Download presentation
Presentation is loading. Please wait.

1
Spine Marrow: Pathologic Fractures and Ditzels
Mark E. Schweitzer, M.D. Chief of Radiology Hospital The Ottawa Hospital Professor of Radiology The University of Ottawa

2
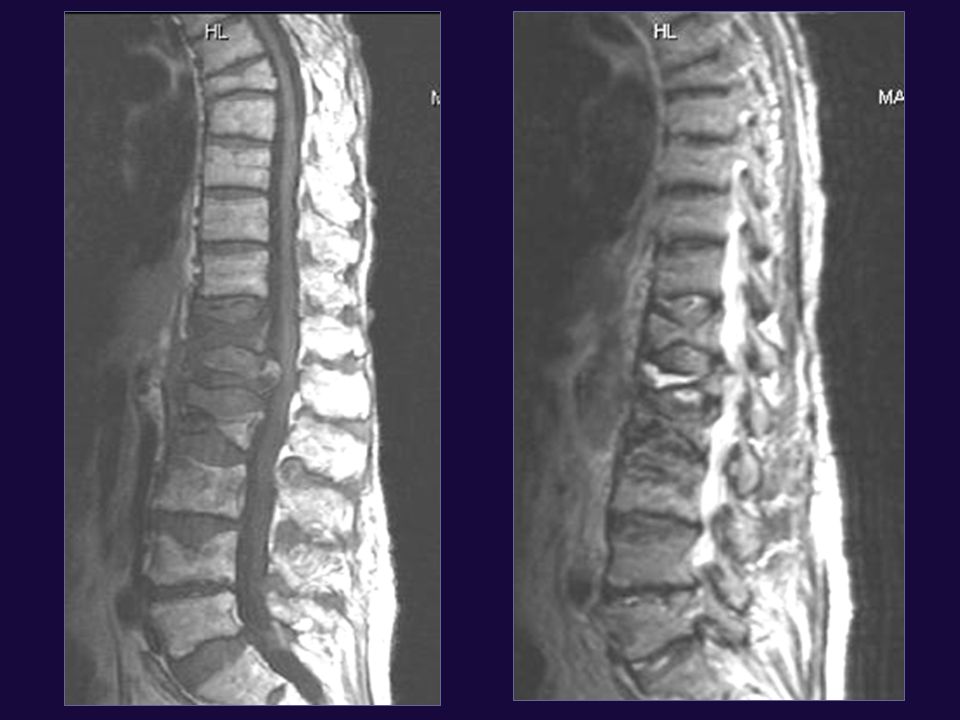
The most likely to be metastatic is A B C D
Breast met a more than D since D is cervial spine The most likely to be metastatic is A B C D

3
MARROW SIGNAL Diffuse Multifocal Focal (as far as you can see)
")
4
This is a child with congenital anemia
This is a normal child This is a child with congenital anemia This could be indolent multiple myeloma This is skeletal carcinomatosis

5
Diffuse marrow Lower than disc on T1 Drops on Salt and pepper
out of phase = red marrow Salt and pepper = myeloma Look for nodes = lymphoma Check acetabulum and for bullseyes If yes benign if no o/w carcinomatosis, leukemia

6
This could be sickle cell All the above
This could be anemia This could be CML This could be gauchers This could be sickle cell All the above

7
CML CML T1 T2

8
This could be skeletal carcinamatosis
This is normal marrow This patient is anemic This could be skeletal carcinamatosis This is multiple myeloma and of low grade

9
Is this just weird normal marrow or multiple myeloma?
MULTIPLE MYELOMA MR PATTERNS Multiple nearly similar sized Small areas T2W Apparently red marrow (infiltration) Salt and pepper May have too many or atypical location of fxs Focal lesion (plasmacytoma)
 Salt and pepper. May have too many or atypical location of fxs. Focal lesion (plasmacytoma)")
10
Two years later Early MM in out in out

11
T1 T2 out MM normal except out-of-phase

12
MM Salt n’ peppa T2 T1

13
T1 T2 Multiple myeloma almost nl Except for plasmacytoma

14
Multiple myeloma

15
Focal Vertebral Marrow: Low Signal
T1 only Higher specificity Diffuse in a vertebrae or portion of marow Fracture? Be careful T2 useful only if dark or halo

16
T1 and T2 Low field pagets

17
The probability that this is malignant 30% 50% 66% 85%
d

18
Is this a benign or malignant fracture?

20
BENIGN FRACTURES NO NOT IGNORE MORPHOLOGY Osteoporosis Trauma T score
Cervical M > F Younger Thoracic Slightly older Usually below T7 Lumbar Older yet Osteoporosis A type of trauma Not cervical T7 and below Most at T10-L4 Most common L2 Most likely not to be benign L5 T score > -2.5 Only 1/3 of fragility NO NOT IGNORE MORPHOLOGY

21
Compression? Yes No Benign Benign Benign Benign Vertebral Body
Is the marrow diffusely involved? Follow up Bone Scan Biopsy Yes No Fracture line? OUT OF PHASE No drop NO Sequential? Yes Drop > 16% Benign Benign Benign Benign

23
Osteoporotic fractures

25
PATHOLOGIC FRACTURE: 2° SIGNS (I)
Extensive involvement posterior elements including pedicle Non-sequential Large soft tissue mass or peridural Atypical locations: L5 Dens Upper to mid Thoracic Atypical appearance (one side worse, “irregular”) No fx line- or vertical
 No fx line- or vertical.")
26
Compression 2° mets T1 Axial T1 STIR

27
Fx line= benign T1 T2

28
PATHOLOGIC FRACTURE: 2° SIGNS
No high signal in disc above Inferior > superior endplate ddx: metabolic bone disease No PLL avulsion Posterior bowing

30
Benign fracture

33
Path fracture

34
T1 T2 fat sat Sequential

35
T1 T2 fat sat Metastases Posterior bowing Multiple bodies Posterior

36
Lung CA mets

37
Soft tissue mass especially peridural

38
Maligant inferior > superior

39
T1 T2 Gad Probability that this is malignant 30% 50% 65% 90% c

40
PATHOLOGIC FRACTURE: 2° SIGNS
Look for metastases elsewhere Look for benign fractures elsewhere Remember curse of epidemiology

41
Pathologic fracture

42
lymphoma

43
T1 T2 Gad PLL avulsion Sequential location Complete fat/
degenerated disc T1 T2 Gad

44
Fracture and Met *No enhancement T1 T2 Gado

45
This is a malignant fx This is a benign, acute fx I can’t tell Show me a plain film before I decide

46
VERTEBRAL FACTURES DO NOT IGNORE LOCATION Risk of Malignancy
Jefferson Teardrop (cervical) Chance Odontoid Burst Plana Anterior compression Atypical compression (r > l side, upper to mid T)
 Chance. Odontoid. Burst. Plana. Anterior compression. Atypical compression (r > l side, upper to mid T)")
47
Breast path fracture

48
Probability that this is malignant 25% 40% 65% 85%
c Probability that this is malignant 25% 40% 65% 85%

49
REMEMBER: ***Be cautious and follow-up***
Hyperacute traumatic/osteoporotic Fractures can look malignant ***Be cautious and follow-up***

50
Acute osteoporotic mimic mets

51
If I am not sure, what should I do?
Out of phase Follow-up/old films Tumor does not rapidly evolve Bone scan Thin slice CT X-ray Contrast Diffusion/perfusion/spectro

52
T1 T2 in out Xrt with out of phase

53
(also treatment response):
CT signs of benignity (also treatment response): Sclerotic margins Central fat Typical Ca++ Treated mm with sclerotic rims
: Sclerotic margins. Central fat. Typical Ca++ Treated mm with sclerotic rims.")
54
Treated MM

55
Benign fracture ues of gad

56
T GAD T CT

57
Kummel’s

58
3 weeks later Fx f/u Probability that this is malignant 25% 45% 65%
85% b 3 weeks later Fx f/u

59
Two months later initial
See scan 2 months before-acute fracture in feb Two months later initial

60
This is a vertebra plana This is subacute This patient must have
osteoporosis D. All the above d

61
When should I not worry about a vertebra plana?

62
Leukemia T2 T1

63
VERTEBRA PLANA >75% loss of height
Usually equal posterior and anterior ddx: Eosinophilic granuloma Metastases Osteoporotic fractures No more common to be malignant than more typical fractures Look at the rest of the spine

64
plana

65
T1 T2 Gad Lymphoma

66
plana

67
T1 T2

69
Malignant plana

70
THE CHANCE THAT THIS IS BENIGN 10% 30% 60% 85%
d THE CHANCE THAT THIS IS BENIGN 10% 30% 60% 85%

71
What do I do with a low signal ditzel on a T1W image?
If a portion of the vertebral body, different rules and lower threshold

73
Ditzel Focal T1 low signal Is it low on T2 is there a halo
Yes probable met Bone island/ Endplate ^ >2cm out of phase Is there central fat Yes, red marrow 1-2 cm CT No and smaller then 1 cm or multifocal = Bone scan

74
Ditzel Focal T1 low signal Is it low on T2? Yes: probable met
No; Is there a halo? Yes: probable met Yes =Bone island/ Endplate Δ >2cm out of phase does not ddx lesions Is there central fat? Yes: red marrow 1-2 cm CT No and smaller than 1 cm or multifocal = Bone scan

75
ALL, treated with 2nd necrosis

76
T In Out MM

78
Bone island-does not drop
In phase is not a substitute for T1

79
T1W T2W (halo) Diffusion out of phase
Breast met

80
L5 ditzel Subtle halo

81
T1 T2

82
Lung mets

83
Rim bright on T1W Center bright on T2W

85
Lung mets

86
T2W gad Is there a role for contrast In short no Only to see
epidural component T2W gad

87
Sclerotic mets can mimic bone islands
Sclerotic mets infrequently fracture PET has few false negatives Cannot be seen after treatment c

88
Is that a bone island or a sclerotic met?
Many sclerotic mets are not that low on T2W √ for reactive interface and homogeneity Size also, but helps to a lesser degree One way mets heal is with sclerosis (vs fatty conversion)
")
89
T1 Bone island T2 T1

91
mets Malig schorl’s T1 Gad T2

92
T1 T2 Sclerotic mets

93
Sclerotic breast mets

94
Compression? Yes No Benign Benign Benign Benign Vertebral Body
Is the marrow diffusely involved? Follow up Bone Scan Biopsy Yes No Fracture line? OUT OF PHASE No drop NO Sequential? Yes Drop > 16% Benign Benign Benign Benign

95
Ditzel Focal T1 low signal Is it low on T2? Yes: probable met
No; Is there a halo? Yes =Bone island/ Endplate Δ Is there central fat? >2cm out of phase Yes: red marrow 1-2 cm CT No and smaller than 1 cm or multifocal = Bone scan

96
Breat met

97
This happened to this patient in adolescence
This patient has osteoporosis This patient may have metasases All the above

98
Could that Schmorl’s node be symptomatic?

100
TYPES OF SCHMORL’S Juvenile: low T1/T2 Vascularized-adj edema
Acute/Traumatic- also edema Usually subacute Neoplastic-usu. Inferior endplates/ “chronic/slow growing” tumors prostate/breast

104
Malignant Schmorl’s

105
This is a diffuse marrow disorder This is Paget’s This is lymphoma
osteopetrosis This is a diffuse marrow disorder This is Paget’s This is lymphoma This is Multiple Myeloma

106
Neuropathic spine

Similar presentations















 – A NEW APPROCH AND OUR EXPERIENCE Kamenetsky Natalya (1), Rachmilewitz Eliezer.>")

















