Download presentation
Presentation is loading. Please wait.

1
ASTHMA

2
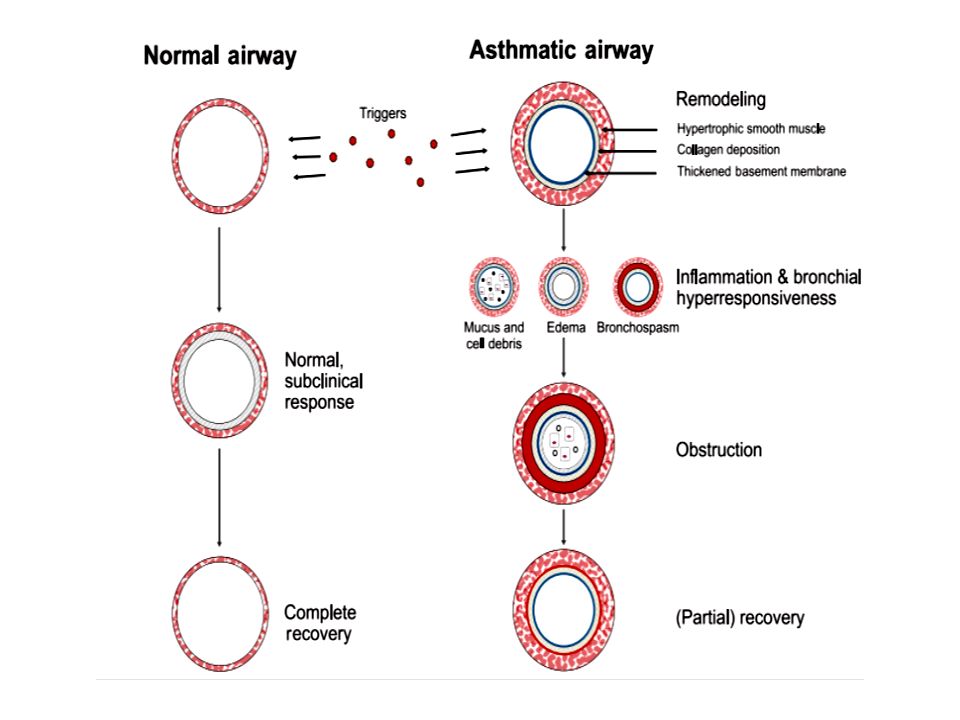
Asthma definition: “Asthma is a chronic inflammatory disorder associated with variable airflow obstruction and bronchial hyper responsiveness. It presents with recurrent episodes of wheeze, cough, shortness of breath, and chest tightness.”

3
Clinical features that increase the probability of asthma More than one of the following symptoms: Wheeze, cough, Difficulty in Breathing, chest tightness, particularly if symptoms: – are frequent and recurrent – are worse at night and in the early morning – occur in response to, or are worse after, exercise or other triggers, such as exposure to pets, cold, damp air, or with emotions/laughter Personal history of atopic disorder Family history of atopic disorder and/or asthma Widespread wheeze heard on auscultation History of improvement in symptoms or lung function in response to adequate therapy

4
Clinical features that lower the probability of asthma Symptoms with colds only, with no interval symptoms Isolated cough in the absence of wheeze or difficulty breathing History of moist cough Prominent dizziness, light-headedness, peripheral tingling Repeatedly normal physical examination of chest when symptomatic Normal peak expiratory flow (PEF) or spirometry when symptomatic No response to a trial of asthma therapy Clinical features pointing to alternative diagnosis
 or spirometry when symptomatic No response to a trial of asthma therapy Clinical features pointing to alternative diagnosis")
5
Causes of Asthma The development of asthma appears to involve the interplay between host factors (particularly genetics) and environmental exposures that occur at a crucial time in the development of the immune system. Imbalance between Th1-type and Th2- type cytokine responses in early life. The immune response will down regulate the Th1 immune response that fights infection and instead will be dominated by Th2 cells, leading to the expression of allergic diseases and asthma. This is known as the “hygiene hypothesis,” which postulates that certain infections early in life, exposure to other children, less frequent use of antibiotics, and “country living” is associated with a Th1 response and lower incidence of asthma, whereas the absence of these factors is associated with a persistent Th2 response and higher rates of asthma.

6
Genetics: Asthma has an inheritable component, but the genetics involved remain complex. Environmental factors: Two major factors are the most important in the development, persistence, and possibly the severity of asthma: airborne allergens (particularly sensitization and exposure to house-dust mite ) viral respiratory infections (including RSV and rhinovirus). Other environmental factors are under study: tobacco smoke air pollution (ozone and particular matter) and diet (obesity or low intake of antioxidants and omega-3 fatty acids).
 viral respiratory infections (including RSV and rhinovirus). Other environmental factors are under study: tobacco smoke air pollution (ozone and particular matter) and diet (obesity or low intake of antioxidants and omega-3 fatty acids)..")
7
Mechanisms: Asthma Inflammation

8
Asthma Inflammation: Cells and Mediators

11
Early Childhood Risk Factors Parental Asthma Allergy – Atopic dermatitis – Allergic rhinitis – Food allergy – Inhalant allergen sensitization – Food allergen sensitization

12
Precipitating and/or aggravating factors Viral respiratory infections Environmental allergens, indoor (e.g., mold, house-dust mite, cockroach, animal dander or secretory products) and outdoor (e.g., pollen) Characteristics of home including age, location, cooling and heating system, wood-burning stove, humidifier, carpeting over concrete, presence of molds or mildew, presense of pets with fur or hair, characteristics of rooms where patient spends time (e.g., bedroom and living room with attention to bedding, floor covering, stuffed furniture) Smoking (patient and others in home or daycare) Exercise Occupational chemicals or allergens
 and outdoor (e.g., pollen) Characteristics of home including age, location, cooling and heating system, wood-burning stove, humidifier, carpeting over concrete, presence of molds or mildew, presense of pets with fur or hair, characteristics of rooms where patient spends time (e.g., bedroom and living room with attention to bedding, floor covering, stuffed furniture) Smoking (patient and others in home or daycare) Exercise Occupational chemicals or allergens")
13
Environmental change (e.g., moving to new home; going on vacation; and/or alterations in workplace, work processes, or materials used) Irritants (e.g., tobacco smoke, strong odors, air pollutants, occupational chemicals, dusts and particulates, vapors, gases, and aerosols) Emotions (e.g., fear, anger, frustration, hard crying or laughing) Stress (e.g., fear, anger, frustration) Drugs (e.g., aspirin; and other nonsteroidal anti-inflammatory drugs, beta- blockers including eye drops, others) Food, food additives, and preservatives (e.g., sulfites) Changes in weather, exposure to cold air Endocrine factors (e.g., menses, pregnancy, thyroid disease) Comorbid conditions (e.g. sinusitis, rhinitis,GERD )
.")
14
Classifying Severity and Initiating Treatment

15
CLINICAL FEATURES Symptoms: Intermittent dry cough Expiratory wheezing Shortness of breath Chest tightness Chest pain Fatigue Difficulty keeping up with peers in physical activities Signs: Expiratory wheezing Prolonged expiratory phase Decreased breath sounds Crackles/ rales Accessory muscle use Nasal flaring Absence of wheezing in severe cases Pulses paradoxus

16
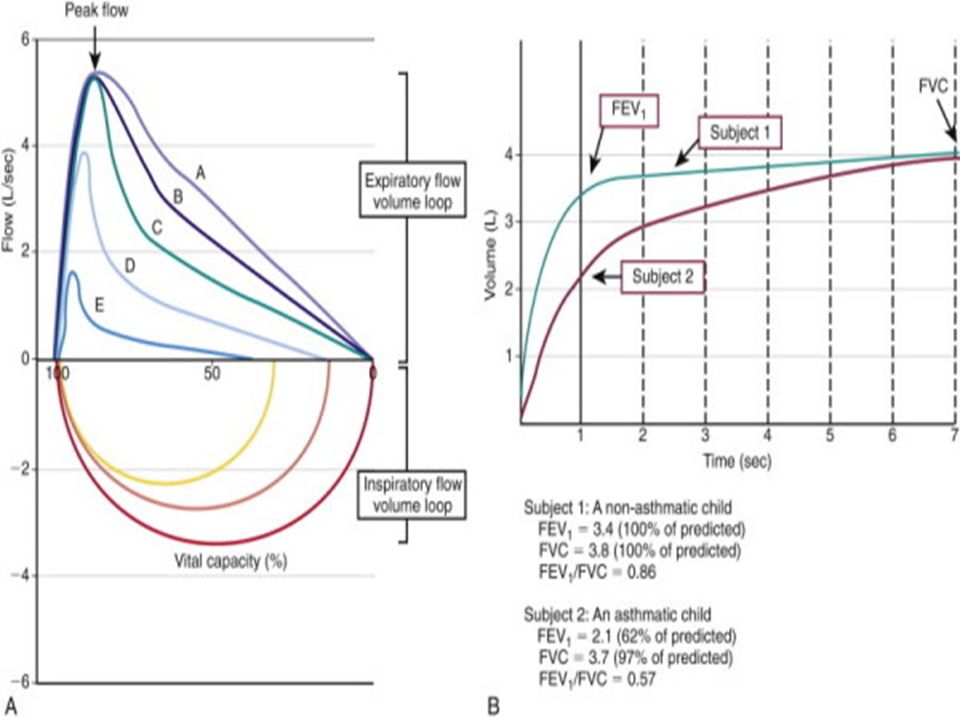
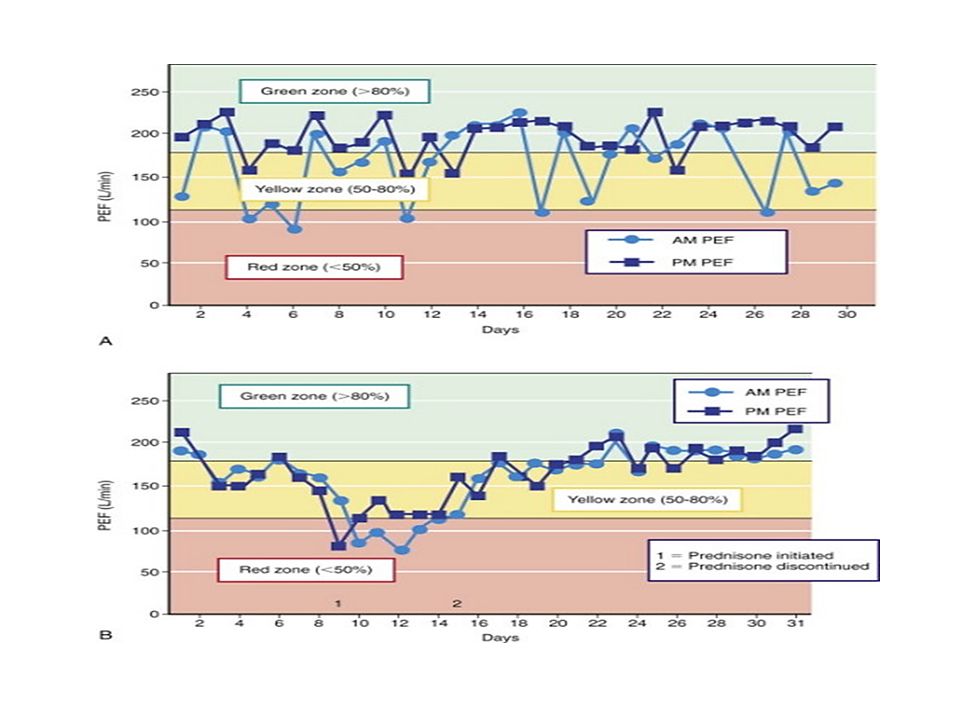
Spirometry: Feasible in children >6 years of age Monitoring Asthma and efficacy of treatment Measures FVC, FEV 1 and FEV1/FVC Ratio Normal values for children available on the basis of height, gender and ethnicity. Airflow Limitation: Low FEV1 FEV1/ FVC ratio < 0.80 Bronchodilator response to β-agonist: Improvement in FEV1 ≥ 12% Exercise challenge: Worsening of FEV1 ≥ 15% Peak expiratory flow rate: It is highly suggestive of asthma when: >15% increase in PEFR after inhaled short acting β2 agonist >15% decrease in PEFR after exercise Diurnal variation > 10% in children not on bronchodilator X-ray : Often normal, sometimes Hyperinflation

19
DIFFERENTIAL DIAGNOSTIC POSSIBILITIES FOR ASTHMA

20
Asthma Management and Prevention Program: Five Components 1. Develop Patient/Doctor Partnership 2. Identify and Reduce Exposure to Risk Factors 3. Assess, Treat and Monitor Asthma 4. Manage Asthma Exacerbations 5. Special Considerations

21
1. Develop Patient/Doctor Partnership Guidelines on asthma management should be available for local use by local asthma planning teams Clear communication between health care professionals and patient is key Educate continually Include the family Provide information about asthma Provide training on self-management skills Emphasize a partnership among health care providers, the patient, and the patient’s family

22
2. Identify and Reduce Exposure to Risk Factors Asthma exacerbations may be caused by a variety of risk factors – allergens, viral infections, pollutants and drugs. Reducing exposure to some categories of risk factors improves the control of asthma and reduces medications needs. Reduce exposure to indoor allergens Avoid tobacco smoke Avoid vehicle emission Identify irritants in the workplace Explore role of infections on asthma development Influenza vaccination should be provided to patients with asthma when vaccination of the general population is advised

23
3. Assess, Treat and Monitor Asthma The goal of asthma treatment, to achieve and maintain clinical control, can be achieved in a majority of patients with a pharmacologic intervention strategy developed in partnership between the patient/family and the health care professional. The focus on asthma control is important because: Attainment of control correlates with a better quality of life, and reduction in health care use Determine the initial level of control to implement treatment (assess patient impairment) Maintain control once treatment has been implemented (assess patient risk)
 Maintain control once treatment has been implemented (assess patient risk).")
24
Levels of Asthma Control (Assess patient impairment) Levels of Asthma Control (Assess patient impairment)
 Levels of Asthma Control (Assess patient impairment)")
25
Assess Patient Risk Features that are associated with increased risk of adverse events in the future include: Poor clinical control Frequent exacerbations in past year Ever admission to critical care for asthma Low FEV 1, exposure to cigarette smoke, high dose medications

26
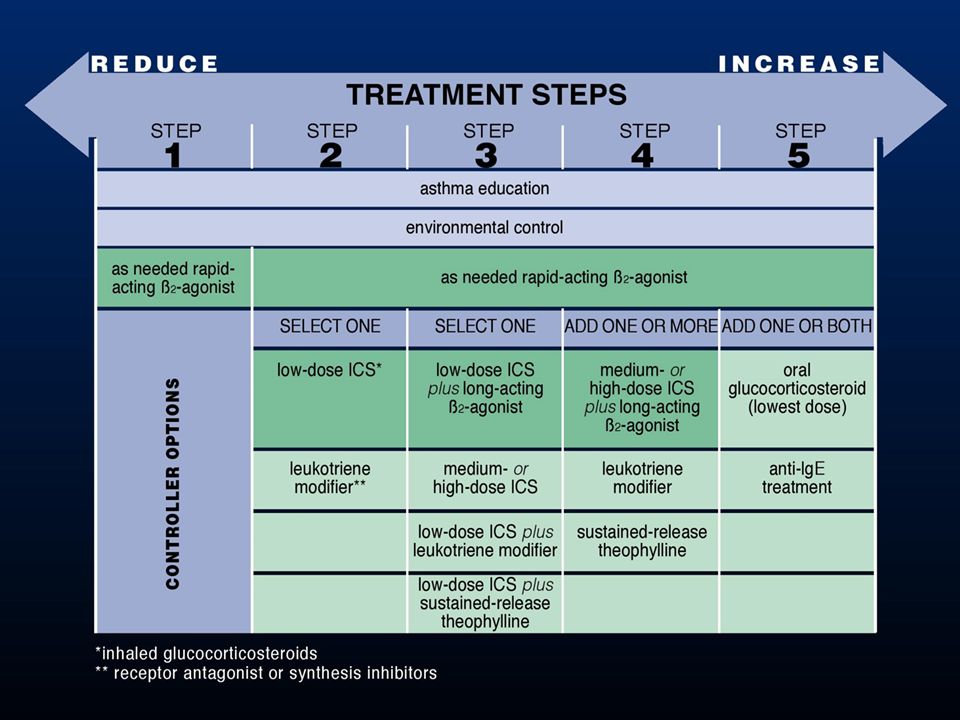
Depending on level of asthma control, the patient is assigned to one of five treatment steps Treatment is adjusted in a continuous cycle driven by changes in asthma control status. The cycle involves: - Assessing Asthma Control - Treating to Achieve Control - Monitoring to Maintain Control A stepwise approach to pharmacological therapy is recommended The aim is to accomplish the goals of therapy with the least possible medication Although in many countries traditional methods of healing are used, their efficacy has not yet been established and their use can therefore not be recommended

27
The choice of treatment should be guided by: Level of asthma control Current treatment Pharmacological properties and availability of the various forms of asthma treatment Economic considerations Cultural preferences and differing health care systems

28
Medications in Asthma Controller Medications Inhaled glucocorticosteroids Leukotriene modifiers Long-acting inhaled β 2 -agonists in combination with inhaled glucocorticosteroids Systemic glucocorticosteroids Theophylline Cromones Anti-IgE Reliever Medications Rapid-acting inhaled β 2 -agonists Systemic glucocorticosteroids Anticholinergics Theophylline Short-acting oral β 2 -agonists

29
Estimate Comparative Daily Dosages for Inhaled Glucocorticosteroids by Age Drug Low Daily Dose( g) > 5 y Age 5 y Age < 5 y Medium Daily Dose ( g) > 5 y Age 5 y Age < 5 y High Daily Dose ( g) > 5 y Age 5 y Age < 5 y Beclomethasone200-500 100-200 >500-1000 >200-400 >1000 >400 Budesonide200-600 100-200 600-1000 >200-400>1000 >400 Budesonide-Neb Inhalation Suspension 250-500 500-1000 >1000 Ciclesonide 80 – 160 80-160 >160-320 >160-320>320-1280 >320 Flunisolide500-1000 500-750>1000-2000 >750-1250 >2000 >1250 Fluticasone100-250 100-200 >250-500 >200-500 >500 >500 Mometasone furoate200-400 100-200 > 400-800 >200-400>800-1200 >400 Triamcinolone acetonide400-1000 400-800>1000-2000 >800-1200>2000 >1200
 > 5 y Age 5 y Age < 5 y Medium Daily Dose ( g) > 5 y Age 5 y Age < 5 y High Daily Dose ( g) > 5 y Age 5 y Age < 5 y Beclomethasone > > >1000 >400 Budesonide > >1000 >400 Budesonide-Neb Inhalation Suspension >1000 Ciclesonide 80 – > > > >320 Flunisolide > > >2000 >1250 Fluticasone > > >500 >500 Mometasone furoate > > > >400 Triamcinolone acetonide > > >2000 >1200")
30
Allergen-specific Immunotherapy Greatest benefit of specific immunotherapy using allergen extracts has been obtained in the treatment of allergic rhinitis The role of specific immunotherapy in asthma is limited Specific immunotherapy should be considered only after strict environmental avoidance and pharmacologic intervention, including inhaled glucocorticosteroids, have failed to control asthma Perform only by trained physician

31
controlled partly controlled uncontrolled exacerbation LEVEL OF CONTROL maintain and find lowest controlling step consider stepping up to gain control step up until controlled treat as exacerbation TREATMENT OF ACTION TREATMENT STEPS REDUCE INCREASE STEP 1 STEP 1 STEP 2 STEP 2 STEP 3 STEP 3 STEP 4 STEP 4 STEP 5 STEP 5 REDUCE INCREASE

33
Treating to Maintain Asthma Control When control as been achieved, ongoing monitoring is essential to: - maintain control - establish lowest step/dose treatment Asthma control should be monitored by the health care professional and by the patient

34
Stepping down treatment when asthma is controlled When controlled on medium- to high-dose inhaled glucocorticosteroids: 50% dose reduction at 3 month intervals. When controlled on low-dose inhaled glucocorticosteroids: switch to once- daily dosing When controlled on combination inhaled glucocorticosteroids and long- acting inhaled β 2 -agonist: reduce dose of inhaled glucocorticosteroid by 50% while continuing the long-acting β 2 -agonist If control is maintained: reduce to low-dose inhaled glucocorticosteroids and stop long-acting β 2 -agonist

35
Stepping up treatment in response to loss of control Rapid-onset, short-acting or long-acting inhaled β2-agonist bronchodilators provide temporary relief. Need for repeated dosing over more than one/two days signals need for possible increase in controller therapy Use of a combination rapid and long-acting inhaled β 2 -agonist (e.g., formoterol) and an inhaled glucocorticosteroid (e.g., budesonide) in a single inhaler both as a controller and reliever is effecting in maintaining a high level of asthma control and reduces exacerbations Doubling the dose of inhaled glucocortico-steroids is not effective, and is not recommended
 and an inhaled glucocorticosteroid (e.g., budesonide) in a single inhaler both as a controller and reliever is effecting in maintaining a high level of asthma control and reduces exacerbations Doubling the dose of inhaled glucocortico-steroids is not effective, and is not recommended.")
37
Component 4: Manage Asthma Exacerbations Exacerbations of asthma are episodes of progressive increase in shortness of breath, cough, wheezing, or chest tightness Exacerbations are characterized by decreases in expiratory airflow that can be quantified and monitored by measurement of lung function (FEV 1 or PEF) Severe exacerbations are potentially life-threatening and treatment requires close supervision Primary therapies for exacerbations: Repetitive administration of rapid-acting inhaled β 2 -agonist Early introduction of systemic glucocorticosteroids Oxygen supplementation Closely monitor response to treatment with serial measures of lung function
 Severe exacerbations are potentially life-threatening and treatment requires close supervision Primary therapies for exacerbations: Repetitive administration of rapid-acting inhaled β 2 -agonist Early introduction of systemic glucocorticosteroids Oxygen supplementation Closely monitor response to treatment with serial measures of lung function")
38
5.Special considerations Special considerations are required to manage asthma in relation to: Pregnancy Surgery Rhinitis, sinusitis, and nasal polyps Occupational asthma Respiratory infections Gastroesophageal reflux Aspirin-induced asthma Anaphylaxis and Asthma

39
STATUS ASTHAMATICUS Status asthmaticus is the condition of a patient in progressive respiratory failure due to asthma, in whom conventional forms of therapy have failed

40
Status Asthamaticus Assessment Findings consistent with impending respiratory failure: Altered level of consciousness Inability to speak Absent breath sounds Central cyanosis Diaphoresis Inability to lie down Marked pulsus paradoxus

41
Clinical Asthma Score

43
Thank You

Similar presentations



>")
 Airway.>")



 -based on the recognition of a characteristic pattern of symptoms and signs and the absence of an alternative.>")



 TEACHING SLIDE SET January 2013>")







 Diagnosis and management of chronic asthma in line with current BTS guidelines (Dr Lowery) 3 x Case.>")
