Download presentation
Presentation is loading. Please wait.

1
La terapia antifungina nel paziente critico Francesco Menichetti, MD Head, Infectious Diseases Unit Ospedale Nuovo Santa Chiara Pisa, Italy SIMIT 2015 SIMPOSIO SIMIT-SIARTI Catania 10 novembre 2015

2
Disclosures Research grants Astellas, Gilead, MSD, Pfizer Advisor/consultant Astellas, Astra Zeneca, Cubist, Durata, Gilead, MSD, Novartis, Pfizer Speaker/chairman Astellas, Gilead, MSD, Novartis, Pfizer

3
Risk Factors for Invasive Candidiasis Eggimann P et al Ann Intens Care 2011 Colonization of several body sites Broad spectrum antibiotics Immunosuppression Neutropenia Burns (>50%) Disruption of physiological GI barriers Major abdominal surgery Surgery of the urinary tract with candiduria Major trauma (ISS>20) Multiple transfusions Parenteral nutrition Haemodialysis APACHE II score >20 Central venous catheter Candiduria >10 5 cfu/ml Young and old ages Diabetes Renal failure Recent surgery Urinary catheter Vascular catheters Prolonged ICU stay (>7days)
 Disruption of physiological GI barriers Major abdominal surgery Surgery of the urinary tract with candiduria Major trauma (ISS>20) Multiple transfusions Parenteral nutrition Haemodialysis APACHE II score >20 Central venous catheter Candiduria >10 5 cfu/ml Young and old ages Diabetes Renal failure Recent surgery Urinary catheter Vascular catheters Prolonged ICU stay (>7days)")
4
Candidemia 2012-2014 Pisa Hospital: 373 episodes

5
21, 9: e71-e72

6
Epidemiology of IFI in the ICU: Results of a Multicenter Italian Survey (AURORA Project) Montagna MT et al. Infection 2013; 41(3): 645-53 18-month surveillance program, 18 ICUs in South Italy 105 episodes of IFIs in 5,561 patients Incidence higher for Candida BSI than filamentous fungi 16.5 cases and 2.3 cases per 1,000 admissions, respectively The overall crude mortality rate 42.8% for Candida & 61% for molds 60% of Candida BSI caused by Candida non-albicans C. parapsilosis the most common (61.8 %)
: month surveillance program, 18 ICUs in South Italy 105 episodes of IFIs in 5,561 patients Incidence higher for Candida BSI than filamentous fungi 16.5 cases and 2.3 cases per 1,000 admissions, respectively The overall crude mortality rate 42.8% for Candida & 61% for molds 60% of Candida BSI caused by Candida non-albicans C. parapsilosis the most common (61.8 %).")
7
Candidemia, Pisa Hospital 2012-2013 Antifungal therapy Med Int (n=64) ICU (n=26) < 24h27 (30%)15 (23,4%)12 (46,1%) 24/48h13 (13,3%)10 (15,6%)3 (11,5%) 48/72h8 (8,9%)5 (7,8%)3 (11,5%) >72h10 (11,1%)6 (9,4%)4 (15,4%) no therapy22 (27,5%)20 (35,7%)2 (8,3%) In hospital mortality (%)39 (43,3%)24 (37,5%)15 (57,7%)
 ICU (n=26) < 24h27 (30%)15 (23,4%)12 (46,1%) 24/48h13 (13,3%)10 (15,6%)3 (11,5%) 48/72h8 (8,9%)5 (7,8%)3 (11,5%) >72h10 (11,1%)6 (9,4%)4 (15,4%) no therapy22 (27,5%)20 (35,7%)2 (8,3%) In hospital mortality (%)39 (43,3%)24 (37,5%)15 (57,7%)")
9
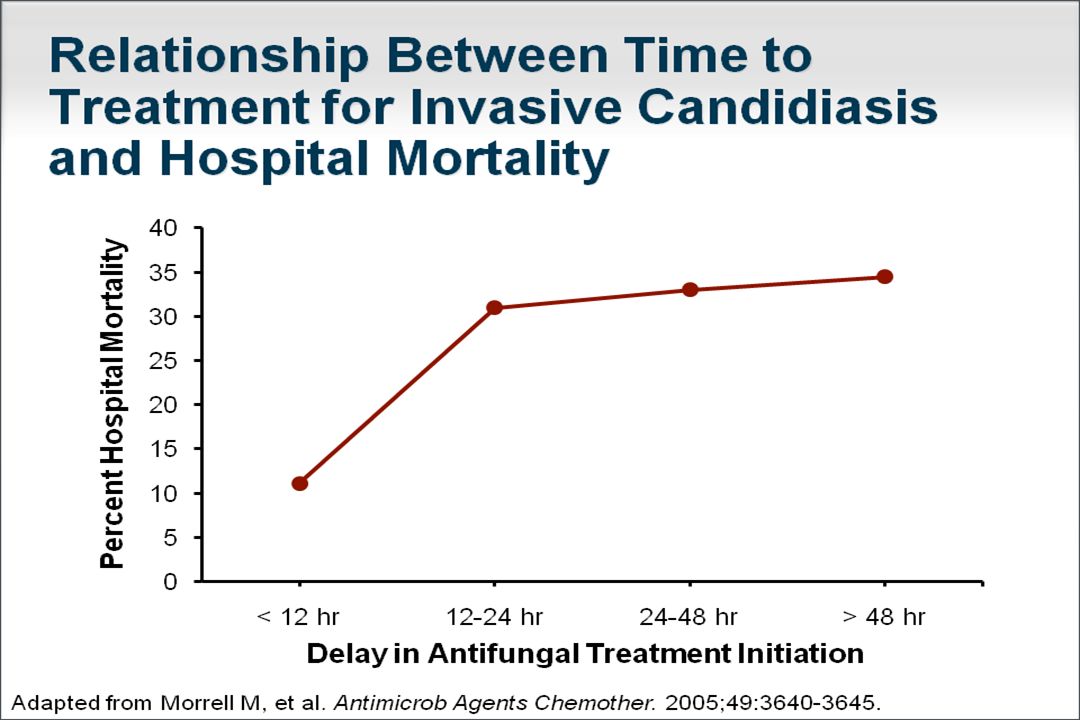
224 consecutive patients with septic shock and a positive blood culture for Candida species. EARLY (< 24 HRS) TREATMENT NO TREATMENT WITHIN 24 HRS OF SHOCK
 TREATMENT NO TREATMENT WITHIN 24 HRS OF SHOCK.")
10
Kollef M et al. Clin Infect Dis. 2012 Jun;54(12):1739-46 224 consecutive patients with septic shock and a positive blood culture for Candida species.
: consecutive patients with septic shock and a positive blood culture for Candida species..")
11
Epidemiology of IFI in ICU: Results of a Multicenter Italian Survey (AURORA Project) Montagna MT et al. Infection 2013; 41(3): 645-53 18-month surveillance program, 18 ICUs in South Italy 105 episodes of IFIs in 5,561 patients Incidence higher for Candida BSI than filamentous fungi 16.5 cases and 2.3 cases per 1,000 admissions, respectively The overall crude mortality rate 42.8% for Candida & 61% for molds 60% of Candida BSI caused by Candida non-albicans C. parapsilosis the most common (61.8 %)
: month surveillance program, 18 ICUs in South Italy 105 episodes of IFIs in 5,561 patients Incidence higher for Candida BSI than filamentous fungi 16.5 cases and 2.3 cases per 1,000 admissions, respectively The overall crude mortality rate 42.8% for Candida & 61% for molds 60% of Candida BSI caused by Candida non-albicans C. parapsilosis the most common (61.8 %).")
12
Isolates 373 Patients 351 C. albicans 188 (50%) C. parapsilosis 98 (26%) C. glabrata 38(10%) C. tropicalis 23(6%) C. krusei 8 others 22 Candidemia 2012-2014 Pisa Hospital: 373 episodes
 C. glabrata 38(10%) C. tropicalis 23(6%) C. krusei 8 others 22 Candidemia Pisa Hospital: 373 episodes.")
13
Clinically important characteristics of Candida spp. C. albicans: 2% resistant to fluconazole C. tropicalis: high virulence C. parapsilosis: low virulence; CVC-related infections C. glabrata: dose-depending resistance to fluconazole C. krusei: innate resistance to fluconazole C. lusitaniae: resistance to amphotericin B

14
The Biofilm challenge

15
OR (95% CI) P Inadequate antifungal therapy 2.35 (1.09-5.10) 0.03 Infection biofilm-forming Candida species 2.33 (1.26-4.30) 0.007 APACHE score 1.03 (1.01-1.15) 0.001 Tumbarello et al JCM 2007
 P Inadequate antifungal therapy 2.35 ( ) 0.03 Infection biofilm-forming Candida species 2.33 ( ) APACHE score 1.03 ( ) Tumbarello et al JCM 2007")
16
Biofilm activity of antifungals vs different Candida species Choi HW et al. Antimicrob Agents Chemother 2007; 51:1520-23

17
Ideal strategy for the management of IFI in ICU pts Timeliness: early start is crucial Appropriateness: the right drug to the right patient Adequacy: the right schedule for the specific patient & site of infection Patient outcome is related to these elements

18
Empirical fluconazole versus placebo for ICU pts: a randomized trial Fluco iv 800 mgPlacebo95% CI Population122127 Succesfull outcome44 (36%)48 (38%)0,69 to 1,32 Persistent fever51%57% Documented IC5%9%0,22 to 1,49 Discontinuation for AEs 7 (5%)10 (7%) Schuster MG et al. Ann Intern Med 2008;149: 83-90 Evidence against the efficacy of fluconazole or against the empiric antifungal strategy in unselected population ? Evidence against the efficacy of fluconazole or against the empiric antifungal strategy in unselected population ?

19
How to select high-risk pts for Invasive Candidiasis:? Candida Risk Factors (Jorda’- Marcos) Candida Colonization Index (D. Pittet) Candida Score (C. Leon) Prediction Rule + Colonization (L. Ostrosky-Zeichner) Blood cultures & Biomarkers
 Candida Colonization Index (D. Pittet) Candida Score (C. Leon) Prediction Rule + Colonization (L. Ostrosky-Zeichner) Blood cultures & Biomarkers.")
21
Any help from the lab for diagnosing candidaemia? SpecimenTestConsiderationsRemarks/Recommendations SerumMannan and Anti-Mannan B-D-Glucan Combined detection No specific for Candida RECOMMENDED Serial determinations may be necessary. High NPV RECOMMENDED (for Fungitell) No recommendation for other tests. Serial determinations are recommended (twice a week). Low specificity, Low sensitivity, High NPV: C II
 No recommendation for other tests. Serial determinations are recommended (twice a week). Low specificity, Low sensitivity, High NPV: C II.")
22
CAGTA Anticorpi anti germ-tube di C. albicans Fattore di virulenza utilizzato per l’invasività

24
Blood cultures Oral cavity GI tract CarriageCarriage Urinary tract SerologySerology Mannan/anti Mannan Beta-D-glucanCAGTA BiopsyBiopsy MicroscopyCulturePCR Diagnosis of candidiasis Respiratory tract Always identify colonization colonization and infection !

25
What to do with the “ surveillance cultures ” in the asymptomatic patient ? Positive blood culture for candida: treat immediately Culture positive from urinary catheter: don’t treat Culture positive from peritoneal drainage: don’t treat Tracheal aspirate or BAL positive for candida: don’t treat Surveillance cultures may generate inappropriate antifungal treatments

26
Candida isolation from respiratory secretions in pts with pneumonia A 2-year autopsy study on 232 ICU pts 135 pts with pneumonia No Candida Pneumonia in 77 pts with pneumonia at autopsy & positive TA and/or BAL cultures for Candida in the previous 2 weeks No Candida Pneumonia in the other 58 pts without pre-mortem Candida isolation Meersseman W ICM 2009; 35: 1526-31

27
Catheter-related Candidaemia “Catheters should be removed in case of CRBSI due to Candida species; Antifungal therapy is recommended for all cases”. IDSA Guidelines for Intravascular Catheter-Related Infection CID 2009:49:1-45 “Indwelling CVC serve as a main source of infection independent of the pathogenesis of candidaemia in the individual patients and should be removed whenever feasible”. M.Ruhnke, Mycoses 2011, 54:279-310 Remove CVC if candidemia treated with azoles or D-Ampho (B II) No advantage of early removal (< 48 hrs) in case of L-Ampho or echinocandins (removal: D II) ESCMID Diagnostic & Management Guideline for Candida Diseases 2011 Always remove non surgical CVC and treat for 14 days after the first negative blood culture
 No advantage of early removal (< 48 hrs) in case of L-Ampho or echinocandins (removal: D II) ESCMID Diagnostic & Management Guideline for Candida Diseases 2011 Always remove non surgical CVC and treat for 14 days after the first negative blood culture.")
28
Not only candidemia

29
Treatment of candidemia: guidelines comparison IDSA 2009ESCMID 2012 FlucoAICI Itraco-DII VoricoAIBI L-AMB AI (intolerance to other drugs) BI ABLC / ABCD-CII D-AMBAI (limited resources)DI CaspoAI MicaAI AnidulaAI D-Ampho: no more ! Fluconazole: severe downgrading More emphasis on Echinocandins D-Ampho: no more ! Fluconazole: severe downgrading More emphasis on Echinocandins

30
Candidemia in critically-ill patients: fluconazole or echinocandins ? FluconazoleEchinocandins Spectrum of activity limitedC.glabrata & C. krusei included C. parapsilosisBetter microb. activityClinical evidence of efficacy (caspo) Antifungal activityfungistaticfungicidal Activity vs. biofilmlowhigh RCTs in candidemia/IC Inferior to anidulafungin Better than ampho D, similar to AmBisome RCTs in empirical therapy No difference with placebo in ICU Better than ampho B liposomal in neutropenia (caspo) CostVery lowMedium/high Guidelines IDSA/ECSCMID CIII/DIAI/AI
 Antifungal activityfungistaticfungicidal Activity vs. biofilmlowhigh RCTs in candidemia/IC Inferior to anidulafungin Better than ampho D, similar to AmBisome RCTs in empirical therapy No difference with placebo in ICU Better than ampho B liposomal in neutropenia (caspo) CostVery lowMedium/high Guidelines IDSA/ECSCMID CIII/DIAI/AI.")
31
Step-down strategy Induction therapy (2 weeks) with an echinocandin for critically ill pts (sepsis/severe sepsis) Re-evaluate induction therapy on the basis of isolate identification, patient condition, site of infection After 2 weeks or more consider step-down therapy with an oral azole
 with an echinocandin for critically ill pts (sepsis/severe sepsis) Re-evaluate induction therapy on the basis of isolate identification, patient condition, site of infection After 2 weeks or more consider step-down therapy with an oral azole")
32
Optimal management of invasive candidiasis in 2015 First line echinocandin -Spectrum +, higher efficacy than fluconazole (C. albicans) Local epidemiology/risk group to be considered Take into account prior exposure to echinocandin/azoles -Azole => Candin ; Candin => L-Amb Early adequate source control -Catheter withdrawal (although persistent controversies) -Abdominal surgery ? Early switching (when infection controlled) Urgent need for more effective diagnostic methods Denning & Bromley, Science 2015
 Local epidemiology/risk group to be considered Take into account prior exposure to echinocandin/azoles -Azole => Candin ; Candin => L-Amb Early adequate source control -Catheter withdrawal (although persistent controversies) -Abdominal surgery . Early switching (when infection controlled) Urgent need for more effective diagnostic methods Denning & Bromley, Science")
Similar presentations