Download presentation
Presentation is loading. Please wait.

1
Placenta &Amniotic fluid Dr. Dina Nawfal Dr. Dina Nawfal

2
Development of the placenta: It is a functioning feto maternal organ originated from both the trophoblastic chorionic plate (fetal part) and the decidual plate ( maternal part ) inclosing a space containing maternal blood ( hemochorial placenta). Formation of the villi : the lacunae ( a small cavities) appears in the syncytium and are separated by trabeculae. the syncytiotrophoblasts grows into the endometrium (decidua) and invades the maternal capillaries so blood extravasates to the lacunae
 appears in the syncytium and are separated by trabeculae. the syncytiotrophoblasts grows into the endometrium (decidua) and invades the maternal capillaries so blood extravasates to the lacunae.")
3
the primary villi appears at the beginning of third week when cytotrophoblasts begin to multiply and grow into each trabicula secondary villi when extraembryonic mesoderm begin to invade the center of each primary villus tertiary villi When the fetal blood vessels appears in the mesoderm Terminal villi After the 20 th week the cytotrophoblast disappear & finally only thin layer of syncytium remains together with the maternal capillary endothelium will separate the maternal and fetal blood to facilitate the exchange function of the placenta.

5
The functional unit of the placenta is fetal cotyledon the mature placenta has about 15 - 20 cotyledons, which are grouped into visible lobes. The placenta at term A discoid spongy structure it is circular in shape with diameter of 15-25 cm and 3cm thickness it weighs about 500-600 gm usually attached near the fundus, to either the anterior or posterior surface.

6
On inspection it consist of 1-Maternal surface 2-Fetal surface

7
Function of placenta Enables the fetus to take oxygen and nutrients from the maternal blood. Excretory function when carbon dioxide and other waste products pass from the fetus to the maternal circulation. Barrier against the transfer of infection to the fetus. Secrete hormones like ( HCG ), oestrogen, progesterone and (hPL).
, oestrogen, progesterone and (hPL)..")
8
Normal placentation The maternal flow to the placenta from 50mL/min in the 1 st trimester to 600mL/min at term This increase in perfusion can only be accomplished by the anatomical conversion of the maternal spiral arteries by trophoblastic invasion.

9
Abnormal placentation leads to: Pre-eclampsia and pregnancy induced hypertention Intrauterine growth restriction(IUGR). Abruptio placentae. Placental abnormalities Infraction : ischemic necrosis of cotyledon resulting from spiral artery occlusion Basal haematomas : caused by damage to spiral artery Calcification of the placenta : deposition of calcium within the placental tissue

10
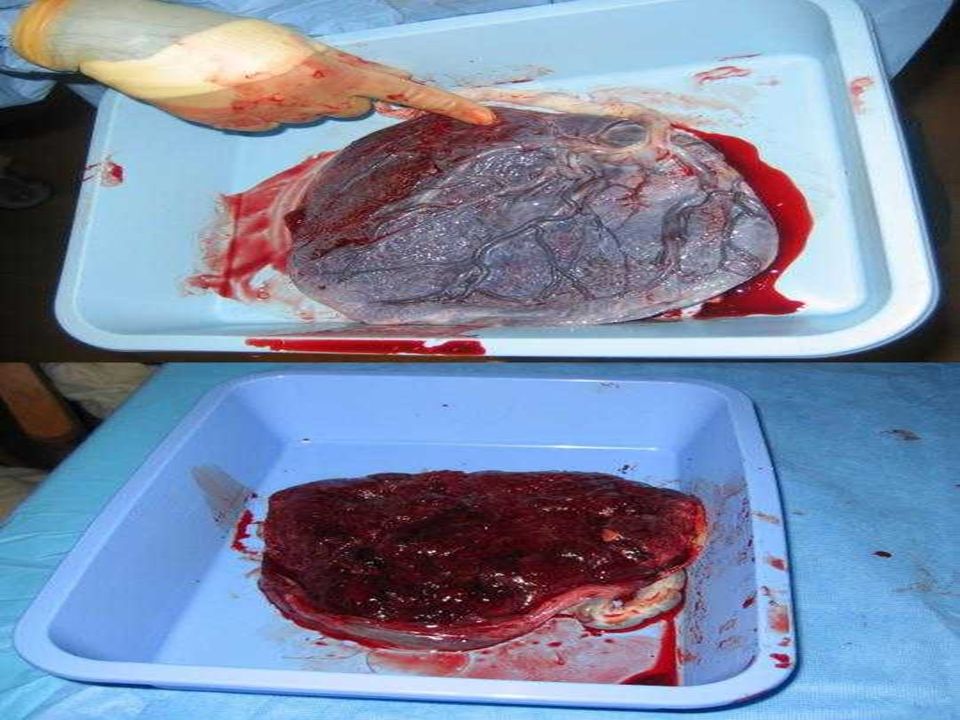
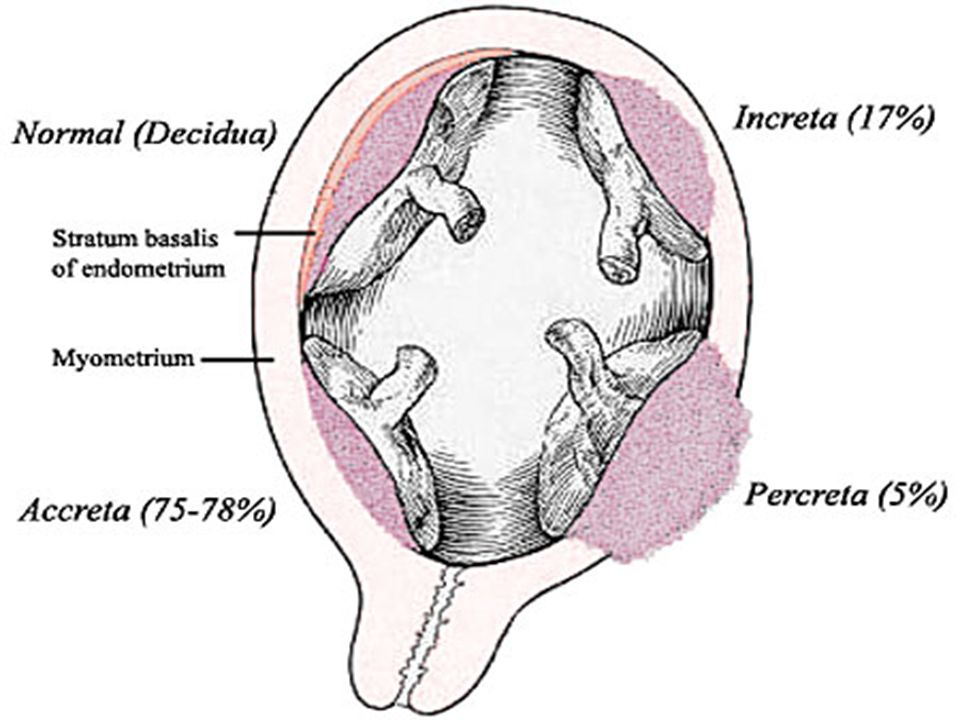
Anomalies in weight Hydropic placenta as in hydrops fetalis Bilobate and trilobate placenta Placenta succenturiata (PPH) Placenta circumvallata (placental abruption) Morbid adherence of the placenta It results from increased penetration of the decidua and myometrium by the chorionic villi. The severity is determined by the depth of invasion

13
Placenta accreta penetration of villi into the superficial part of the myometrium Placenta increta penetrate deeply through the decidua into the myometrium. Placenta percreta penetration can even be seen on the serosal surface of the uterus and may invade the bladder

15
Placenta previa pregnancies the placenta is implanted wholly or partially on the lower uterine segment of the uterus Tumours of the placenta choriocarcinoma, vascular tumours called haemangioma.

16
The umbilical cord At term the umbilical cord is about 50cm length 2cm in diameter it is tortuous causing false knots it contain 2 arteries and 1 vein covered with jelly of Wharton and amnion.

17
Abnormal length Excessive length predispose to prolapse of the cord, Short cord predispose to delay in 2 nd stage of labour, premature separation of the placenta, inversion of uterus are rare complication. Knots in the cord formed by fetal movement, they do occasionally cause IUD

18
Abnormal insertion of the cord The cord usually attached to the placenta slightly in an eccentric position, Velamentous insertion of the cord the cord is attached to the membrane at some distance from the edge of the placenta

19
Amniotic Fluid It is a fluid that filled the amniotic cavity, usually turbid from a mixture of solid particles derived from fetal skin and amniotic epithelium Amniotic fluid production Early in pregnancy, the amniotic fluid is initially secreted by the amnion. By the 10th week it is mainly a transudate of the fetal serum via the skin and umbilical cord From 16 weeks gestation, the fetal kidney play an increasing role in the production of amniotic fluid and small lung fluid.

20
Disposal of the amniotic fluid: Partly by the absorption through the amnion to the maternal plasma and partly by fetal swallowing and absorption in to the intestine to enter fetal circulation. Amniotic fluid volume increases progressively 10 weeks:30 ml 30 weeks:600 mL 38 weeks: 1000 mL 40 weeks:800 mL 42 weeks: 350 mL

21
Amniotic fluid function: allows the fetus room for growth, movement and development. for fetal pulmonary development which requires a fluid filled respiratory tract the amniotic fluid had a protective role for the fetus, it contain antibacterial activity during labor and delivery, the amniotic fluid continues to serve as a protective medium for the fetus & aiding dilatation of the cervix

22
THANK YOU

Similar presentations




 and abnormalities of the Third Stage Sept 12 – Dr. Z. Malewski.>")
















