Download presentation
Presentation is loading. Please wait.

1
Constitutes 10-40% of childhood blindness Dandona et al (India)-15% Rahi et al (India)-12% Tailor et al (USA)-15%
-15% Rahi et al (India)-12% Tailor et al (USA)-15%")
2
Study by Rahi et al (India, blind school) Unoperated cataract-40% Uncorrected aphakia & amblyopia -40% Unsuccessful surgery / post operative complications-20 %
 Unoperated cataract-40% Uncorrected aphakia & amblyopia -40% Unsuccessful surgery / post operative complications-20 %")
3
Lens structures include embryonal, fetal nuclei, cortex, lens epithelium & lens capsule Because of the layered development of the lens the timing of intrauterine insult can be judged by the location of the opacity Since lens and other anterior segment structure interrelated during development the abnormalities many times coexist

4
Only 60% of Bilateral cataract and 40% of Unilateral cataract can be established with specific etiology Others are undetermined

5
Congenital cataract Hereditary, genetic Metabolic Secondary Embryodisgenesis Etiology

6
Hereditary factors Non hereditary factors

7
Isolated hereditary congenital cataracts Cataracts associated with ocular disorder Cataract associated with autosomal syndrome Cataract associated with metabolic disorder

8
Autosomal dominant Most common Variable expressivity with high penetrance Different morphology in families and in individuals Autosomal recessive Less common responsible for metabolic disorders

9
X-linked inheritance - 3 forms Dense cataract in affected male Sutural cataract in carrier female Associated with microcornea and microphthalmos Cataract & dental anamolies ( Nancy Horan syndrome)
")
10
New mutation (50%) Familial (8-23%) Dominant & recessive Chromosomal trisomy 21,13,31,18,32, turners Systemic disease- lowes, Hallerman shreif, conradis, potters, sticklers,cockayne
 Familial (8-23%) Dominant & recessive Chromosomal trisomy 21,13,31,18,32, turners Systemic disease- lowes, Hallerman shreif, conradis, potters, sticklers,cockayne")
11
Pulverulent Anterior polar Posterior polar Nuclear Lamellar Sutural Blue dot cataract Total cataract

12
Inherited as autosomal dominant - 2 types Zonular pulverulent cataract (Coppock cataract) Central pulverulent cataract Typically bilateral & symmetrical Genes located at Chromosome 1q, 2q & 13q Mutated genes - connexin 50 & crystalins
 Central pulverulent cataract Typically bilateral & symmetrical Genes located at Chromosome 1q, 2q & 13q Mutated genes - connexin 50 & crystalins")
13
Inherited as autosomal dominant Opacity situated at the anterior pole of the lens Minimal effect on visual acuity Usually unilateral & stationary Gene located at chromosome 17p

14
Conical opacity with apex of the cone projecting into the anterior chamber Measures 2-2.5mm in diameter Usually bilateral Occurs sporaidically

15
Thinning and protrusion of center of the posterior capsule posteriorly Associated with posterior lenticular opacity Characterised by late onset

16
Small opacity at posterior capsule Inherited as autosomal dominant and recessive form Can cause gross visual impairment Can be associated with Mittindorf’s dot

17
Inherited as AD, AR or X-linked Opacification of central zone of lens specifically the region between the anterior & posterior sutures Usually bilateral with variable density gene located at chromosome 21 q Mutated gene - crystelins

18
Inherited as autosomal dominant Lamella of lenticular opacification sandwiched between clear nucleus and cortex Usually bilateral with variable density Gene located at chromosome 2q

19
Inherited as X-linked trait Opacities of lens sutures Seldom impairs vision Gene located at chromosome 17q

20
Autosomal dominant Multi coloured dot like opacities Genes located at 17q and 22q

21
Autosomal dominant Complete opacification of lens Usually bilateral and often begins as lamellar or nuclear cataract Gene located at chromosome 10q Mutated gene Pitx 3

22
Anterior segment disorders Aniridia Anterior segment dysgenesis Peter’s anomaly Microcornea Microphthalmia Coloboma Posterior lenticonus

24
Posterior segment disorder Mittindorf’s dot PHPV Retinitis pigmentosa Lebers congenital amaurosis Contd..

25
Chondrodysplasia punctata (AD, AR or x-linked) Hallerman -shrief syndrome (AD or AR) Myotonic dystrophy (AD) Neurofibromatosis type II (AD)
 Hallerman -shrief syndrome (AD or AR) Myotonic dystrophy (AD) Neurofibromatosis type II (AD)")
26
Stickler syndrome (AD) Bardt- Biedl syndromes (AR) Cockayane syndrome (AR) Usher disease (AR) X - linked - Alport’s syndrome Marfan’s syndrome Contd..
 Bardt- Biedl syndromes (AR) Cockayane syndrome (AR) Usher disease (AR) X - linked - Alport’s syndrome Marfan’s syndrome Contd..")
27
Galactosemia (AR) G6PD deficiency (AR) Hypocalcemia (X-linked) Lowe syndrome (X-linked) Fabry disease (X-linked)
 G6PD deficiency (AR) Hypocalcemia (X-linked) Lowe syndrome (X-linked) Fabry disease (X-linked)")
28
Down syndrome (Trisomy 21) Trisomy 10q, 13, 18 & 20p Turner syndrome (XO) Chromosome translocation 3:4, 2:14, 2:16
 Trisomy 10q, 13, 18 & 20p Turner syndrome (XO) Chromosome translocation 3:4, 2:14, 2:16")
29
Maternal illness Maternal drugs Maternal nutrition Prematurity Radiation Photocoagulation Steroid intake Trauma Acquired

30
Intrauterine infections caused by Rubella virus, Toxoplasmosis, Cytomegalo virus, Herpes Zoster and Simplex

31
Caused by the virus getting into the developing lens Characterised by central nuclear cataract usually bilateral Associated ocular findings are microcornea, glaucoma, keratitis and retinopathy Systemic associations are deafness and mental retardation

32
70% of cases were bilateral Mean age at 1st presentation 5.5 yrs 60% of children had a manifest squint 44% of children had nystagmus

33
More complex than in adults Amblyopia is imminent in infants Aphakic correction and amblyopia therapy more difficult than cataract itself Parents are often unable to attend for follow up

34
History Family history Antenatal and perinatal Birth weight Mile stones Onset- noticed by whom? What?

35
Ophthalmic examination Laboratory investigation Paediatrician evaluation

36
Visual acuity Fixation pattern Nystagmus Strabismus

37
Anterior segment Corneal diameter Size, location & density of lens opacities Diffuse light examination Red reflex test Slit lamp and Fundus Examination EUA if necessary

38
Try to ascertain the time of onset Rule out PHPV,retinoblastoma and injury Evaluate the motility USG for post segment pathology Good prognosis if there is good central fixation, no deviation, good convergence movement

39
Healthy child - No investigations Sick child TORCH for IgM Reducing sugars Other Investigations -SOS Routine investigations for general anesthesia

40
In all Syndromes In all Sick Children In all Mentally retarded children Ectopic and Spheroaphakic lenses Assessment for general anesthesia Genetic analysis if possible

41
General Considerations Small eye 100% PCO Increased inflammatory response

42
General considerations Low Scleral rigidity Elastic anterior capsule Post operative visual rehabilitation Long term follow up

43
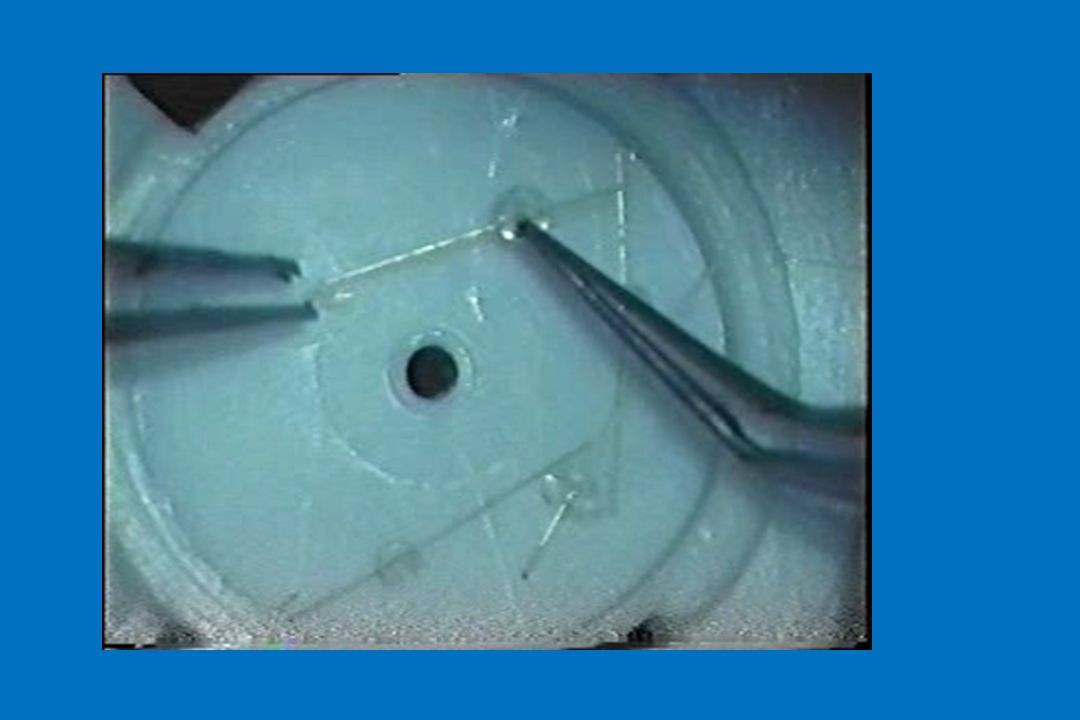
Basic Principles Nucleus is soft in nature Can be aspirated with Simcoe cannula, I & A tip of phaco machine or by Vitrectomy instrument No phacoemulsification or nucleus expression is necessary ICCE is contraindicated

44
Lensectomy with Anterior vitrectomy(AV) ECCE + PCCC + AV ECCE + PCCC + AV + IOL ECCE + IOL ECCE
 ECCE + PCCC + AV ECCE + PCCC + AV + IOL ECCE + IOL ECCE")
45
Choice of surgical procedure depends upon age, type of cataract, other ocular & systemic disabilities & socio- economic background of the parents

46
90% of the growth of eye ball is complete during the first 18 months after birth (Gordon Donzis)
")
47
Less than 6 Months Lensectomy + vitrectomy with posterior capsulectomy either central or total especially in sick infants,cat with other ocular anomalies, Membranous or in calcified type Other cases – ECCE with PCC Aphakic correction with spectacles or contact lenses as early as possible

48
6 months – 2 years ECCE with PCC /or Lensectomy with 4mm posterior capsulectomy depending upon the type of cataract Aphakic correction with spectacles or contact lenses Unilateral cataract; ECCE PCC with IOL

49
2 – 5 years ECCE with or without central posterior capsulectomy +/- Primary IOL Above 5 years ECCE with Primary IOL

50
Children < 2yrs Do biometry and undercorrect by 20% Or use axial length only Axial length(mm) Power (D) 1728.00 1827.00 1926.00 2024.00 2122.00 Children between 2-8 yrs Do biometry and undercorrect by 10%
 Power (D) Children between 2-8 yrs Do biometry and undercorrect by 10%")
51
Infant & toddler: within a week in equally dense cataracts Older child: If IOL is decided atleast 2 months after To watch the performance in both eyes and decide in unequally dense cataracts

52
Unilateral Cataract Prognosis not good Options are minimal Influencing factors on decision making manifold

53
Up to 2 years once in three months 2-5 years once in 6 months After 5 years 6 months / yearly

54
Visual acuity,Visual axis IOP, Fundus examination Strabismus and amblyopia

55
Depends upon Individualized approach Suitable technique Implanted lens power Careful postoperative monitoring Recognition of PCO & its management Overall co-operation from patient & parents

58
Usage of Intraocular lenses in infants Newer Viscoelastics Better intraocular lenses Dyes for visualisation of capsule Contact lenses Surgical techniques

60
Array Multifocal IOL

61
Normal PMMASquareedge IOL

62
AT-45 CrystaLens

63
To achieve emmetropia in extremely short eyes To avoid explantation of primary IOL’s in children

64
Morcher Iris diaphragm lens

65
Foldable acrylic IOL for implantation into the capsular bag through a microincision Optic diameter:5.5mm Length:11mm AcriSmart 48S Thin OptX

Similar presentations



1 RETINOBLASTOMA. 2 RETINOBLASTOMA It is the most common primary ocular malignancy of childhood. It formed 15% of all childhood cancers.>")



, FRCS (Glasg) Professor, Ophthalmology, KGMU.>")














