Download presentation
Presentation is loading. Please wait.

2
BREAST DISEASE Pt 1 PresenterAishaAmin

5
Benign Breast Disease

6
WHAT IS IT

7
Benign breast lesion is a non-cancerous lesion. According to American Cancer society, when tissue biopsy is examined under the microscope, nine out of every 10 women will have some type of abnormality The goal is to exclude cancer Davis HH, Simons M, Davis JB. Cystic disease of the breast: relationship to carcinoma. Cancer 1964;17:957-78

8
Epidemiology from 2011-2012 The most prevalent benign breast diseases are fibrocystic and dominant lumps. Dominant lumps are defined as lesions that are distinct, unchanging, and persistent, for example: galactocele, fibroadenomas and gross cysts.

9
BENIGN VS MALIGNANT

10
BENIGN (80%)
")
11
ANDI CLASSIFICATION FIBROCYSTIC CHANGE IS NOT DISEASE CLINICAL CLASSIFICATION

12
ANDI CLASSIFICATION OF BBB 1) DISORDERS OF DEVELOPMENT 2) DISORDERS OF CYCLICAL CHANGE 3)DISORDERS OF INVOLUTION
 DISORDERS OF DEVELOPMENT 2) DISORDERS OF CYCLICAL CHANGE 3)DISORDERS OF INVOLUTION")
13
Classification based on Clinical Features Physiological swelling and tenderness – Nodularity – Mastalgia – Dominant lumps (macrocysts, galactocoeles & fibroadenoma) Nipple discharge – Galactorea – Abnormal nipple discharge
 Nipple discharge – Galactorea – Abnormal nipple discharge")
14
Breast infections – Intrinsic mastitis 1. Postpartum engorgement 2. Lactational mastitis 3. Lactational breast abscess 4.Chronic recurrent subareolar abscess 5. Acute mastitis associated with macrocystic breasts – Extrinsic infections

15
1) DISORDERS OF DEVELOPMENT Polymazia & Polythelia Amazia Congenital inversion of nipples Macromastia Mastitis of infants Adolescent hypertrophy - gross stromal hyperplasia at time of development, of unknown origin
 DISORDERS OF DEVELOPMENT Polymazia & Polythelia Amazia Congenital inversion of nipples Macromastia Mastitis of infants Adolescent hypertrophy - gross stromal hyperplasia at time of development, of unknown origin")
17
Disorders of Cyclical Change Mastalgia and nodularity

18
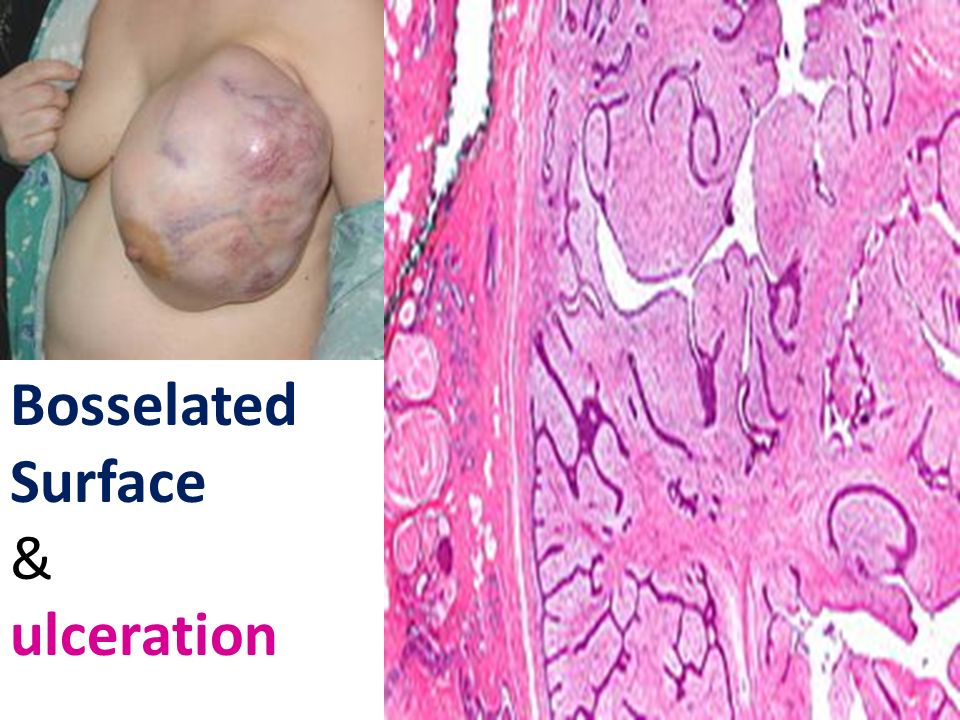
Disorders of Involution Fibrocystic breast disease Fibrocystic changes: – Cysts – Fibrosis – Sclerosing adenosis – Duct ectasia with periductal mastitis Fibroadenoma Phylloides

20
Bosselated Surface & ulceration

21
30 year old female presents to the OPD with a tender swelling on her left breast. The surrounding area is also red, swollen, and tender to touch. There is nipple retraction on the other breast. Excision of the area reveals brownish discharge. What is your diagnosis? What is the next best appropriate step? How would you proceed to manage this patient?

22
Duct ectasia/ Periductal mastitis Dilation of the breast ducts -> periductal inflammation -> the larger lactiferous ducts fill with a brown or green secretion -> may discharge. There maybe an abscess or a visible lump There may be fistula formation Fibrosis may eventually develop -> nipple retraction. Maybe associated with smoking?

23
Treatment: flucloxacillin & metronidazole. Surgery maybe needed: involves the excission of the major ducts “Hadfield’s operation”

24
A 20 year old woman presents to the OPD after noticing a swelling on her right breast. The swelling is about 2 cm in size, with well- defined borders and a smooth surface. lymph nodes are not palpable. What is the most probable diagnosis? Incase if the patient was 40 years old, with a positive history of breast cancer in the family, how would your management change?

25
A 22 year old lady presents to the OPD one week after giving birth. Both her breasts were swollen and tender, with cracked nipples. What is your diagnosis? What organism is most commonly associated with a presentation like this? What treatment will you prescribe? How will you treat cracked nipples What possible complications can occur?

26
1) Bacterial mastitis: associated with Cracked nipples or “Cleansing the baby’s mouth” 2) staph A. 3) Drain the abscess after emptying milk, and treat with an appropriate antibiotic, flucloxacillin. Analyze pus with cytology for inflammatory carcinoma. 4) Rest breast for 24-48 hours and empty via a breast pump 5) if the abscess is not drained, and antibiotics are prescribed, an antibioma can result.
 Drain the abscess after emptying milk, and treat with an appropriate antibiotic, flucloxacillin. Analyze pus with cytology for inflammatory carcinoma. 4) Rest breast for hours and empty via a breast pump 5) if the abscess is not drained, and antibiotics are prescribed, an antibioma can result..")
27
Inflammations of the Breasts 1) Bacterial mastitis 2) Mastitis from milk engorgement 3) chronic inflammatory abscess 4) tubercolosis/ syphillis/ actinomycosis 5) Mondor’s disease (Thrombophlebitis of the superficial veins of the breasts & ant. Chest wall)
.")
28
AAFP journal, April 15, 2010. Volume 61/ No. 8 The most common breast problems for which women consult a physician are breast pain, nipple discharge and a palpable mass.

29
A 30 year old female comes to your OPD with breast pain. On inquiry, the patient tells your that this pain occurs off and on but does not interfere with her daily activities. Examination of the breast and surrounding tissue is unremarkable. The patient displays concern regarding breast cancer and tells you that her neighbor died from it. WHAT IS THE NEXT BEST STEP

30
A) REASSURE B) ASK HER TO RECORD A PAIN CHART AND BRING IT ON HER NEXT FOLLOW UP AFTER 3 MONTHS C) ORDER A MAMMOGRAM D) PRESCRIBE AN ANALGESIC
 REASSURE B) ASK HER TO RECORD A PAIN CHART AND BRING IT ON HER NEXT FOLLOW UP AFTER 3 MONTHS C) ORDER A MAMMOGRAM D) PRESCRIBE AN ANALGESIC")
31
A) REASSURE B) ASK HER TO RECORD A PAIN CHART AND BRING IT ON HER NEXT FOLLOW UP AFTER 3 MONTHS C) ORDER A MAMMOGRAPHY D) PRESCRIBE AN ANALGESIC
 REASSURE B) ASK HER TO RECORD A PAIN CHART AND BRING IT ON HER NEXT FOLLOW UP AFTER 3 MONTHS C) ORDER A MAMMOGRAPHY D) PRESCRIBE AN ANALGESIC")
32
Breast Pain THOROUGH HISTORY PHYSICAL EXAMINATION MAMMOGRAPHY AND /OR SONAR ABNORMALITIES…….BIOPSY CLASSIFY REASSURANCE

33
Why does it occur? Unknown etiology Hormonal influence? No reproducible alterations in estrogen, progesterone or prolactin levels have been identified in women with mastalgia. Premenstrual water retention in the breasts has also been proposed as a cause of mastalgia and is the rationale for the use of diuretics in the treatment of this condition.

34
EXCLUDE.. Cardiac Respiratory Dermatological Musculoskeletal Endocrine Gynaecological Habits

35
History? Type of pain? Location? Relationship to the menstrual cycle (cyclic or non-cyclic)
")
36
Cyclical and Non-cyclic Pain Cyclic breast pain occurs more often in younger women. Most cyclic pain resolves spontaneously. Mostly bilateral

37
Theories of Causation!

38
Noncyclic mastalgia is most common in women 40 to 50 years of age. It is often unilateral and is described as a sharp, burning pain that appears to be localized in the breast. Noncyclic mastalgia is occasionally secondary to the presence of a fibroadenoma or cyst, and the pain may be relieved by treatment of the underlying breast lesion.

39
Patient concerns are usually related to cancer. It is rarely a symptom of cancer

40
Examination & Investigations Exclude breast mass When the physical examination is normal, imaging studies are not indicated in women younger than 35 years of age. women 35 years of age and older should undergo mammography unless a mammogram was obtained in the past 10 to 12 months.

41
MANAGEMENT 1) Exclude cancer 2) reassure 3) pain chart 4) evening primrose oil, Danazol (if very severe), Tamoxifen (rarely needed)
 Exclude cancer 2) reassure 3) pain chart 4) evening primrose oil, Danazol (if very severe), Tamoxifen (rarely needed)")
42
2) Nipple Discharge This common breast problem has been reported in 10 to 15 percent of women with benign breast disease and in 2.5 to 3 percent of women with breast cancer.
 Nipple Discharge This common breast problem has been reported in 10 to 15 percent of women with benign breast disease and in 2.5 to 3 percent of women with breast cancer.")
43
Differentials Eczema, Paget’s disease, psoriasis, chancre (discharge from the surface) Intraductal ca, intraductal papilloma, euct ectasia (bloody discharge) Fibrocysitc disease, duct ectasia, carcinoma (serous discharge)
 Intraductal ca, intraductal papilloma, euct ectasia (bloody discharge) Fibrocysitc disease, duct ectasia, carcinoma (serous discharge)")
44
Pathological or not? Nipple discharges are classified as pathologic if they are spontaneous, bloody or associated with a mass. Pathologic discharges are usually unilateral and confined to one duct. The most common cause of pathologic nipple discharge is intraductal papillomoa & duct ectasia. If a palpable mass is present in association with a discharge, the likelihood of cancer is greatly increased.

45
Physiologic discharges are characterized by discharge only with compression and by multiple duct involvement. These discharges are frequently bilateral. With either type, the discharge fluid may be clear, yellow, white or dark green.

46
Examination & Investigation Localization of the affected duct and examination of discharge for occult blood Cytology generally is not useful because the absence of malignant cells does not exclude cancer, and a positive result cannot distinguish intraductal cancer from invasive cancer. Mammogram for the identification of masses and calcifications

47
All patients with spontaneous or unilateral nipple discharge should be referred for surgical evaluation (specially if bloody or serous discharge) A terminal duct excision is both diagnostic and, for discharges that turn out to have a benign cause, therapeutic.
 A terminal duct excision is both diagnostic and, for discharges that turn out to have a benign cause, therapeutic.")
48
Galactorrhea Never a symptom of breast cancer

49
nipple stimulation chest wall trauma oral contraceptives, phenothiazines, antihypertensive drugs and a variety of tranquilizers. endocrine abnormalities: hypothyroidism, pituitary adenomas

50
Benign lumps Cysts Galactocele Fibroadenoma phylloides

Similar presentations














>")









