Download presentation
Presentation is loading. Please wait.

1
Urinary Tract Infection In Children

2
ETIOLOGY Localization cystitis (infection localized to the bladder) pyelonephritis (infection of the renal parenchyma, calyces, and renal pelvis) renal abscess(which may be intrarenal or perinephric) bacteria commonly causing infection Escherichia coli Klebsiella Proteus Enterococcus Pseudomonas Staphylococcus saprophiticus
 pyelonephritis (infection of the renal parenchyma, calyces, and renal pelvis) renal abscess(which may be intrarenal or perinephric) bacteria commonly causing infection Escherichia coli Klebsiella Proteus Enterococcus Pseudomonas Staphylococcus saprophiticus")
3
EPIDEMIOLOGY Approximately 8 o/o of girls and 2 o/o of boys have a UTI by 11 years of age. The lifetime incidence of UTI in females is about 30 o/o compared to only 1 o/o in males. Approximately 75 o/o of infants younger than 3 months of age with bacteriuria are male compared with only 10% berween 3 and 8 months of age. After 12 months of age, UTI in healthy children usually is seen in girls.

4
Predisposing Factors short urethra in girls Uncircumcised male infants Obstruction to urine flow and urinary stasis: – Anatomic abnormalities – Nephrolithiasis – Renal tumor – Indwelling urinary catheter – Ureteropelvic junction obstruction – Megaureter – Extrinsic compression – Pregnancy – Vesicoureteral reflux

5
CLI N ICAL MANIFESTATIONS Neonate failure to thrive feeding problems fever direct hyperbilirubinemia 1 month to 2 years old feeding problems failure to thrive diarrhea vomiring unexplained fever

6
At 2 years of age, children begin to show the classic signs of UTI such as urgency, dysuria, frequenry, and abdominal or back pain.

7
The presence of UTI should be suspected in all infants and young children with unexplained fever and in patients of all ages with fever and congenital anomalies of the urinary tract.

8
LABORATORY AND IMAGING STUDIES The diagnosis of UTI requires a culture of the urine. Urine samples for urinalysis should be examined promptly (within 20 minutes) or refrigerated until culrured.
 or refrigerated until culrured..")
9
Urine obtained by midstream, clean-catch technique (for older children and adolescents) is considered significant with bacterial growth of a single organism of more than 100,000 colony forming units (CFU)/mL. Urine obtained by catheterization is considered significant with bacterial growth of more than 10,000 CFU/mL. Urine obtained by suprapubic aspiration is considered significant bacterial growth of more than 1000 CFU/nL. Perineal bags for urine collection are prone to contamination and are not recommended for urine collection for culture.

10
Urinalysis Pyuria (leukocyturia of >10 white blood cells [WBCs]/mm') suggests infection, but also is consistent with urethritis, vaginitis, nephrolithiasis, glomerulonephritis, and intersticial nephritis. Urinary dipstick tests that combine both the leukocyte esterase and nitrite have high sensitivity and specificity for detecting a UTI.
![Urinalysis Pyuria (leukocyturia of >10 white blood cells [WBCs]/mm ) suggests infection, but also is consistent with urethritis, vaginitis, nephrolithiasis, glomerulonephritis, and intersticial nephritis.](http://images.slideplayer.com/32/9944919/slides/slide_10.jpg "Urinary dipstick tests that combine both the leukocyte esterase and nitrite have high sensitivity and specificity for detecting a UTI..")
11
Imaging Ultrasonography, Voiding cystourethrogram (VCUG) Radionuclide cystography Renal nucleotide scans Computed tomography (CT) Magnetic resonance imaging (MRI)
 Radionuclide cystography Renal nucleotide scans Computed tomography (CT) Magnetic resonance imaging (MRI)")
12
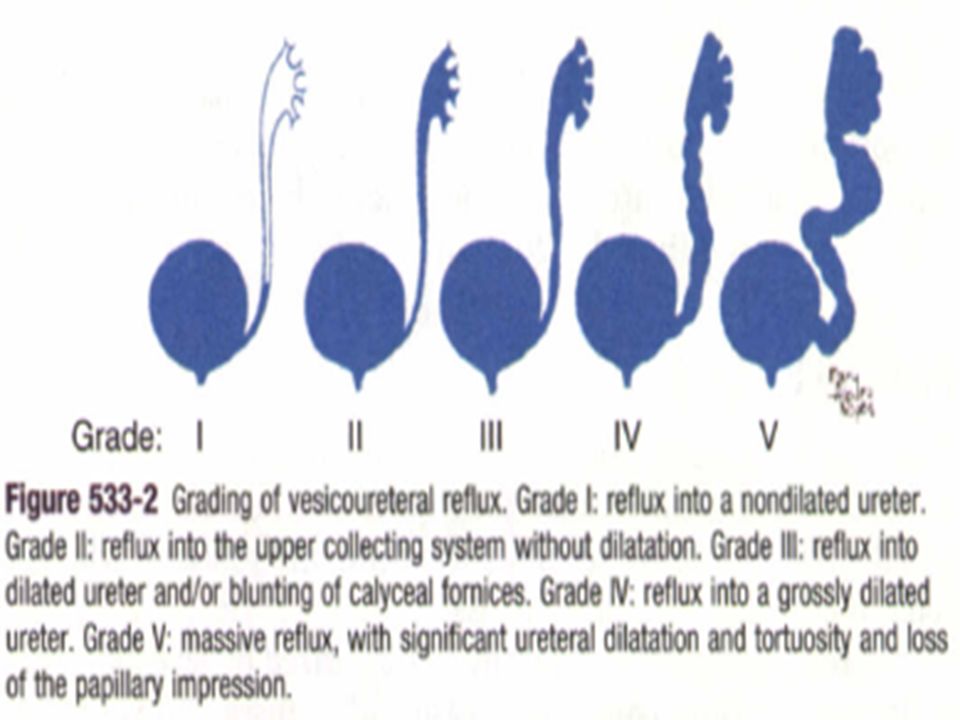
Ultrasound provides limited information about renal scarring and is performed to exclude an anatomic abnormaliry. VCUG is the best imaging study for determining the presence or absence of vesicoureteral reflux, which is ranked from grade I (ureter only) to grade V (complete gross dilation of the ureter and obliteration of caliceal and pelvic anatomy). A technetium- 99m DMSA scan can identify acute pyelonephriris and is most useful co define renal scarring as a late effect of UTI.
 to grade V (complete gross dilation of the ureter and obliteration of caliceal and pelvic anatomy). A technetium- 99m DMSA scan can identify acute pyelonephriris and is most useful co define renal scarring as a late effect of UTI..")
13
DIFFERENTIAL DIAGNOSIS UTI signs of sepsis seen in young children enteritis appendicitis mesenteric lymphadenitis pneumonia in older children Dysuria pinworm infection hypersensitiviry to soaps or derergents vaginitis Sexual abuse and infection

14
DIFFERENTIAL DIAGNOSIS The diagnosis of a UTI is confirmed by a positive urine culture, although this does not disringuish between upper tract and lower tract infection. Localizatron of a UTI is important because upper UTI is associated more frequently with bacteremia and with anatomic abnormalities than is uncomplicated cystitis.

15
DIFFERENTIAL DIAGNOSIS Upper tract infection high fever, Costovertebral tenderness high erythrocyte sedimentation rate (ESR) leukocytosis Bacteremia WBC casts, inability ro concentrare urine maximally, presence of antibody-coated bacteria detecred by immunofluorescence) and B2- microglobulin excretion lower tract infection Signs of cystitis low fever
 leukocytosis Bacteremia WBC casts, inability ro concentrare urine maximally, presence of antibody-coated bacteria detecred by immunofluorescence) and B2- microglobulin excretion lower tract infection Signs of cystitis low fever")
16
TREATMENT Empirical therapy For an older child who does not appear ill For a child with suspected UTI who appears toxic, appears dehydrated, or is unable to retain oral fluids Children with high fever or other manifestations of acute pyelonephritis

17
Duration of treatment Neonate :10 to 14 days with parenteral antibiotics Older children with acute cystitis : 7 to 14 days (5to7days) with an oral antibiotic Pyelonephritis : 7 to 14 days
 with an oral antibiotic Pyelonephritis : 7 to 14 days")
18
COMPLICATIONS AND PROGNOSIS Bacteremia occurs in 2o/oto 5o/o of episodes of pyelonephritis and is more likely in infants than in older children. Focal renal abscesses are uncommon complication. The relapse rate of UTI is approximately 25 o/o to 40o/o Most relapses occur within 2 to 3 weeks of treatment.

19
Follow-up urine cultures should be obtained 1 to 2 weeks after completing therapy to document sterility of the urine. Prophylactic antibiotics should be administered until the VCUG has been completed and the presence of reflux is known. TMP-SMZ (2 mglkg TMP, 10 mglkg SMZ) and nitrofurantoin (1 to 2 mglkg) given once daily at bedtime are recommended as prophylactic agents, which, in contrast to amoxicillin and cephalosporins, are associated with low rates of developing antibiotic resistance.
 and nitrofurantoin (1 to 2 mglkg) given once daily at bedtime are recommended as prophylactic agents, which, in contrast to amoxicillin and cephalosporins, are associated with low rates of developing antibiotic resistance..")
20
Clinical follow-up for at least 2 to 3 years is prudent, with repeat urine culture as indicated. Some experts recommend that follow-up urine cultures after recurrent cystitis or pyelonephritis are obtained monthly for 3 months, at 3-month intervals for 6 months, then yearly for 2 to 3 years.

21
PREVENTION Primary prevention is achieved by promoting good perineal hygiene and managing undedying risk factors for UTI, such as chronic constipation, encopresis, and daytime and nighttime urinary incontinence. Secondary prevention of UTI with antibiotic prophylaxis given once daily is directed toward preventing recurrent infections, although the impact of secondary prophylaxis to prevent renal scarring is unknown.

22
Acidification of the urine with cranberry iuice is not recommended as the sole means of preventing UTI in children at high risk.

23
Vesicoureteral reflux (VUR)
")
24
Vesicoureteral reflux (VUR) is the retrograde flow of urine from the bladder to the ureter or up to the kidney. Most VUR results from congenital incompetence of the ureterovesical (UV) junction that matures through early childhood. In a significant minority of children, structural UV abnormalities exist that never resolve. VUR may be familial; 30o/o to 4o o/o of siblings of a child with VUR also have VUR. VUR may also be secondary to distal bladder obstruction or other urinary tract anomalies.
 junction that matures through early childhood. In a significant minority of children, structural UV abnormalities exist that never resolve. VUR may be familial; 30o/o to 4o o/o of siblings of a child with VUR also have VUR. VUR may also be secondary to distal bladder obstruction or other urinary tract anomalies..")
25
VUR exposes the kidney to increased hydrodynamic pressure during voiding and increases the likelihood of renal infection due to incomplete emptying of the ureter and bladder. Reflux nephropathy refers to development and progression of renal scarring.

26
CLI N ICAL MANIFESTATIONS VUR is most often identified during radiologic evaluation following a UTI. The younger the patient with a UTI, the more likely VUR is present. No clinical signs are reliable in differentiating children with UTI with and without VUR.

27
DIAGNOSTIC STUDIES A voiding cystourethrogram (VCUG) or radionuclide cystogram (NCG) should be performed in all infants and children up to 6 years of age with a documented first UTI, regardless of gender.
 or radionuclide cystogram (NCG) should be performed in all infants and children up to 6 years of age with a documented first UTI, regardless of gender.")
30
TREATMENT The presence of VUR is generally an indication for longterm prophylactic antibiotic therapy (trimethoprimsulfamethoxazole or nitrofurantoin). Complications of reflux nephropathy are hypertension and chronic kidney disease( CKD).
..")
31
CKD is typically heralded by mild proteinuria and involves development of focal and segmental glomerulosclerosis and intersticial scarring. Indications for surgical repair of VUR are controversial and have been made more complex by the development of dextranomer/ hyaluronic acid copolymer (Deflux procedure), which appears to be a very successful minimally invasive correction of mild to moderate VUR.
, which appears to be a very successful minimally invasive correction of mild to moderate VUR..")
Similar presentations