Download presentation
Presentation is loading. Please wait.

1
Carcinoid GI tumors Sasha Rabotin

2
Carcinoid tumors 1888 - first described by Lubarsch 1907 - Oberndorfer coined the term Karzinoide to indicate the carcinoma-like appearance and the presumed lack of malignant potential

3
Epidemiology Rare 4.7 per 100,000 Men~women (4.97 versus 4.49/100,000) Median age at diagnosis (all NETs) - 63 Yao JC, Hassan M, et al. One hundred years after "carcinoid": epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol. 2008 Jun 20;26(18):3063-72.
:")
5
Distribution

6
Pathology Arise from enterochromaffin cells of the GI tract Stain with potassium chromate (chromaffin) due to presence of serotonin Well circumscribed Yellow cut surface (high lipid content) Grow slowly Usually submucosal
 due to presence of serotonin Well circumscribed Yellow cut surface (high lipid content) Grow slowly Usually submucosal")
10
Pathology After invasion to serosa: - mesenteric fibrosis - intestinal kinking - intermittent obstruction

11
Drawing illustrates a carcinoid tumor in the distal ileum. Radiological Society of North America et al. Radiographics 2007;27:236 ©2007 by Radiological Society of North America

12
Pathology Most ( ∼ 75%) GI carcinoid 2 cm 80-90% Primary tumors – small Mets (LNs, mesentery, liver) - large Multicentric 20-30% Synchronous adenocarcinoma 10-20% MEN1 10%
 GI carcinoid 2 cm 80-90% Primary tumors – small Mets (LNs, mesentery, liver) - large Multicentric 20-30% Synchronous adenocarcinoma 10-20% MEN1 10%")
13
Classification

14
Classification

15
Secretory Products

16
Clinical Manifestations Often asymptomatic Abdominal pain Obstructive (intuss/desmop)
")
17
Malignant Carcinoid Syndrome Rare Less than 10% of patients Usually in GI tumors (small bowel) Usually comes with liver metastases Signs: - flushing (80%) - diarrhea (76%) - hepatomegaly (71%) - cardiac lesions (41-71%) - asthma (25%)
 Usually comes with liver metastases Signs: - flushing (80%) - diarrhea (76%) - hepatomegaly (71%) - cardiac lesions (41-71%) - asthma (25%)")
18
Diagnosis Rarely diagnosed preoperatively 30%-50% of patients with small bowel Carcinoid are diagnosed at the of operation for: obstruction, ischemia or bleeding

19
Diagnosis Biochemical Testing ◦ 24 hour urinary excretion of 5-HIAA Sensitivity 75%, specificity up to 100% May not be useful for foregut carcinoids ◦ Chromogranin concentration in plasma Sensitive but not specific (many FPs) Used as a tumor marker: progression, recurrence
 Used as a tumor marker: progression, recurrence")
20
Diagnosis Barium studies

21
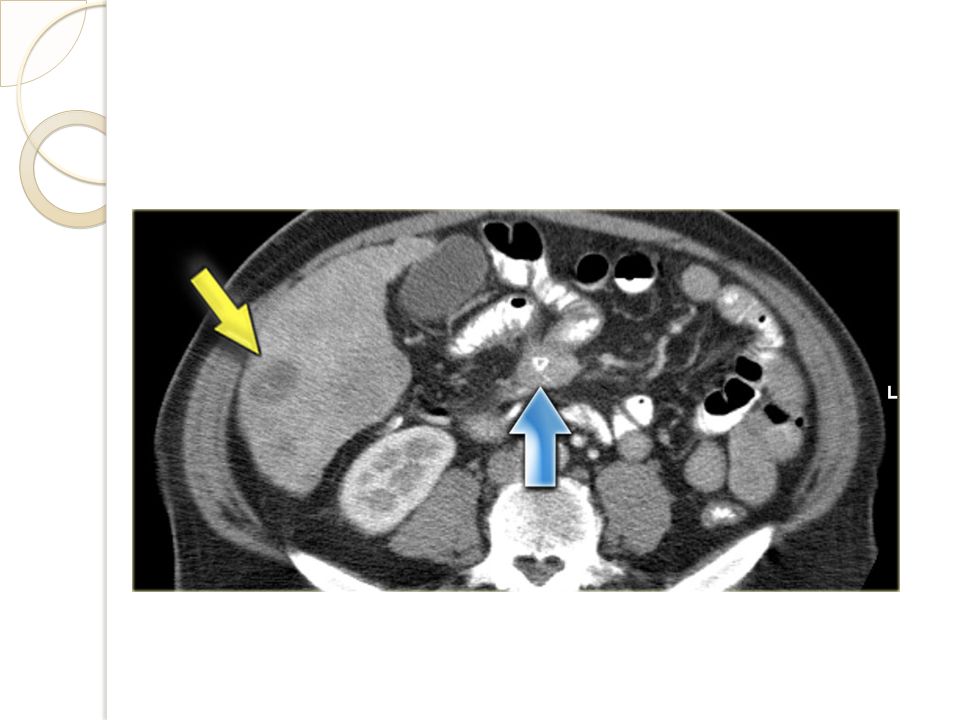
Diagnosis Imaging ◦ CT Primary tumors usually not seen Useful in detecting: 1. LN and hepatic metastases 2. bowel wall and mesenteric involvement ◦ MRI Sometimes better in demonstrating metastases ◦ US, Angiography Mesenteric/hepatic involvement

26
Diagnosis Imaging ◦ Somatostatin-receptor scintigraphy (OctreoScan) Used to evaluate metastatic spread 90% sensitivity ◦ PET/PET-CT May allow better sensitivity in the future
 Used to evaluate metastatic spread 90% sensitivity ◦ PET/PET-CT May allow better sensitivity in the future")
29
Treatment Multidisciplinary approach Surgery is the primary treatment for most patients Prophylactic – perioperative octreotide (subcutaneously) Carcinoid crisis – octreotide (IV bolus and infusion), antihistamine, hydrocortisone
 Carcinoid crisis – octreotide (IV bolus and infusion), antihistamine, hydrocortisone")
30
Treatment Appendix ◦ Smaller than 2 cm – simple appendectomy ◦ Larger than 2 cm or mesoappen. invasion – R. hemicolectomy controversial

31
Treatment Treatment Small bowel ◦ Smaller than 1 cm – segmental resection ◦ Larger than 1 cm or multiple tumors or regional LN mets – wide bowel and mesentery excision ◦ Terminal ileum – R. Hemicolectomy

32
Treatment Rectum ◦ Smaller than 1 cm and confined to mucosa or submucosa (T1) – local endoscopic excision ◦ 1-2 cm and confined – controversial ◦ Larger than 2 cm or invade m. propria or regional LN mets – LAR/APR

33
Treatment Octreotide – control symptoms IFNa – severe side effects Chemotherapy – limited success Receptor targeted therapy (studies) ◦ Radiolabeled somatostatin analogs ( 90 Y, 111 In- octerotide) ◦ 131 I-MIBG (up to 60% response) Metastatic disease – operate to relieve symptoms!
 ◦ Radiolabeled somatostatin analogs ( 90 Y, 111 In- octerotide) ◦ 131 I-MIBG (up to 60% response) Metastatic disease – operate to relieve symptoms!")
34
Prognosis Depends on: 1)Stage and site of origin 2)Residual disease 3)Differentiation and grade 4)Liver mets and heart involvement (presense of carcinoid syndrome) -worse prognosis Chromogranin A ◦ Independent predictor of an adverse prognosis
Stage and site of origin 2)Residual disease 3)Differentiation and grade 4)Liver mets and heart involvement (presense of carcinoid syndrome) -worse prognosis Chromogranin A ◦ Independent predictor of an adverse prognosis")
35
Prognosis

36
שאלות ?

37
Sabiston Textbook of Surgery: the Biological Basis of Modern Surgical Practice, 18Th Edition. Dries, David J. Current Surgical Therapy 10th Edition By Cameron UpToDate.com

Similar presentations
















 bowel habit change (-) bearing down sensation PMHx. hemorrhoidectomy,>")
 are derived from the diffuse neuroendocrine system, which is made up of.>")





: Jack Mbabuike Colon Adenocarcinoma (3): Joshua Gordon Basal Cell Carcinoma (1): Owen Dubowy Hepatocellular Carcinoma.>")




