Download presentation
Presentation is loading. Please wait.

1
How to Navigate the New Oral Anticoagulants and Deal With Triple Therapy Dr. Morteza Safi Professor of interventional cardiology Cardiovascular Research Center, Modarres hospital, Shahid Beheshti University of medical sciences, Tehran, Iran.

2
In 2010, it was estimated that AF affected 5.2 million Americans, and this number is projected to increase to 12.1 million by 2030

3
With more than 80% of these patients having an indication for oral anticoagulation, and approximately 35% of these patients having coronary artery disease

5
Question Is The Treatment Of Atrial Fibrillation And The Stented ACS Patient The Same?

6
The Optimal Management of Atrial Fibrillation and ACS Differ Atrial Fibrillation (ACTIVE W): The combination of aspirin and clopidogrel is not as effective as warfarin in patients with AF However Stenting (STARS): The combination of aspirin and clopidogrel is more effective than warfarin in patients with coronary stents
: The combination of aspirin and clopidogrel is not as effective as warfarin in patients with AF However Stenting (STARS): The combination of aspirin and clopidogrel is more effective than warfarin in patients with coronary stents")
19
APPRAISE2 Trial Stopped Prematurely On November 15, 2010 the Data Monitoring Committee recommended that the trial be stopped after enrollment of 7,048 pts with median follow-up 3.5 months due to an excess of clinically important bleeding in the apixaban arm without a counterbalancing reduction in ischemic events

20
Rivaroxaban in patients with recent Acute Coronary Syndrome

25
Pimary PCI In patients on NOAC Should additional peri-procedural anticoagulation be used?

26
In patients on warfarin with INR in the therapeutic range (2.0-3.0), PCI appears to be safe without the need for additional peri-procedural anticoagulation Karjalainen PP, et al Eur Heart J. 2008;29

27
All currently available NOACs reach a peak plasma level within one to four hours after ingestion, and reach the trough level between 12-24 hours In patients presenting with STEMI who have taken a NOAC within four hours of presentation, the risk of bleeding when giving additional anticoagulants or antiplatelet agents is at least theoretically higher than those who have taken the last dose of NOAC >12 hours before STEMI presentation

28
In a small randomized study involving 50 patients on dual antiplatelet therapy (DAPT) undergoing elective PCI, use of peri-procedural dabigatran did not provide sufficient anticoagulation during PCI Vranckx P, et al. EuroIntervention. 2013;8:1052-60

29
The X-PLORER trial In a small study, peri-procedural rivaroxaban given two to four hours prior to elective PCI appeared to provide adequate anticoagulation without increased risk of bleeding Vranckx P, et al. The X-PLORER trial. Thromb Haemost. 2015;114:258-67

30
Until there are larger studies proving the safety and efficacy of performing PCI on NOACs without additional anticoagulation, it is recommended to give additional heparin or bivalirudin (and avoid glycoprotein [GP] IIb/IIIa inhibitors) regardless of the last NOAC dose
![Until there are larger studies proving the safety and efficacy of performing PCI on NOACs without additional anticoagulation, it is recommended to give additional heparin or bivalirudin (and avoid glycoprotein [GP] IIb/IIIa inhibitors) regardless of the last NOAC dose](http://images.slideplayer.com/47/11750076/slides/slide_30.jpg "Until there are larger studies proving the safety and efficacy of performing PCI on NOACs without additional anticoagulation, it is recommended to give additional heparin or bivalirudin (and avoid glycoprotein [GP] IIb/IIIa inhibitors) regardless of the last NOAC dose")
31
If using heparin as the additional peri- procedural anticoagulant, the routine target ACT level (250-300s) can be used for heparin titration, even in patients who are taking NOACs
 can be used for heparin titration, even in patients who are taking NOACs")
32
Radial Access MATRIX trial In a recent multicenter randomized study of 8404 patients radial compared to femoral access in patients with ACS was shown to reduce the net adverse clinical events through a reduction in major bleeding and all-cause mortality

33
Acute and Long-term Antiplatelet Agents

34
Though the current practice is highly variable in terms of the initial P2Y 12 inhibitor used, in patients taking NOACs, a loading dose of clopidogrel (600 mg) is preferable compared to the newer antiplatelet agents given the lower risk of bleeding associated with clopidogrel.
 is preferable compared to the newer antiplatelet agents given the lower risk of bleeding associated with clopidogrel.")
35
Long-term antiplatelet and anticoagulation regimen

44
North American Consensus Statement Regarding Antithrombotic Therapy in Atrial Fibrillation Requiring a Stent Low dose aspirin (<100 mg per day) Clopidogrel is preferred in combination with aspirin and warfarin Prasugrel and ticagrelor cannot be recommended Warfarin dose adjusted INR between 2 and 2.5 Not unreasonable to use dabigatran in place of warfarin based on the PETRO trial (dabigatran50, 150, 300 mg BID with or without aspirin vs warfarin)
 Clopidogrel is preferred in combination with aspirin and warfarin Prasugrel and ticagrelor cannot be recommended Warfarin dose adjusted INR between 2 and 2.5 Not unreasonable to use dabigatran in place of warfarin based on the PETRO trial (dabigatran50, 150, 300 mg BID with or without aspirin vs warfarin)")
45
However, until more data are available, some experts advocate use of triple therapy with warfarin (INR 2.0-2.5) rather than NOACs for the shortest duration possible, depending on the type of stent and individual bleeding risk.
 rather than NOACs for the shortest duration possible, depending on the type of stent and individual bleeding risk.")
46
(EHRA) guideline The latest updated European Heart Rhythm Association (EHRA) guidelines on use of NOACs recommend restarting the same NOAC in combination with SAPT or DAPT after discontinuation of parenteral anticoagulation in patients with ACS, based on expert opinion rather than currently available evidence
 guideline The latest updated European Heart Rhythm Association (EHRA) guidelines on use of NOACs recommend restarting the same NOAC in combination with SAPT or DAPT after discontinuation of parenteral anticoagulation in patients with ACS, based on expert opinion rather than currently available evidence")
47
(EHRA) guideline It is recommended to reduce the doses of NOACs when combining with DAPT Dabigatran 110 mg twice-daily Apixaban 2.5 mg twice-daily Rivaroxaban 15 mg once-daily Edoxaban 30 mg once-daily
 guideline It is recommended to reduce the doses of NOACs when combining with DAPT Dabigatran 110 mg twice-daily Apixaban 2.5 mg twice-daily Rivaroxaban 15 mg once-daily Edoxaban 30 mg once-daily")
48
Until further data are available, the experts recommend use of radial access, loading dose of aspirin and clopidogrel, and additional peri- procedural anticoagulation with heparin or bivalirudin in the acute setting for these patients. Post-ACS, for patients at high risk of embolic events, triple therapy (DAPT plus warfarin or reduced-dose of NOAC) is recommended for as short a duration as possible.
 is recommended for as short a duration as possible..")
58
Triple Therapy Summary and Synthesis of Guideline, Expert Consensus Documents, and Comprehensive Review Article Recommendations on the Management of Patients Treated With Triple Therapy Assess ischemic and bleeding risks using validated risk predictors (e.g., CHA2DS2-VASc, HAS-BLED) Keep triple therapy duration as short as possible; dual therapy only (oral anticoagulant and clopidogrel) may be considered in select patients Consider target INR 2.0–2.5 when warfarin is used Clopidogrel is the P2Y12inhibitor of choice Use low dose (≤100 mg daily) aspirin PPI Rx should be used in patients with a history of GI bleeding and are reasonable to use in patients with increased risk of GI bleeding
 Keep triple therapy duration as short as possible; dual therapy only (oral anticoagulant and clopidogrel) may be considered in select patients Consider target INR 2.0–2.5 when warfarin is used Clopidogrel is the P2Y12inhibitor of choice Use low dose (≤100 mg daily) aspirin PPI Rx should be used in patients with a history of GI bleeding and are reasonable to use in patients with increased risk of GI bleeding")
59
Thanks for your attention

61
The WOEST Trial: First Randomized Trial Comparing Two Regimens With and Without Aspirin in Patients on Oral Anticoagulant Therapy Undergoing Coronary Stenting

68
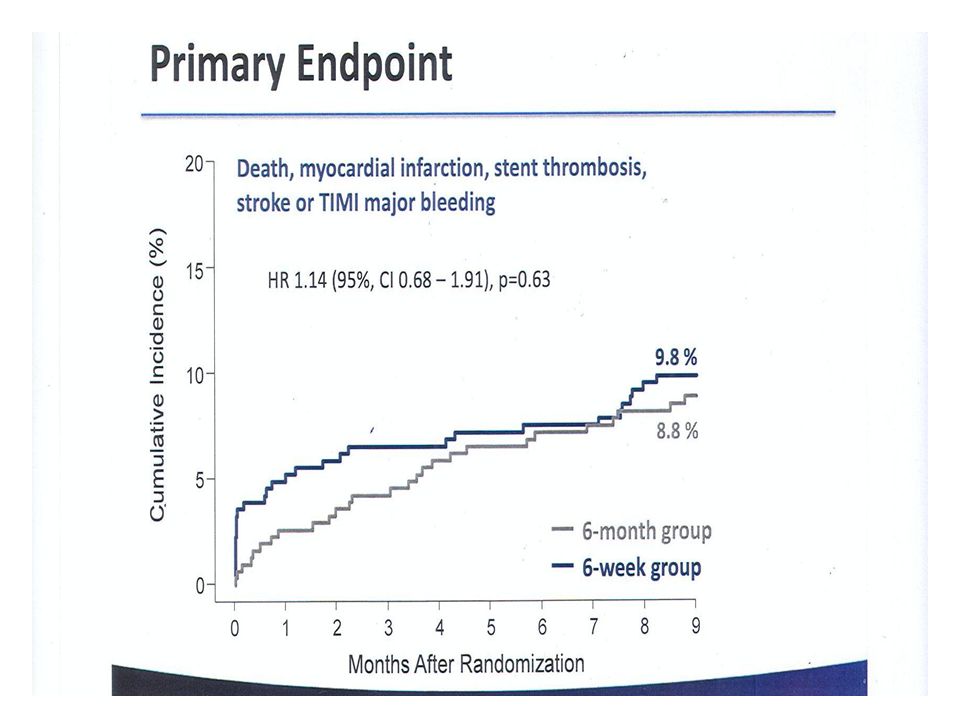
Dual vs. Triple Antiplatelet Therapy Prospective Studies ISAR–Triple Trial: 6 months vs 6 weeks of clopidogrel after DES in patients on aspirin and warfarin WOEST (What is the Optimal antiplatElet and anticoagulant in patients with oral anticoagulants and StenTing study): warfarin + clopidogrel 75 mg/day vs warfarin + clopidogrel + aspirin (80 mg/day)
: warfarin + clopidogrel 75 mg/day vs warfarin + clopidogrel + aspirin (80 mg/day).")
69
Patient with chronic atrial fibrillation who needs DAPT for DES

73
Recommendations for Patients with AF Undergoing Stenting Assess the risk for stent thrombosis, ischemic events, and thromboembolism, and adjust the need or degree of anticoagulation to the risk

Similar presentations























































 Presented.>")


 Secondary objective: Death, MI, stroke, stent thrombosis Randomize.>")

