Download presentation
Presentation is loading. Please wait.

1
STD DR.Hanieh FaizMahdavi

2
Clinical manifestations and diagnosis of Chlamydia trachomatis infections

3
Chlamydia trachomatis is the most common bacterial cause of sexually transmitted genital infections.The majority of affected persons are asymptomatic, and thus provide an ongoing reservoir for infection. In infants born to mothers through an infected birth canal, conjunctivitis and pneumonia can occur. Moreover, both men and women can experience clinical syndromes due to infection at common epithelial sites, including the rectum and conjunctivae. Other types of C. trachomatis infection, including lymphogranuloma venereum and endemic trachoma, an ocular infection spread by direct contact and seen commonly in the developing world, may occur in both men and women.

4
In women, C. trachomatis most commonly affects the cervix. The majority of infected women are asymptomatic, although some may present with the typical findings of cervicitis, including vaginal discharge, abnormal vaginal bleeding, and purulent endocervical discharge on exam.

5
The majority (at least 85 percent) of women infected at the cervix have neither signs nor symptoms, which is the rationale for routine annual screening of young sexually active women. As an example, in a multinational study of high-risk women who were screened for genital chlamydial infection with polymerase chain reaction testing of vaginal swabs, four of five sites recorded symptoms in only 6 to 14 percent of those who developed a new infection within the first year of testing.When symptoms do occur, they are highly nonspecific, and can easily be confused with vaginitis or endometrial pathology: a change in vaginal discharge, intermenstrual vaginal bleeding, and post-coital bleeding. Similarly, abnormal exam findings are found in the minority of women with genital chlamydial infection, approximately 10 to 20 percent in some studies.When signs are present, they include classic findings of cervicitis: mucopurulent endocervical discharge,easily induced endocervical bleeding, or edematous ectopy.

6
The incubation period of symptomatic disease generally ranges from 7 to 14 days following infection. However, it is unclear how long those with asymptomatic disease may carry the infection. In a systematic review of ten studies of untreated, uncomplicated genital chlamydial infections, detection of chlamydia persisted over the short term (weeks to months after diagnosis) in 56 to 89 percent, and for at least one year in 46 to 57 percent.However, these studies did not record infection date nor did they evaluate for reinfection as opposed to persistent infection, thus limiting the understanding of duration of untreated chlamydial infection. Nevertheless, despite the possibility of spontaneous resolution,all women diagnosed with chlamydia should be treated to prevent further complications.
 in 56 to 89 percent, and for at least one year in 46 to 57 percent.However, these studies did not record infection date nor did they evaluate for reinfection as opposed to persistent infection, thus limiting the understanding of duration of untreated chlamydial infection. Nevertheless, despite the possibility of spontaneous resolution,all women diagnosed with chlamydia should be treated to prevent further complications..")
7
Dysuria-pyuria syndrome due to urethritis — Chlamydial infection of the female urethra typically occurs in a relatively small proportion (approximately 25 percent) of women with cervical infection. Most of these women do not report symptoms specific to the urethral tract, but some complain of typical symptoms of a urinary tract infection (UTI) such as frequency and dysuria. Urinalysis reveals pyuria, but bacteriuria is absent on dipstick analysis, and no organisms are seen on Gram stain or in bacterial culture. This combination of pyuria but no bacteriuria in a young, sexually active woman should prompt strong suspicion for chlamydial infection of the urethra. The differential diagnosis for such a presentation includes low-colony count urinary tract infection (eg, infection caused by Staphylococcus saprophyticus), or urethritis due to other sexually transmitted disease organisms, such as Neisseria gonorrhoeae or herpes simplex virus.
 such as frequency and dysuria. Urinalysis reveals pyuria, but bacteriuria is absent on dipstick analysis, and no organisms are seen on Gram stain or in bacterial culture. This combination of pyuria but no bacteriuria in a young, sexually active woman should prompt strong suspicion for chlamydial infection of the urethra. The differential diagnosis for such a presentation includes low-colony count urinary tract infection (eg, infection caused by Staphylococcus saprophyticus), or urethritis due to other sexually transmitted disease organisms, such as Neisseria gonorrhoeae or herpes simplex virus..")
8
The most concerning complication of untreated cervical chlamydial infection is pelvic inflammatory disease, which in turn can lead to infertility, ectopic pregnancy, or chronic pelvic pain

9
Pelvic inflammatory disease — C. trachomatis can ascend to the upper reproductive tract, where pelvic inflammatory disease (PID) can result. In some studies of women presenting to sexually transmitted disease clinics, 2 to 4.5 percent developed clinical PID in the two weeks between diagnosis of chlamydia infection and follow-up.One small study of 20 women with N. gonorrhoeae and C. trachomatis coinfection who were given antibiotics that were ineffective against chlamydia found a 30 percent incidence of PID after seven weeks.In contrast, studies of lower risk women have found no cases of clinical PID after a year of untreated chlamydial infection.These studies likely underestimate the incidence of PID in chlamydial infection, as many cases of PID may cause no symptoms and only be suspected years later in the setting of tubal infertility. When symptoms of PID are present, abdominal or pelvic pain are the most common, and their presence in the setting of cervicitis or a diagnosis of chlamydial infection should prompt strong suspicion for upper genital tract involvement. Signs of PID include cervical motion and uterine or adnexal tenderness. PID due to C. trachomatis is associated with higher rates of subsequent tubal infertility, ectopic pregnancy, and chronic pelvic pain when compared with PID caused by gonorrhea, which typically causes a more acute symptomatic presentation.
 can result. In some studies of women presenting to sexually transmitted disease clinics, 2 to 4.5 percent developed clinical PID in the two weeks between diagnosis of chlamydia infection and follow-up.One small study of 20 women with N. gonorrhoeae and C. trachomatis coinfection who were given antibiotics that were ineffective against chlamydia found a 30 percent incidence of PID after seven weeks.In contrast, studies of lower risk women have found no cases of clinical PID after a year of untreated chlamydial infection.These studies likely underestimate the incidence of PID in chlamydial infection, as many cases of PID may cause no symptoms and only be suspected years later in the setting of tubal infertility. When symptoms of PID are present, abdominal or pelvic pain are the most common, and their presence in the setting of cervicitis or a diagnosis of chlamydial infection should prompt strong suspicion for upper genital tract involvement. Signs of PID include cervical motion and uterine or adnexal tenderness. PID due to C. trachomatis is associated with higher rates of subsequent tubal infertility, ectopic pregnancy, and chronic pelvic pain when compared with PID caused by gonorrhea, which typically causes a more acute symptomatic presentation..")
10
Perihepatitis (Fitzhugh-Curtis syndrome) — Occasionally, patients with chlamydia infection develop perihepatitis, an inflammation of the liver capsule and adjacent peritoneal surfaces.Perihepatitis is more commonly seen in the setting of actual PID, occurring in 5 to up to 15 percent of cases. It is associated with right-upper quadrant pain or pleuritic pain, but there are typically no liver enzyme abnormalities. The pathogenesis of this entity is not fully understood but may involve either direct extension of infected material from the cul-de-sac through the peritoneum and/or lymphatics, or an immunologically mediated mechanism

11
The diagnostic test of choice for chlamydial infection of the genitourinary tract is nucleic acid amplification testing (NAAT) of vaginal swabs for women or urine for men. Many laboratories have also validated NAAT on rectal swabs to diagnose chlamydial proctitis. If non-NAAT-based testing is used for diagnosis or if adequate follow-up cannot be insured, patients with signs and symptoms consistent with chlamydia should be treated empirically before diagnostic test results return.

12
Any sexually active individual with signs and symptoms consistent with the clinical syndromes associated with chlamydia and patients with documented gonococcal infection should undergo diagnostic testing for C. trachomatis. Because the majority of chlamydial infections are asymptomatic, routine screening with NAAT should be offered to sexually active patients at high risk of infection and complications of chlamydia

13
N. gonorrhoeae not only causes similar clinical syndromes as C. trachomatis but also coexists in a significant proportion of patients with chlamydial infection. Thus, any testing for C. trachomatis should also prompt testing for N. gonorrhoeae.

14
The goals of treatment are to prevent complicated infections related to chlamydia (eg, pelvic inflammatory disease, infertility, ectopic pregnancy), decrease the risk of transmission to others, and attain resolution of symptoms. ●Complete care of the patient presenting with a chlamydial infection should include active antimicrobial therapy, directed or empiric therapy for concomitant gonococcal infection, if appropriate, counseling for HIV testing, counseling to return for persistent or recurrent symptoms, retesting to evaluate for recurrent infection, and treatment of sexual partners. ●Antimicrobial agents that have excellent activity against C. trachomatis include doxycycline (a tetracycline) and azithromycin (a macrolide).doxycyclinetetracycline azithromycin
 and azithromycin (a macrolide).doxycyclinetetracycline azithromycin.")
15
Uncomplicated genital chlamydial infections include urethritis in men and urethritis and cervicitis in women. For patients with uncomplicated genital chlamydial infections, we suggest directly observed azithromycin rather than unobserved azithromycin or doxycycline.,Azithromycin is given as a 1000 mg single dose. Doxycycline is dosed at 100 mg twice daily for seven days. Both are highly effective, but directly observed therapy ensures completion of the regimen. Patients who are prescribed doxycycline should be counseled on treatment adherence. Women should also have pregnancy testing since doxycycline is not recommended for pregnant women. azithromycin doxycycline

16
●Chlamydial and gonococcal infections may coexist in a significant percentage of community patients, which has a direct impact on treatment since first-line agents for chlamydia do not have activity against gonococci. Additional empiric therapy for gonorrhea should be based on a high suspicion of infection (eg, a positive Gram stain in men, a sexual partner recently diagnosed with gonorrhea). ●Empiric therapy for chlamydial infection should be offered to persons who present with symptoms suggestive of infection (cervicitis, pelvic inflammatory disease, urethritis). This is especially true if follow-up cannot be ensured and if relatively insensitive diagnostic testing is being used.
. ●Empiric therapy for chlamydial infection should be offered to persons who present with symptoms suggestive of infection (cervicitis, pelvic inflammatory disease, urethritis). This is especially true if follow-up cannot be ensured and if relatively insensitive diagnostic testing is being used..")
17
Doxycycline is contraindicated during pregnancy; the preferred agent is azithromycin. ●The treatment of HIV-infected patients with chlamydial infection is the same as in HIV-seronegative patients. ●A "test of cure" for assessing the adequacy of the prescribed antibiotic regimen is not routinely done except in the pregnant female or among those with persistent symptoms. In these circumstances, a test of cure can be performed at least three weeks after treatment is completed. ●Recently infected persons should have repeat testing for chlamydia approximately three to six months after treatment, regardless of whether patients believe their sex partners were treated, to rule out the possibility of reinfection. Doxycyclineazithromycin

21
Clinical manifestations and diagnosis of Neisseria gonorrhoeae infection

22
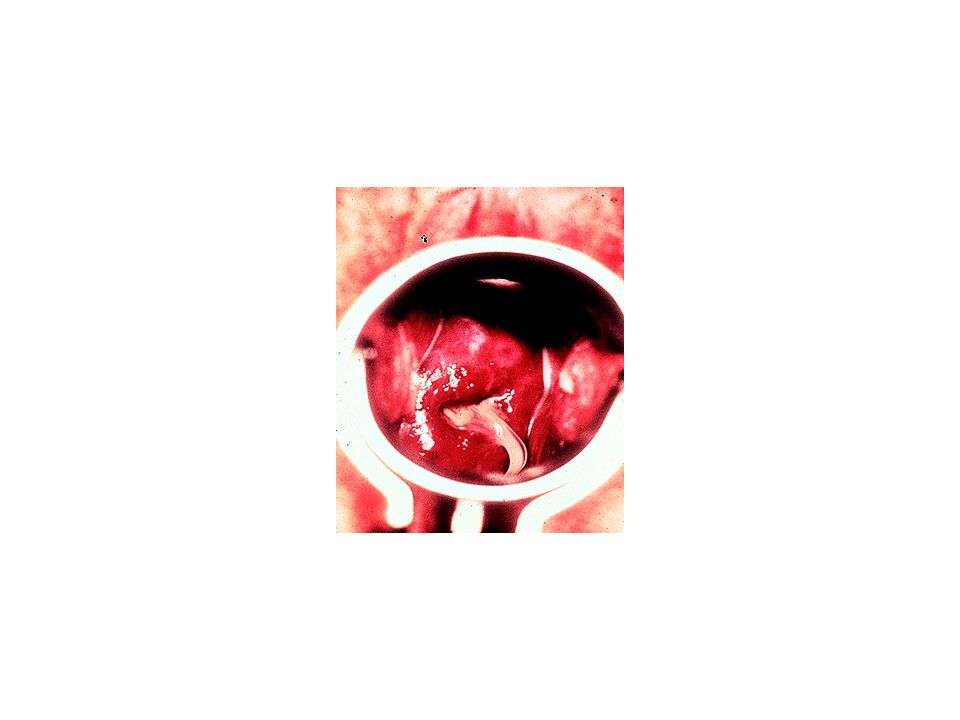
The gram-negative coccus N. gonorrhoeae causes sexually-transmitted urogenital and extragenital infections among men and women worldwide. ●Most genital gonococcal infections in women are asymptomatic. The cervix is the most commonly infected mucosal site in women. When symptomatic, gonococcal cervical infection can present with the typical findings of cervicitis, including vaginal pruritus and a mucopurulent cervical discharge.Some women may also have symptomatic involvement of the urethra (dysuria) or Bartholin’s glands (perilabial pain).Pelvic inflammatory disease is a complication of untreated urogenital gonococcal infection and can lead to infertility.
 or Bartholin’s glands (perilabial pain).Pelvic inflammatory disease is a complication of untreated urogenital gonococcal infection and can lead to infertility..")
23
Bacteremic spread of N. gonorrhoeae from the initial site of infection occurs in a small minority of patients. Disseminated infection often manifests as purulent arthritis or a triad of tenosynovitis, dermatitis, and polyarthralgia.

24
The clinical syndromes caused N. gonorrhoeae cannot be reliably distinguished from those caused by other pathogens on the basis of signs and symptoms alone. Other sexually transmitted pathogens, including Chlamydia trachomatis, Trichomonas vaginalis, and Mycoplasma genitalium, as well as herpes simplex virus (HSV) and syphilis, can cause similar symptoms.
 and syphilis, can cause similar symptoms..")
25
Nucleic acid amplification testing (NAAT) is the preferred test for the microbiologic diagnosis of N. gonorrhoeae because of its superior accuracy and use with various specimen types. For urogenital infections, vaginal swabs in women (clinician-collected and self-collected) and first- catch urine in men are the preferred specimens for NAAT. For extragenital infections, NAAT, used on pharyngeal and rectal swabs, is also the preferred test.
 and first- catch urine in men are the preferred specimens for NAAT. For extragenital infections, NAAT, used on pharyngeal and rectal swabs, is also the preferred test..")
26
Culture remains important for its ability to assess antibiotic susceptibilities of the isolate when resistance is suspected. Patients with confirmed gonococcal infection who have persistent symptoms after appropriate therapy with good adherence and lack of re-exposure should be tested for antibiotic resistant N. gonorrhoeae with culture and susceptibility testing. Culture requires endocervical, urethral, pharyngeal, or rectal swabs with specific handling.

27
N. gonorrhoeae not only causes similar clinical syndromes as C. trachomatis but also coexists in a significant proportion of patients with chlamydial infection. Thus, any testing for N. gonorrhoeae should also prompt testing for C. trachomatis.

28
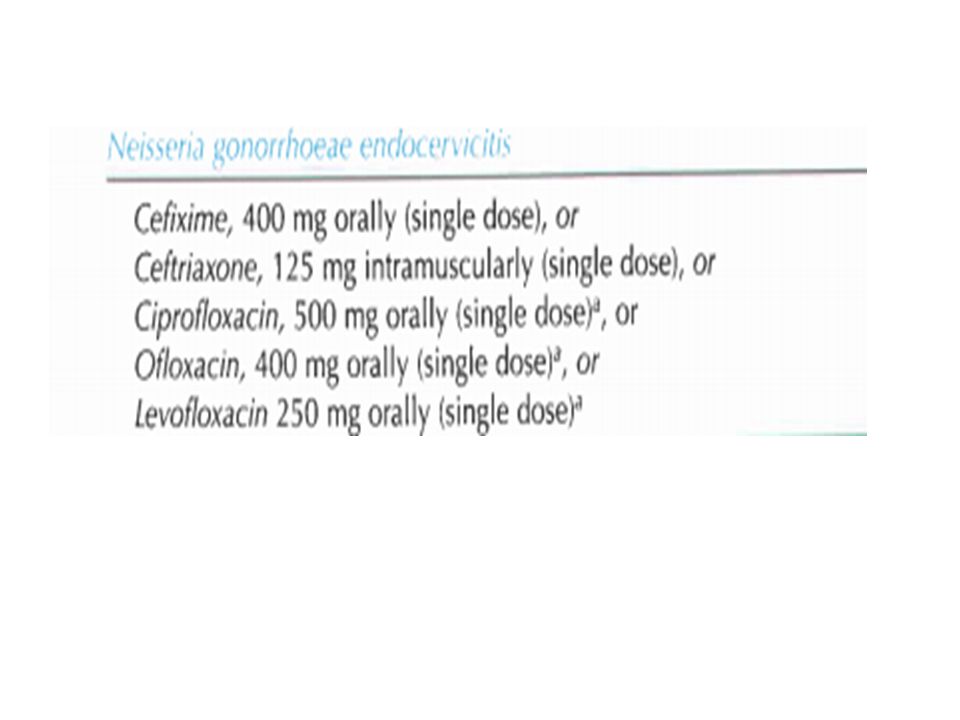
High microbiologic cure rates of gonococcal infection had been documented for multiple classes of drugs in the past. However, surveillance of resistance patterns in N. gonorrhoeae worldwide have demonstrated increased resistance to multiple classes of antibiotics including penicillins, tetracyclines, macrolides and fluoroquinolones. Of the cephalosporin class of drugs, ceftriaxone has the lowest rates of gonococcal drug resistance in epidemiologic surveys. In addition, ceftriaxone cures approximately 98 to 99 percent of pharyngeal and uncomplicated urogenital and anorectal infections. ●are being reportedA low but increasing proportion of isolates with decreased susceptibility to ceftriaxone worldwide. Because of this trend and the lack of new, effective antimicrobials in advanced product development, we suggest dual rather than monotherapy for the treatment of gonococcal infections.ceftriaxone

29
For the treatment of suspected or confirmed uncomplicated urogenital gonococcal infection, we recommend ceftriaxone as the first agent.For the second agent, we suggest azithromycin.Doxycycline is an alternate option. Ceftriaxone is administered as a single injection of a 250 mg dose at the point of care. Azithromycin is given orally as a single dose (1 g) while doxycycline is given twice daily for seven days (100 mg). Azithromycin and doxycycline also have activity against chlamydia, which is a common copathogen.ceftriaxoneazithromycinDoxycycline
 while doxycycline is given twice daily for seven days (100 mg). Azithromycin and doxycycline also have activity against chlamydia, which is a common copathogen.ceftriaxoneazithromycinDoxycycline.")
30
Pregnant women with uncomplicated gonorrheal infection should be treated with dual therapy with ceftriaxone plus azithromycin since doxycycline should be avoided during pregnancy.ceftriaxone azithromycindoxycycline

31
Treatment of sexual partners is essential for preventing reinfection and controlling the spread of N. gonorrhoeae. For sex partners of patients with documented gonococcal infection, we suggest not routinely employing expedited partner therapy.Instead, we prefer evaluation and management through traditional strategies of public health or patient notification. However, if a heterosexual partner cannot be evaluated and managed in this manner, delivery of oral cefixime and azithromycin through expedited partner therapy is a reasonable approach. cefiximeazithromycin

32
Patients who finish a recommended regimen for treatment of uncomplicated gonorrheal infections do not need to return for a test of cure.

34
Trichomoniasis

35
Trichomoniasis is caused by the protozoa Trichomonas vaginalis. It is virtually always sexually transmitted and can be identified in 70 percent of the male sexual partners of infected women. Coinfection with other sexually transmitted diseases (STDs) and bacterial vaginosis is common.
 and bacterial vaginosis is common..")
36
Clinical manifestations in women range from an asymptomatic carrier state to an acute, severe inflammatory disease. Signs and symptoms include a purulent, malodorous, thin discharge with associated burning, pruritus, dysuria, frequency, and dyspareunia. Men are often asymptomatic, but have developed urethritis.

38
Asymptomatic carriage can occur for prolonged periods of time, thus it is not necessarily possible to ascertain when or from whom the infection was acquired

39
The diagnosis of T. vaginalis is based on laboratory testing (motile trichomonads on wet mount,positive culture, positive nucleic acid amplification test (NAAT), or positive rapid antigen or nucleic acid probe test). None of the clinical features of trichomoniasis is sufficiently sensitive or specific to allow a diagnosis based upon signs and symptoms alone. We suggest NAAT (if available) in patients with suggestive clinical findings (eg, elevated vaginal pH, increased numbers of polymorphonuclear leukocytes but an absence of motile trichomonads and clue cells on wet mount) or when microscopy is unavailable or unreliable.
, or positive rapid antigen or nucleic acid probe test). None of the clinical features of trichomoniasis is sufficiently sensitive or specific to allow a diagnosis based upon signs and symptoms alone. We suggest NAAT (if available) in patients with suggestive clinical findings (eg, elevated vaginal pH, increased numbers of polymorphonuclear leukocytes but an absence of motile trichomonads and clue cells on wet mount) or when microscopy is unavailable or unreliable..")
40
If NAAT for trichomoniasis is not available, rapid antigen tests or DNA hybridization probes for diagnosis ofT. vaginalis are commercially available and can be used as an alternative to NAAT or culture. NAAT are the standard.

41
Treatment is indicated for both symptomatic and asymptomatic women and men. Treatment reduces the prevalence of T. vaginalis carriage in the population, relieves symptoms, and reduces the risk of sequelae (including acquisition/transmission of HIV). For nonpregnant women and their sex partners, we recommend a single oral dose of 2 grams of a 5- nitroimidazole drug (eg, metronidazole, tinidazole) compared with multi-dose regimens.Single dose therapy is more convenient and appears to be as effective as multiple dose therapy. Oral administration is more effective than topical administration.metronidazoletinidazole
. For nonpregnant women and their sex partners, we recommend a single oral dose of 2 grams of a 5- nitroimidazole drug (eg, metronidazole, tinidazole) compared with multi-dose regimens.Single dose therapy is more convenient and appears to be as effective as multiple dose therapy. Oral administration is more effective than topical administration.metronidazoletinidazole.")
42
Patients should be screened for other sexually transmitted infections

43
Although expedited partner therapy (EPT) is effective for treatment of Trichomonas infections, we prefer that sexual partners be evaluated so they can be screened for other sexually transmitted infections. However, EPT is reasonable if compliance is an issue

44
We recommend treating symptomatic pregnant women with confirmed T. vaginalis infections.In addition, we suggest treating asymptomatic pregnant women with confirmed infection.Metronidazole 2 g orally in a single dose is used in pregnancy. Alternate dosing with metronidazole 500 mg twice daily for five to seven days may be associated with less nausea and vomiting. Either regimen is acceptable.Metronidazole

45
For patients with refractory trichomoniasis, increasing the dose and duration of metronidazole or tinidazoleare the primary options. ●Patients should be instructed to avoid intercourse until they and their partners have completed treatment and are asymptomatic, which generally takes about a week..metronidazoletinidazole

46
●Women treated for a documented trichomonal infection are retested within three months following treatment regardless of whether they believe their sex partners were treated. Testing with NAAT can be done as soon as two weeks after completing treatment

47
Candida infections

48
The clinical manifestations of infection with Candida species range from local mucous membrane infections to widespread dissemination with multisystem organ failure. Although Candida are considered normal flora in the gastrointestinal and genitourinary tracts of humans, they have the propensity to invade and cause disease when an imbalance is created in the ecologic niche in which these organisms usually exist.

49
Candida is considered part of the normal vaginal flora, but overgrowth of the organism and penetration of superficial epithelial cells can result in vulvovaginitis. Candida albicans accounts for 80 to 92 percent of episodes of vulvovaginal candidiasis; Candida glabrata is the next most common species.

50
Vulvar pruritus is the dominant symptom. Vulvar burning, soreness, and irritation are common and may result in dysuria and dyspareunia. The vulva and vagina appear erythematous, and vulvar excoriation and fissures may be present. There is often little or no discharge; when present, it is classically white, thick, adherent, and clumpy (curd-like or cottage cheese-like) with no or minimal odor.
 with no or minimal odor..")
52
The diagnosis of vulvovaginal candidiasis is based on the presence of Candida on wet mount, Gram’s stain, or culture of vaginal discharge in a woman with characteristic clinical findings.

53
Culture is not necessary for diagnosis if microscopy shows yeast, but should be obtained in : Women with clinical features of vulvovaginal candidiasis, normal vaginal pH, and negative microscopy. Women with persistent or recurrent symptoms because many of these women have non-albicans infection resistant to azoles.

54
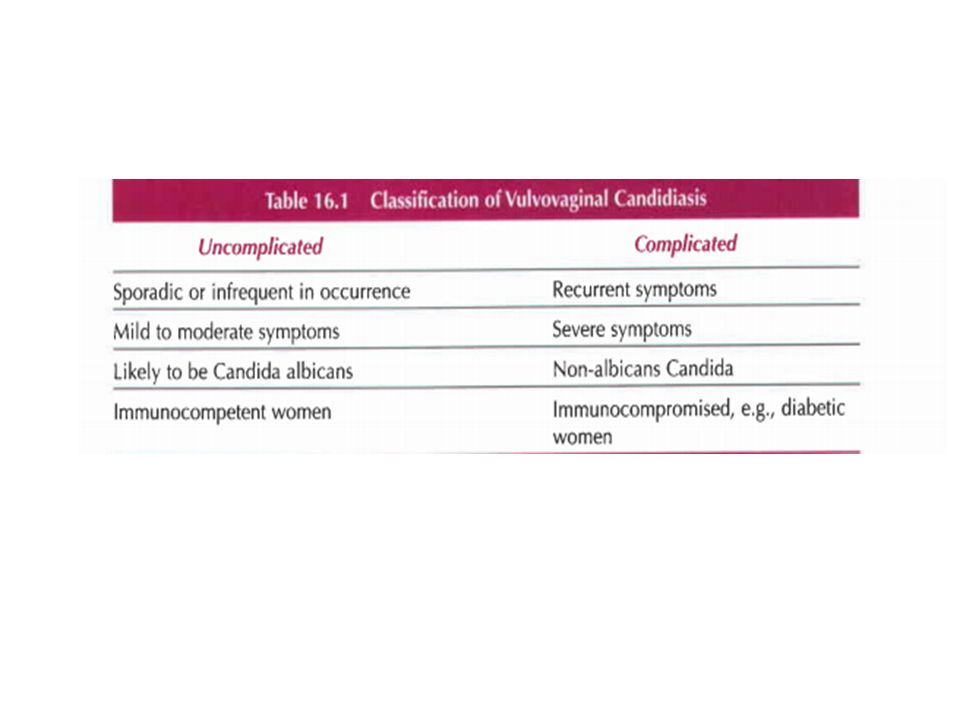
Treatment ●Treatment is indicated to relieve symptoms. Asymptomatic women and sexual partners do not require treatment. ●The treatment regimen is based on whether the woman has an uncomplicated infection (90 percent of patients) or complicated infection (10 percent of patients).
 or complicated infection (10 percent of patients)..")
55
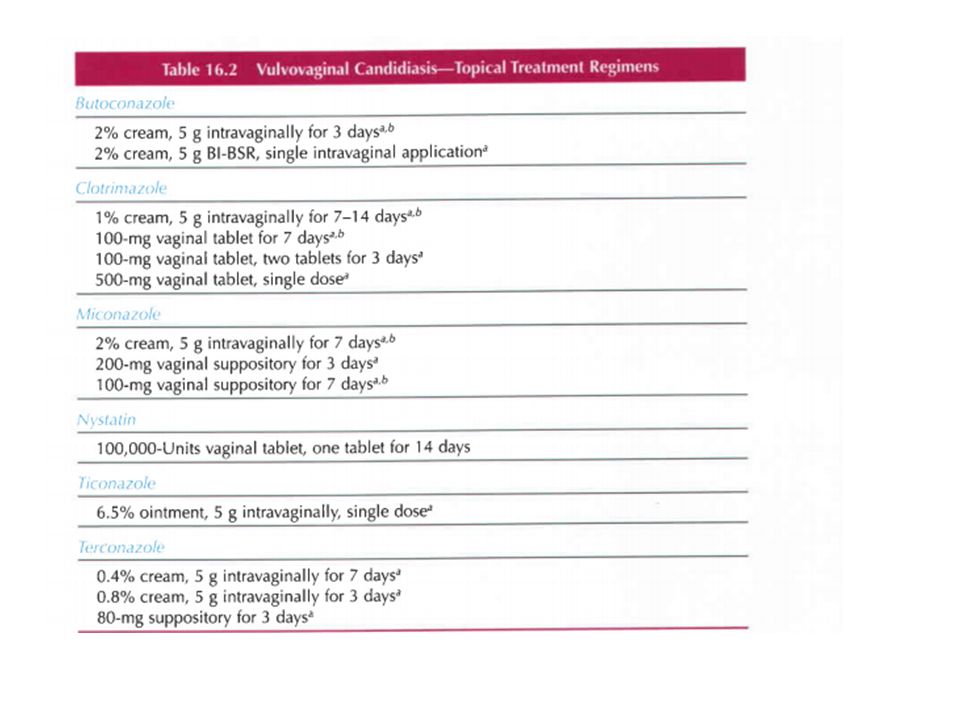
Uncomplicated infections — Oral and topical antimycotic drugs achieve comparable clinical cure rates, which are in excess of 80 percent in uncomplicated infection ●We suggest a single dose of oral fluconazole (150 mg) for treatment of uncomplicated infections rather than multidose and topical regimens fluconazole
 for treatment of uncomplicated infections rather than multidose and topical regimens fluconazole")
56
Complicated infections — Women with complicated infection require longer courses of therapy than women with uncomplicated infection. ●For women with severe symptoms, we suggest fluconazole (150 mg) in two sequential doses given three days apart rather than topical antimycotic agents.fluconazole ●For pregnant women, we suggest a topical imidazole (clotrimazole, miconazole) vaginally for seven days rather than a nystatin pessary or an oral azole.Case reports have described a pattern of birth defects (abnormalities of cranium, face, bones, and heart) after first trimester exposure to high dose oral azole therapy (400 to 800 mg/day) and cohort studies have reported conflicting data on risk of miscarriage. clotrimazolemiconazolenystatin
 in two sequential doses given three days apart rather than topical antimycotic agents.fluconazole ●For pregnant women, we suggest a topical imidazole (clotrimazole, miconazole) vaginally for seven days rather than a nystatin pessary or an oral azole.Case reports have described a pattern of birth defects (abnormalities of cranium, face, bones, and heart) after first trimester exposure to high dose oral azole therapy (400 to 800 mg/day) and cohort studies have reported conflicting data on risk of miscarriage. clotrimazolemiconazolenystatin.")
57
For women with recurrent vulvovaginitis (≥4 episodes/year), we suggest suppressive maintenance therapy rather than treatment of individual episodes.We prescribe initial induction therapy withfluconazole 150 mg every 72 hours for three doses, then maintenance fluconazole 150 mg once per week for six months. Women with recurrent infection should try to eliminate or reduce risk factors for infection. fluconazole

60
Bacterial vaginosis

61
Bacterial vaginosis (BV) is the most common cause of vaginitis in women of childbearing age. ●BV represents a complex change in the vaginal flora characterized by a reduction in concentration of the normally dominant hydrogen-peroxide producing lactobacilli and an increase in concentration of other organisms, particularly anaerobic and highly specific fastidious BV-associated bacteria. Vaginal wall biofilms, comprised predominantly of Gardnerella vaginalis, appear to play a role in pathogenesis.

62
PATHOGENESIS AND MICROBIOLOGY — Bacterial vaginosis (BV) represents a complex change in the vaginal flora characterized by a reduction in concentration of the normally dominant hydrogen-peroxide producing lactobacilli and an increase in concentration of other organisms, especially anaerobic gram negative rods.The major bacteria detected are Gardnerella vaginalis, Prevotella species, Porphyromonas species, Bacteroides species, Peptostreptococcus species, Mycoplasma hominis, Ureaplasma urealyticum, and Mobiluncus species.Fusobacterium species and Atopobium vaginae are also common. The mechanism by which the floral imbalance occurs and the role of sexual activity in the pathogenesis of BV are not clear, but formation of an epithelial biofilm containing G. vaginalis appears to play an important role. Hydrogen-peroxide producing lactobacilli appear to be important in preventing overgrowth of the anaerobes normally present in the vaginal flora. With the loss of lactobacilli, pH rises and massive overgrowth of vaginal anaerobes occurs. These anaerobes produce large amounts of proteolytic carboxylase enzymes, which break down vaginal peptides into a variety of amines that are volatile, malodorous, and associated with increased vaginal transudation and squamous epithelial cell exfoliation, resulting in the typical clinical features observed in patients with BV The rise in pH also facilitates adherence of G. vaginalis to the exfoliating epithelial cells.

63
RISK FACTORS — Sexual activity is a risk factor for bacterial vaginosis (BV), and most experts believe that BV does not occur in women who have never had vaginal intercourse.Epidemiologic studies are strongly supportive of sexual transmission of BV pathogens. In a systematic review and meta-analysis of 43 observational studies, sexual contact with new and multiple male and female partners was associated with an increased risk of BV, while condom use was associated with a decreased risk. Further, the presence of other sexually transmitted infections appears to be associated with an increased prevalence of BV. In a systematic review and meta- analysis of studies evaluating the association between BV infection and herpes simplex virus (HSV)-2 infection, women infected with HSV-2 had a 55 percent higher risk of BV infection compared with women who were HSV-2 uninfected.Similarly, a five-year prospective cohort study reported that BV was both more prevalent and more persistent among HIV-infected women compared with those without HIV.Conversely, bacterial vaginosis may also be a risk factor for HIV acquisition In addition to sexual and infectious risk factors, most studies indicate douching and cigarette smoking are risk factors for acquisition of BV among sexually active women.Although some degree of genetic susceptibility to BV is likely, no association between a gene polymorphism and BV has been established. Use of condoms and estrogen-containing contraceptives may be protective factors.
-2 infection, women infected with HSV-2 had a 55 percent higher risk of BV infection compared with women who were HSV-2 uninfected.Similarly, a five-year prospective cohort study reported that BV was both more prevalent and more persistent among HIV-infected women compared with those without HIV.Conversely, bacterial vaginosis may also be a risk factor for HIV acquisition In addition to sexual and infectious risk factors, most studies indicate douching and cigarette smoking are risk factors for acquisition of BV among sexually active women.Although some degree of genetic susceptibility to BV is likely, no association between a gene polymorphism and BV has been established. Use of condoms and estrogen-containing contraceptives may be protective factors..")
64
CONSEQUENCES ●Pregnant women with bacterial vaginosis (BV) are at higher risk of preterm delivery. ●BV is a cause of : Endometrial bacterial colonization Plasma-cell endometritis Postpartum fever Posthysterectomy vaginal cuff cellulitis Postabortal infection ●BV is a risk factor for human immunodeficiency virus (HIV) acquisition and transmission. ●BV is a risk factor for acquisition of herpes simplex virus type 2 (HSV-2), gonorrhea, chlamydia, and trichomonas infection.Although BV is more common among women with pelvic inflammatory disease (PID), it is not clear whether it is a causal factor or an independent risk factor for this disease. It has been hypothesized that the increased risk of acquisition of sexually transmitted infections in women with BV may be due to lack of hydrogen peroxide-producing lactobacilli in the vaginal flora of affected women; other factors associated with BV infection, such as local cytokine production, may also play a role.hydrogen peroxide ●BV may be a factor in development of precancerous cervical lesions. In a systematic review and meta- analysis of primarily cross-sectional studies, the risk of cervical intraepithelial neoplasia (CIN) or squamous intraepithelial lesions (SIL) was increased in women with BV (OR 1.51, 95% CI 1.24-1.83); however, there was considerable heterogeneity among these studies and both CIN 1 and low-grade SIL, which do not usually progress to cancer, were included as outcomes.BV appears conducive to the persistence of human papillomavirus (HPV) infection,which is necessary but not sufficient for development of high grade cervical lesions and cancer
 acquisition and transmission. ●BV is a risk factor for acquisition of herpes simplex virus type 2 (HSV-2), gonorrhea, chlamydia, and trichomonas infection.Although BV is more common among women with pelvic inflammatory disease (PID), it is not clear whether it is a causal factor or an independent risk factor for this disease. It has been hypothesized that the increased risk of acquisition of sexually transmitted infections in women with BV may be due to lack of hydrogen peroxide-producing lactobacilli in the vaginal flora of affected women; other factors associated with BV infection, such as local cytokine production, may also play a role.hydrogen peroxide ●BV may be a factor in development of precancerous cervical lesions. In a systematic review and meta- analysis of primarily cross-sectional studies, the risk of cervical intraepithelial neoplasia (CIN) or squamous intraepithelial lesions (SIL) was increased in women with BV (OR 1.51, 95% CI ); however, there was considerable heterogeneity among these studies and both CIN 1 and low-grade SIL, which do not usually progress to cancer, were included as outcomes.BV appears conducive to the persistence of human papillomavirus (HPV) infection,which is necessary but not sufficient for development of high grade cervical lesions and cancer.")
65
Approximately 50 to 75 percent of women with BV are asymptomatic. Those with symptoms often present with an off-white, thin, and homogeneous "fishy smelling" discharge that is more noticeable after coitus and during menses. ●Sequelae of BV can include an increased risk of preterm birth, plasma-cell endometritis, postpartum fever, post-hysterectomy vaginal cuff cellulitis, postabortal infection, pelvic inflammatory disease, and acquisition of other sexually transmitted infections.

66
CLINICAL FEATURES — Fifty to 75 percent of women with bacterial vaginosis (BV) are asymptomatic.Symptomatic women typically present with vaginal discharge and/or vaginal odor.The discharge is off-white, thin, and homogeneous; the odor is an unpleasant "fishy smell" that may be more noticeable after sexual intercourse and during menses. BV alone does not cause dysuria, dyspareunia, pruritus, burning, or vaginal inflammation (erythema, edema).The presence of these symptoms suggests mixed vaginitis Although BV does not involve the cervix, the disorder may be associated with acute cervicitis (endocervical mucopurulent discharge or easily induced cervical bleeding.
.The presence of these symptoms suggests mixed vaginitis Although BV does not involve the cervix, the disorder may be associated with acute cervicitis (endocervical mucopurulent discharge or easily induced cervical bleeding..")
67
Diagnosis ●When microscopy is available, the diagnosis of BV is based on the presence of at least three of the following four Amsel criteria Homogeneous, thin, grayish-white discharge that smoothly coats the vaginal walls Vaginal pH greater than 4.5 Positive whiff-amine test, defined as the presence of a fishy odor when 10 percent potassium hydroxide (KOH) is added to a sample of vaginal discharge Clue cells on saline wet mount, comprising at least 20 percent of epithelial cells ●If microscopy is not available, we suggest using physical examination, pH testing, whiff-amine test, and a commercial test using a DNA probe (eg, Affirm VP III) to make the diagnosis of BV. ●Vaginal culture is not useful.

68
TREATMENT — Bacterial vaginosis (BV) resolves spontaneously in up to one-third of nonpregnant and one- half of pregnant women.Treatment is indicated for relief of symptoms in women with symptomatic infection and to prevent postoperative infection in those with asymptomatic infection prior to abortion or hysterectomy. Treatment of BV may also reduce the risk of acquiring sexually transmitted diseases (STDs), including human immunodeficiency virus (HIV).For this reason, some experts support the concept of treating all women with BV regardless of presence or absence of symptoms; however, we agree with the United States Centers for Disease Control and Prevention (CDC) recommendations to not treat asymptomatic women. Asymptomatic pregnant women with previous preterm births may also benefit, but screening and treatment of these women is controversial
, including human immunodeficiency virus (HIV).For this reason, some experts support the concept of treating all women with BV regardless of presence or absence of symptoms; however, we agree with the United States Centers for Disease Control and Prevention (CDC) recommendations to not treat asymptomatic women. Asymptomatic pregnant women with previous preterm births may also benefit, but screening and treatment of these women is controversial.")
69
Treatment of nonpregnant women ●Treatment of symptomatic women with bacterial vaginosis is indicated to reduce vaginal discharge and odor. We recommend metronidazole or clindamycin. Options include:metronidazoleclindamycin Metronidazole 500 mg twice daily orally for seven daysMetronidazole Metronidazole gel 0.75 percent (5 grams containing 37.5 mg metronidazole) once daily vaginally for 5 daysMetronidazole Clindamycin 2% vaginal cream once daily at bedtime for seven daysClindamycin Clindamycin 300 mg twice per day orally for seven daysClindamycin Clindamycin 100 mg vaginal suppositories at bedtime for three daysClindamycin Clindamycin bioadhesive cream (Clindesse) 2% as a single vaginal dose of 5 grams of cream containing 100 mg of clindamycin phosphate.Clindamycin
 once daily vaginally for 5 daysMetronidazole Clindamycin 2% vaginal cream once daily at bedtime for seven daysClindamycin Clindamycin 300 mg twice per day orally for seven daysClindamycin Clindamycin 100 mg vaginal suppositories at bedtime for three daysClindamycin Clindamycin bioadhesive cream (Clindesse) 2% as a single vaginal dose of 5 grams of cream containing 100 mg of clindamycin phosphate.Clindamycin.")
70
●During therapy with metronidazole, alcohol should not be consumed. During therapy with clindamycin cream, latex condoms should not be used. ●We recommend not treating sexual partners of women with BV.●Approximately 30 percent of patients with an initial response to therapy have a recurrence of symptoms within three months and more than 50 percent experience a recurrence within 12 months. We treat symptomatic relapse with a longer course of therapy, using a different antibiotic than that used for the initial episode. For women who prefer preventive therapy instead of treatment of frequent episodes of BV, we suggest metronidazole or tinidazole orally for seven days; vaginal boric acid 600 mg is begun at the same time and continued for 21 days. Patients are seen for follow-up a day or two after their last boric acid dose; if they are in remission, we immediately begin metronidazole gel twice weekly for four to six months as suppressive therapy. ●We suggest treatment of asymptomatic women who are to undergo hysterectomy.Preoperative treatment decreases the frequency of postoperative infectious complications.metronidazoleclindamycin metronidazoletinidazole

71
Managment of pregnant women ●Pregnant women with BV are at increased risk of preterm birth. We recommend not screening all pregnant women for BV, given there is no evidence that screening and treatment of asymptomatic infection reduces the risk of preterm birth ●We treat pregnant women with symptomatic BV infection to relieve symptoms. We prescribe clindamycin300 mg orally twice daily for seven days or metronidazole 500 mg orally twice daily for seven days. ●We suggest treatment of asymptomatic women who are to undergo pregnancy termination.Preoperative treatment decreases the frequency of postoperative infectious complications.clindamycinmetronidazole

72
DIFFERENTIAL DIAGNOSIS — In the absence of microscopy, a lack of fishy odor (negative whiff test) makes the diagnosis of bacterial vaginosis (BV) unlikely. BV is usually suspected because of high vaginal pH (>4.5). Other causes of increased pH include trichomoniasis, atrophic vaginitis, and desquamative inflammatory vaginitis. These four entities are easily distinguishable by clinical and microscopic features. ●Women with BV do not have dyspareunia or signs of vaginal inflammation; in contrast, women with atrophic vaginitis, desquamative inflammatory vaginitis, and trichomoniasis usually have these signs and symptoms. ●Both atrophic vaginitis and desquamative inflammatory vaginitis are associated with an increased number of parabasal cells on microscopy, which is not observed in women with BV. ●A large number of polymorphonuclear leukocytes on microscopy are characteristic of desquamative inflammatory vaginitis, trichomoniasis, and atrophic vaginitis with infection, but not BV. ●Visualization of trichomonads readily makes the diagnosis of trichomoniasis in the setting of an elevated pH, however, in other cases, we suggest using more sensitive and specific diagnostic tests to diagnose or exclude trichomoniasis.
. Other causes of increased pH include trichomoniasis, atrophic vaginitis, and desquamative inflammatory vaginitis. These four entities are easily distinguishable by clinical and microscopic features. ●Women with BV do not have dyspareunia or signs of vaginal inflammation; in contrast, women with atrophic vaginitis, desquamative inflammatory vaginitis, and trichomoniasis usually have these signs and symptoms. ●Both atrophic vaginitis and desquamative inflammatory vaginitis are associated with an increased number of parabasal cells on microscopy, which is not observed in women with BV. ●A large number of polymorphonuclear leukocytes on microscopy are characteristic of desquamative inflammatory vaginitis, trichomoniasis, and atrophic vaginitis with infection, but not BV. ●Visualization of trichomonads readily makes the diagnosis of trichomoniasis in the setting of an elevated pH, however, in other cases, we suggest using more sensitive and specific diagnostic tests to diagnose or exclude trichomoniasis..")
73
THE END

Similar presentations