Download presentation
Presentation is loading. Please wait.

1
D ENTAL C ARIES Prepared by: Dr. karam Ahmed MSc. in Operative dentistry

2
Dental caries: is defined as a microbiological disease of the hard structure of teeth, which results in localized demineralization of the inorganic portion and destruction of the organic substances of the tooth. Dental Caries

4
1. Tooth (Host) a. Variation in morphology b. Composition c. Position LOCAL FACTORS AFFECTING THE INCIDENCE OF CARIES

5
2. Environmental factor A- Saliva i. Composition ii. Quantity iii. pH iv. Viscosity v. Antibacterial factors

6
B- DIET i.Physical factors ii. Local factors Carbohydrate content—presence of refined cariogenic carbohydrate particles on the tooth surface Fluoride content Etiolog of Dental Caries

7
C- Microorganisms Most commonly seen microorganisms associated with caries are Streptococcus mutans and Lactobacillus. These bacteria are called acidogenic because they produce acid from carbohydrates. The acids diffuse in to enamel or dentin and dissolve them Enamel and dentin are made of million tiny crystals which are break down inside the tooth by these acid.( Demineralization ). 3.TIME PERIOD
. 3.TIME PERIOD.")
8
Etiology of Dental Caries Diet Caries Bacteria Time Susceptible Surface (Host) Possible interventions Reduce intake of cariogenic sugars Particularly sucrose Possible interventions Avoid frequent sucrose intake (snacking) Stimulate salivary flow + sugar clearance Possible interventions Reduce Strep. mutans numbers by: Reduction in sugar intake Active or passive immunization Possible interventions Water + other types of Fluoridation Prevention during post- eruptive maturation Fissure sealing Properly contured restorations

9
New Theories of dental caries (1) Acidogenic Theory (2) Proteolytic Theory (3) Proteolysis-chelation Theory Etiology of Dental Caries
 Acidogenic Theory (2) Proteolytic Theory (3) Proteolysis-chelation Theory Etiology of Dental Caries")
10
(1) Acidogenic/Chemoparasitic Theory 1890 WD Miller dental decay is a chemoparasitic process consisting of 2 stages decalcification of enamel results in total destruction Old Theories New Theories (Exogenous Theory)
 Acidogenic/Chemoparasitic Theory 1890 WD Miller dental decay is a chemoparasitic process consisting of 2 stages decalcification of enamel results in total destruction Old Theories New Theories (Exogenous Theory)")
11
(1) Acidogenic/Chemoparasitic Theory decalcification of dentin as a preliminary stage followed by dissolution of softened residue Old Theories New Theories (Exogenous Theory)
 Acidogenic/Chemoparasitic Theory decalcification of dentin as a preliminary stage followed by dissolution of softened residue Old Theories New Theories (Exogenous Theory)")
12
(1) Acidogenic/Chemoparasitic Theory following factors cause decay: (1) Role of carbohydrates (2) Role of microorganisms (3) Role of acids (4) Role of dental plaque Old Theories New Theories (Exogenous Theory)
 Acidogenic/Chemoparasitic Theory following factors cause decay: (1) Role of carbohydrates (2) Role of microorganisms (3) Role of acids (4) Role of dental plaque Old Theories New Theories (Exogenous Theory)")
13
(1) Role of carbohydrates food substances act as substrate for microorganisms of dental plaque various carbohydrates have been examined for cariogenic potential Old Theories (1)Acidogenic/ Chemoparasitic Theory
 Role of carbohydrates food substances act as substrate for microorganisms of dental plaque various carbohydrates have been examined for cariogenic potential Old Theories (1)Acidogenic/ Chemoparasitic Theory")
14
(1) Role of carbohydrates cariogenicity of carbohydrate varies with: (1) frequency of ingestion (2) physical form (3) chemical composition (4) route of administration (5) presence of other food constituents Old Theories (1)Acidogenic/ Chemoparasitic Theory
 Role of carbohydrates cariogenicity of carbohydrate varies with: (1) frequency of ingestion (2) physical form (3) chemical composition (4) route of administration (5) presence of other food constituents Old Theories (1)Acidogenic/ Chemoparasitic Theory")
15
(1) Role of carbohydrates (1) frequency of ingestion taken repeatedly in between two major meals provides constant supply of carbohydrate to plaque bacteria for fermentation + production of acids Old Theories (1)Acidogenic/ Chemoparasitic Theory
 Role of carbohydrates (1) frequency of ingestion taken repeatedly in between two major meals provides constant supply of carbohydrate to plaque bacteria for fermentation + production of acids Old Theories (1)Acidogenic/ Chemoparasitic Theory")
16
(1) Role of carbohydrates (2) physical form sticky solid carbohydrates Old Theories (1)Acidogenic/ Chemoparasitic Theory
 Role of carbohydrates (2) physical form sticky solid carbohydrates Old Theories (1)Acidogenic/ Chemoparasitic Theory")
17
(1) Role of carbohydrates (3) chemical composition in the form of glucose, sucrose + fructose due to low molecular weight rapidly diffuse into plaque make themselves easily available for fermentation by plaque bacteria Old Theories (1)Acidogenic/ Chemoparasitic Theory
 Role of carbohydrates (3) chemical composition in the form of glucose, sucrose + fructose due to low molecular weight rapidly diffuse into plaque make themselves easily available for fermentation by plaque bacteria Old Theories (1)Acidogenic/ Chemoparasitic Theory")
18
(1) Role of carbohydrates (4) Route of administration oral intake of sticky food (1)Acidogenic/ Chemoparasitic Theory
 Role of carbohydrates (4) Route of administration oral intake of sticky food (1)Acidogenic/ Chemoparasitic Theory")
19
(1) Role of carbohydrates (5) Presence of other food constituents refined pure carbohydrates more caries producing (1)Acidogenic/ Chemoparasitic Theory
 Role of carbohydrates (5) Presence of other food constituents refined pure carbohydrates more caries producing (1)Acidogenic/ Chemoparasitic Theory")
20
(2) Role of microorganisms caused by acid resulting from action of microorganisms on carbohydrates (1)Acidogenic/ Chemoparasitic Theory
 Role of microorganisms caused by acid resulting from action of microorganisms on carbohydrates (1)Acidogenic/ Chemoparasitic Theory")
21
(2) Role of microorganisms Initiation of Dental Caries Progression of Dental Caries Streptococci S. mutans S. milleri S. mitior S. sanguis S. salivaris Streptococcal species: Streptoccal species in deep dentinal caries and root caries Lactobacilli L. acidophillus L. casei Lactobacilli in dentin L. acidophillus L. casei Actinomycoses A. viscosus A. naeslundii Actinomycoses A. Israeli A. odontolyticus (1)Acidogenic/ Chemoparasitic Theory
Acidogenic/ Chemoparasitic Theory.")
22
(2) Role of microorganisms S. mutans has been proved for the initiation of caries (1)Acidogenic/ Chemoparasitic Theory
Acidogenic/ Chemoparasitic Theory.")
23
(3) Role of acids play most important role in pathogenesis of dental caries pH 5.5 is called critical pH below this pH demineralization of tooth substance begins (1)Acidogenic/ Chemoparasitic Theory
 Role of acids play most important role in pathogenesis of dental caries pH 5.5 is called critical pH below this pH demineralization of tooth substance begins (1)Acidogenic/ Chemoparasitic Theory")
24
(4) Role of Dental Plaque found on uncleaned tooth surfaces appear as tenacious, thin film may accumulate within 24-48 hours (1)Acidogenic/ Chemoparasitic Theory
 Role of Dental Plaque found on uncleaned tooth surfaces appear as tenacious, thin film may accumulate within hours (1)Acidogenic/ Chemoparasitic Theory")
25
(2) Proteolytic Theory proteolysis of the organic components of tooth as an initial process than actual demineralization + dissolution of inorganic substances Old Theories New Theories (Exogenous Theory)
 Proteolytic Theory proteolysis of the organic components of tooth as an initial process than actual demineralization + dissolution of inorganic substances Old Theories New Theories (Exogenous Theory)")
26
(2) Proteolytic Theory proposed that enamel lamellae or rod sheath (proteins) may be lysed which means proteolysis as first event in further progression of bacterial invasion + demineralization carious lesions Old Theories New Theories (Exogenous Theory)
 Proteolytic Theory proposed that enamel lamellae or rod sheath (proteins) may be lysed which means proteolysis as first event in further progression of bacterial invasion + demineralization carious lesions Old Theories New Theories (Exogenous Theory)")
27
(3) Proteolysis Chelation Theory suggests that caries is caused by simultaneous events of proteolysis + chelation proteolysis destruction of organic portion of tooth by proteolytic microorganisms Old Theories New Theories (Exogenous Theory)
 Proteolysis Chelation Theory suggests that caries is caused by simultaneous events of proteolysis + chelation proteolysis destruction of organic portion of tooth by proteolytic microorganisms Old Theories New Theories (Exogenous Theory)")
28
(3) Proteolysis Chelation Theory chelation removal of calcium by forming soluble chelates oral bacteria attack organic component of enamel (proteolysis) breakdown products have chelating ability and this dissolves tooth minerals Old Theories New Theories (Exogenous Theory)
 Proteolysis Chelation Theory chelation removal of calcium by forming soluble chelates oral bacteria attack organic component of enamel (proteolysis) breakdown products have chelating ability and this dissolves tooth minerals Old Theories New Theories (Exogenous Theory)")
29
(1) Depending on nature of attack (2) Depending on progression of caries (3) Depending on surfaces involved (4) Based on direction of attack (5) Based on number of surfaces involved Old Theories Classification
 Depending on nature of attack (2) Depending on progression of caries (3) Depending on surfaces involved (4) Based on direction of attack (5) Based on number of surfaces involved Old Theories Classification")
30
(6) GV Black Classification based on treatment and restoration design (7) Based on location of lesion (8) Based on tissue involved Old Theories Classification
 GV Black Classification based on treatment and restoration design (7) Based on location of lesion (8) Based on tissue involved Old Theories Classification")
31
Primary Caries incipient; initial first attack on tooth surface Secondary Caries recurrent occurs on margins or walls of existing restorations Old Theories (1) Nature of Attack
 Nature of Attack")
32
Acute rapidly invading process involves several teeth lesions are soft + light colored Old Theories (2) Progression of Caries
 Progression of Caries")
33
Acute usually pulp is involved at early stage Rampant caries Nursing bottle caries Radiation caries Old Theories (2) Progression of Caries
 Progression of Caries")
34
Chronic lesions are long standing fewer in number Old Theories (2) Progression of Caries
 Progression of Caries")
35
Pit and fissure Smooth surface caries Old Theories (3) Surfaces involved
 Surfaces involved")
36
Forward Caries proceeds from enamel to dentin lesion is triangle in shaped with base of triangle at enamel surface + apex towards dentin in pits + fissures base is at DEJ + apex is in the pit Old Theories (4) Direction of caries attack
 Direction of caries attack")
37
Backward Caries proceeds from DEJ towards enamel surface also triangle shaped with base at DEJ + apex towards enamel surface Old Theories (4) Direction of caries attack
 Direction of caries attack")
38
Simple only one surface is involved by caries Compound 2 surfaces are involved Complex more than 3 surfaces involved Old Theories (5) Number of Surfaces involved
 Number of Surfaces involved")
39
Class I begin in pits, fissures + defective grooves seen in occlusal surface occlusal two-thirds of molars lingual pits of incisors Old Theories (6) GV Black Classification
 GV Black Classification")
40
Class II lesions seen on proximal aspects of molars + premolars Old Theories (6) GV Black Classification
 GV Black Classification")
41
Class III lesions involving proximal aspects of incisors do not involve or necessitate removal of incisal edge Old Theories (6) GV Black Classification
 GV Black Classification")
42
Class IV lesions involving proximal aspects of incisors involve or require removal of incisal edge Old Theories (6) GV Black Classification
 GV Black Classification")
43
Class V lesions present on gingival third of all teeth Old Theories (6) GV Black Classification
 GV Black Classification")
44
Class VI lesions found on incisal edges + cusp tips Old Theories (6) GV Black Classification
 GV Black Classification")
45
Pit and Fissure caries Occlusal Buccal or lingual pit Smooth surface caries Proximal Buccal or Lingual surface Root caries Old Theories (7) Location of the lesion
 Location of the lesion")
46
Enamel Caries Dentinal Caries Cemental Caries Old Theories (8) Tissue involved
 Tissue involved")
47
Senile Caries caries associated with aging almost exclusively seen on root surface Residual Caries not removed during restorative procedure Classification

48
Interproximal Caries opaque chalky region (white spot) some cases yellow or brown pigment area spots are generally located on outer surface of enamel between contact point + height of free gingival margin Clinical Features: Smooth Surface Caries
 some cases yellow or brown pigment area spots are generally located on outer surface of enamel between contact point + height of free gingival margin Clinical Features: Smooth Surface Caries")
49
Interproximal Caries as caries penetrates enamel, enamel surrounding the lesion assumes bluish white appearance usally apparent as laterally spreading caries at DEJ Clinical Features: Smooth Surface Caries

50
Interproximal Caries common for proximal caries to extend both bucally + lingually Clinical Features: Smooth Surface Caries

51
Clinical Features: usually extends from area opposite gingival crest occlusally to convexity of tooth surface extends laterally towards proximal surfaces Cervical, Buccal, Lingual or Palatal Caries

52
Clinical Features: usually occurs on cervical area typical cervical lesion is a crescent shaped cavity beginning as slightly roughened chalky area gradually becomes excavated Cervical, Buccal, Lingual or Palatal Caries

53
Clinical Features: appears brown or black feel slightly soft catch a fine explorer point Pit and Fissure Caries

54
Clinical Features: enamel bordering the pit and fissure may appear opaque as it becomes bluish white undermined Pit and Fissure Caries

55
Clinical Features: lateral spread of caries at DEJ as well as penetration into dentin along dentinal tubules may be extensive without fracturing away overhanging enamel there may be large carious lesion with only a tiny point of opening Pit and Fissure Caries

56
also known as cemental caries involves both dentin + cementum in number of people exhibiting gingival recession with clinical exposure of cemental surface Root Caries

57
Clinical Features: slowly progressing chronic lesion usually found in mandibular molar area + premolar region gingival recession is associated with root surface caries Root Caries

58
occurs immediately adjacent to restoration may be caused by inadequate extension of restoration was not able to excavate or removed well original carious lesion Recurrent Caries

59
Clinical Features: restoration with poor margins permitted leakage + entrance of both bacteria + substrate Recurrent Caries

60
Etiology: due to nursing bottle containing milk or milk formula, fruit juice or sweetened water sometimes it occurs due to sugar or honey-sweetened pacifier Nursing Bottle Caries

61
Pathogenesis: child is put on bed at afternoon nap time or at night with nursing bottle containing milk or a sugar containing beverage milk or sweetened liquid becomes pooled around maxillary anterior teeth Nursing Bottle Caries

62
Pathogenesis: carbohydrate containing liquid provide an excellent culture medium for acidogenic microorganisms Nursing Bottle Caries

63
Clinical Feature: prolonged feeding beyond usual time may result in early + rampant caries early carious involvement of maxillary anterior, maxillary + mandibular 1 st permanent molars, mandibular canines Nursing Bottle Caries

64
Clinical Feature: carious process is so severe that only root stumps remain Nursing Bottle Caries

65
Prevention: parent should start brushing the child teeth as soon as they erupt in oral cavity discontinue bottle feeding as soon as child can drink from a cup, at approximately 12-15 months of age Nursing Bottle Caries

66
suddenly appearing widespread resulting in early involvement of pulp Rampant Caries

67
Etiology: may be due to nutritional deficiency malnutrition emotional disturbances Rampant Caries

68
Clinical Features: occurs in children with poor dietary habits extensive inter-proximal + smooth surface caries Rampant Caries

69
Management: extensive dental care parent education Rampant Caries

70
Clinical Features: both deciduous + permanent are affected large open cavities brown-stained polished appearance + hard Arrested Caries

71
Restorative Treatment Tooth Brushing Mouth Rinsing Dental Floss Topical Fluoride Application (Pedo Patients) Pit and Fissure Sealants Prevention/Management of Dental Caries
 Pit and Fissure Sealants Prevention/Management of Dental Caries")
72
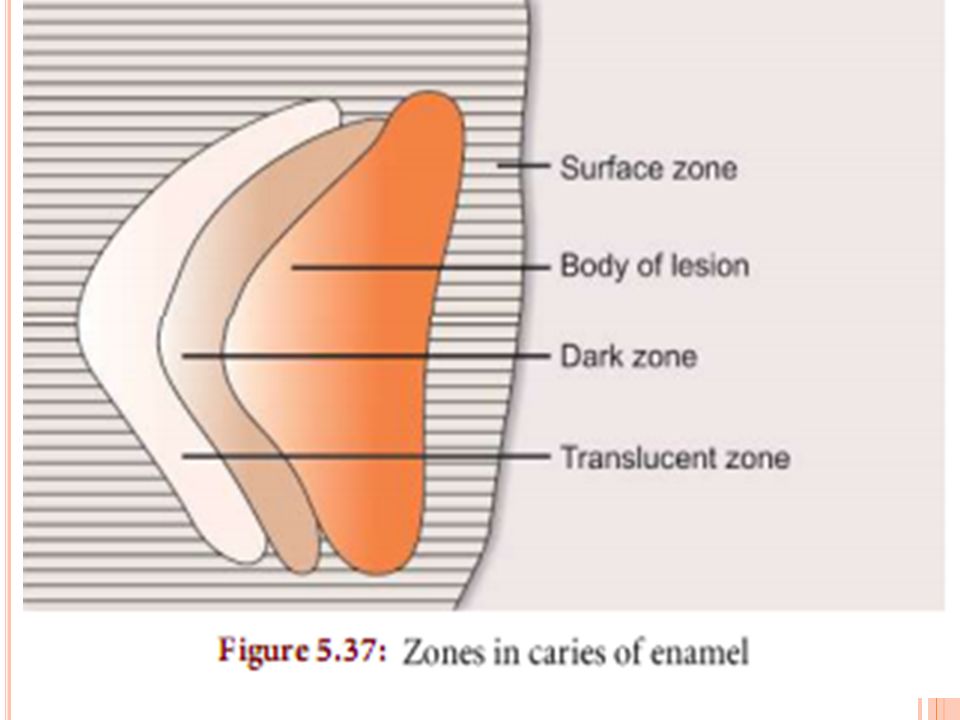
Zones in Enamel Caries Di ff erent zones are seen before complete disintegration of enamel. Early enamel lesion seen under polarized light reveals four distinct zones of mineralization. These zones begin from the dentinal side of the lesion.

74
Zone 1: Translucent zone – Represent the advancing front of the lesion – Ten times more porous than sound enamel – Not always present. Zone 2: Dark zone – It lies adjacent and superficial to the translucent zone – Usually present and thus referred as positive zone – Called dark zone because it does not transmit polarized light – Formed due to demineralization.

75
Zone 3: Body of the lesion – Largest portion of the incipient caries – Found between the surface and the dark zone – It is the area of greatest demineralization making it more porous. Zone 4: Surface zone – This zone is not or least a ff ected by caries – Greater resistance probably due to greater degree of mineralization and greater fluoride concentration – It is less than 5 percent porous – Its radiopacity is comparable to adjacent enamel.

76
2-Dentinal Caries Although caries of enamel is clearly a dynamic process, it is not a vital process because it does not defend itself from trauma. But since pulp and dentin are vital tissues, they are capable of defending. When enamel caries reaches the DEJ it spreads rapidly laterally because it is least resistant to caries.

77
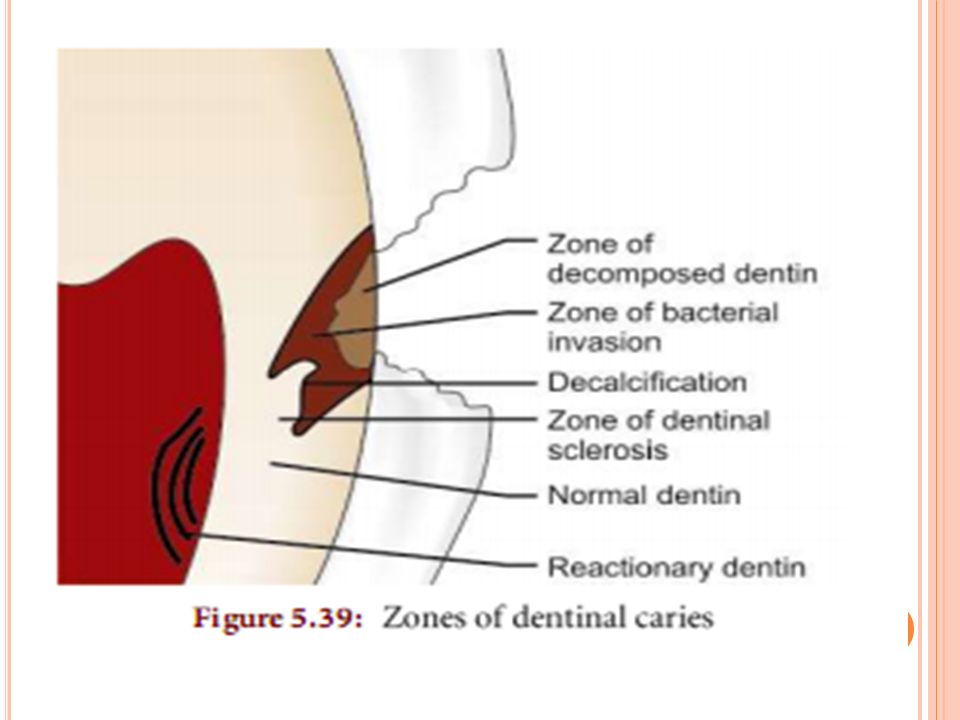
Zones of Dentinal Caries Five zones have been described in dentinal caries. These zones are clearly distinguished in chronic caries than in acute caries. These zones begin from the pulpal side :

79
Zone 1: Normal dentin – Zone of fatty degeneration of Tome’s fibers – Formed by degeneration of the odontoblastic process – Otherwise dentin is normal and produces sharp pain on stimulation. Zone 2: Zone of dentinal sclerosis – Intertubular dentin is demineralized – Dentinal sclerosis, i.e. deposition of calcium salts in dentinal tubules takes place – Damage to the odontoblastic zone process is apparent – There are no bacteria in this zone. Hence, this zone is capable of remineralization.

80
Zone 3: Zone of decalcification of dentin – Further demineralization of intertubular dentin lead to softer dentin. Zone 4: Zone of bacterial invasion – Widening and distortion of the dentinal tubules which are filled with bacteria – Dentin is not self-repairable, because of less mineral content and irreversibly denatured collagen –This zone should be removed during tooth preparation.

81
Zone 5: Zone of decomposed dentin due to acids and enzymes – Outermost zone – Consists of decomposed dentin filled with bacteria – It must be removed during tooth preparation.

82
The End

Similar presentations












>")






