometry Laser doppler flowmetry Near-infrared spectroscopy Transcutaneous O2 measurements Tissue pH monitors…

34
Preoperative Goal-Directed Fluid Optimization Observational study (N=12) Preoperative maximization of stroke volume using oesophageal doppler (OD) Comparison of the findings with: Modelflow determined stroke volume Oesophageal doppler estimated corrected flow time (FTc) Central venous oxygen saturation (SvO2) Muscle and brain oxygenation (NIRS) From Bundgaard-Nielsen M et al; Br J Anaesth 98:38-44, 2007.
 Preoperative maximization of stroke volume using oesophageal doppler (OD) Comparison of the findings with: Modelflow determined stroke volume Oesophageal doppler estimated corrected flow time (FTc) Central venous oxygen saturation (SvO2) Muscle and brain oxygenation (NIRS) From Bundgaard-Nielsen M et al; Br J Anaesth 98:38-44, 2007.")
35
Preoperative Goal-Directed Fluid Optimization

36
From Bundgaard-Nielsen M et al; Br J Anaesth 98:38-44, 2007.

37
Preoperative Goal-Directed Fluid Optimization From Bundgaard-Nielsen M et al; Br J Anaesth 98:38-44, 2007.

38
Preoperative Goal-Directed Fluid Optimization Based on OD assessment, optimization of stroke volume was achieved after the administration of 400- 800 ml of colloid. The hypothetical volumes administered for optimization based upon Modelflow and SvO2 differed from OD in 10 and 11 patients respectively Changes in FTc and NIRS were inconsistent with OD guided optimization From Bundgaard-Nielsen M et al; Br J Anaesth 98:38-44, 2007.

39
Peroperative Fluid Management

40
The Wet vs Dry Philosophy « Most of the dry-supporting studies used fixed amounts of volume instead of a fluid concept adapted to the patient need (« goal-directed ») » From Boldt J. Eur J Anaesthesiol 23:631-640, 2006.

43
Perioperative Fluid Management Accurate dosing of fluid therapy Accurate choice between the various available IV fluids

44
COLLOIDS Pro Volume effect Con Secondary effects Cost

46
Critical Appraisal of Meta-Analyses Possible selection bias of included trials Results of analysis may be similar......but interpretation can be quite different Specific objections to meta-analyses on volume therapy: Mixing of patients with different diseases Different kinds of infused fluids Old studies (more than 15 years) included Mortality used as the endpoint in the meta-analyses...... but not in most of the volume replacement studies From Boldt J. Can J Anesth 51:500-513, 2004.

49
Volume «Optimization » in Surgical Patients Choice between the different solutions Physiological compartment that needs to be restored (intravascular, interstitial, intracellular) Characteristics of the solutions Pharmacokinetic and pharmacodynamic properties Side effects Costs
 Characteristics of the solutions Pharmacokinetic and pharmacodynamic properties Side effects Costs")
50
Perioperative Fluid Strategy Conclusions (1) Preoperative fluid deficit must be compensated Replace water losses by crystalloids and plasma losses by synthetic colloids Hartmann or Plasmalyte instead of NaCl 0.9% Neurosurgery: avoid hypotonic solutions Fluid strategy must be goal-oriented and adapted: To the patient To the surgical procedure
 Preoperative fluid deficit must be compensated Replace water losses by crystalloids and plasma losses by synthetic colloids Hartmann or Plasmalyte instead of NaCl 0.9% Neurosurgery: avoid hypotonic solutions Fluid strategy must be goal-oriented and adapted: To the patient To the surgical procedure")
51
Type of fluids does not influence outcome Type of fluids does not influence outcome

52
Goal-directed fluid optimization improves outcome Goal-directed fluid optimization improves outcome

53
Some types of fluids allow more efficient goal-directed fluid optimization Some types of fluids allow more efficient goal-directed fluid optimization

54
Thank you for your attention ?

58
From Bundgaard-Nielsen M et al; Br J Anaesth 98:38-44, 2007.

Similar presentations














>")











 1. Mass Balance>")





 4(d² + 4) 3rs(2r – s) 15cd(1 + 2cd) 8(4a² + 3b²)>")
