Download presentation
Presentation is loading. Please wait.

1
Principles and Practice of Geriatric rehabilitation

2
Objectives Upon completion of this lecture student will be able to:
Explain the purpose of geriatric rehabilitation. Describe major principles influencing geriatric rehabilitation. Understand the goals for adapting an environment for the older person.

3
Introduction The purpose of geriatric rehabilitation is to assist the disabled aged in recovering lost physical, psychological or social skills to make them more independent. The decline in muscle strength and mass, respiratory reserve and cardiovascular functioning ,kyphotic postural changes and many other physiological and psychological changes associated with inactivity and ageing.

4
Principles of geriatric rehabilitation.
Three major principles : Variability. Hypokinetics. Optimal health.

5
VARIABILITY Variability of the aged must be considered in rehabilitation principles and practices of aged. Variability of capabilities within an aged group is more pronounced than younger. Optimum health is directly related to optimum functional ability. In acute situations, rehabilitation must be directed toward: Stabilizing the primary problems. Preventing secondary complications such as bed sores & contractures Restoring lost functions

6
HYPOKINETICS Hypokinetics describes the physiology of inactivity
Most common reason for losses in functional capabilities in aged is inactivity or immobility. There are many reasons for immobilizing the aged. Deconditioning is defined as multiple changes in multiple organ system physiology that are induced by inactivity and reversed by activity(exercise) The degree of deconditioning depends on degree of superimposed inactivity and prior level of physical fitness
 The degree of deconditioning depends on degree of superimposed inactivity and prior level of physical fitness.")
7
HYPOKINETICS Two major categories of inactivity or hypokinetics :
The acute hypokinetics of bed rest Chronic inactivity induced by a sedentary lifestyle or chronic disease.

8
Systemic complications of bed rest
Neurosensory: Decreased EEG Decreased thermoregulation Decreased cognition Decreased in reaction time Decreased balance Decreased postural sway

9
Systemic complications of bed rest
Cardiovascular: Decreased output. Increased heart rate. Decreased oxygen uptake. Decreased blood volume. Decreased aerobic capacity. Delayed post activity recovery time

10
Systemic complications of bed rest
Respiratory: Atelectais. Hypoxemia. Increased risk of pneumonia. Decreased chest wall compliance. Decreased intercoastal muscle strength. Decreased vital capacity. Impaired gas exchange

11
Systemic complications of bed rest
Musculoskeletal Decreased muscle strength. Decreased aerobic capacity. Bone loss Joint contractures Osteoarthritis Decreased glycoproteins

12
Systemic complications of bed rest
Genitourinary : Urinary tract infection. Urinary incontinence. Skin- pressure sores Gastrointestinal – constipation. Functional Decreased activities of daily living. Increased risk of falls

13
Systemic complications of bed rest
Psychological Anxiety Fear Depression Mood changes Hallucinations Sleep disturbances

14
Systemic complications of bed rest
B- bladder and bowel incontinence retention, bed sores E- emotional trauma D- deconditioning of muscles& nerves, depression, demineralization of bone R- ROM loss & contractures, restlessness, renal dysfunction E- energy depletion, EEG activity decrease S- sensory deprivation,sleep disorders, skin problems T- trouble

15
OPTIMAL HEALTH The last principle in geriatric rehabilitation is of optimal health. WHO defines health as a state of complete physical, mental and social well being. The existence of complete physical health refers to absence of pathology, impairment or disability. WHO , mental health include cognitive and intellectual intactness as well as emotional well being.

16
OPTIMAL HEALTH There are some cumulative effects : Biological
Physiological Anatomical Preventing impairment and disability is a key principle in geriatric rehabilitation.

17
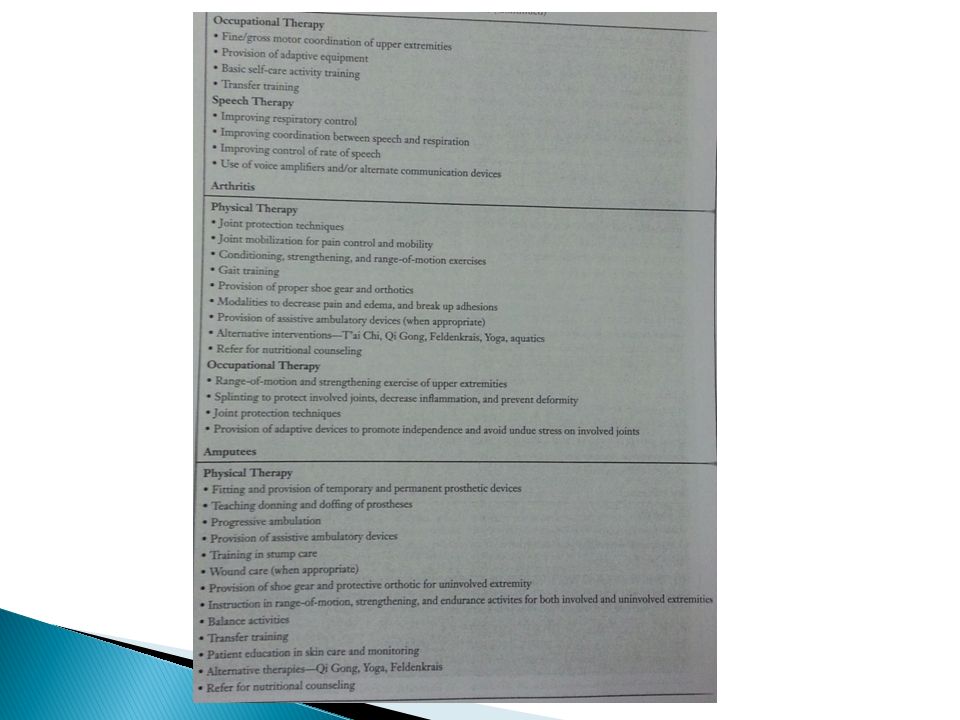
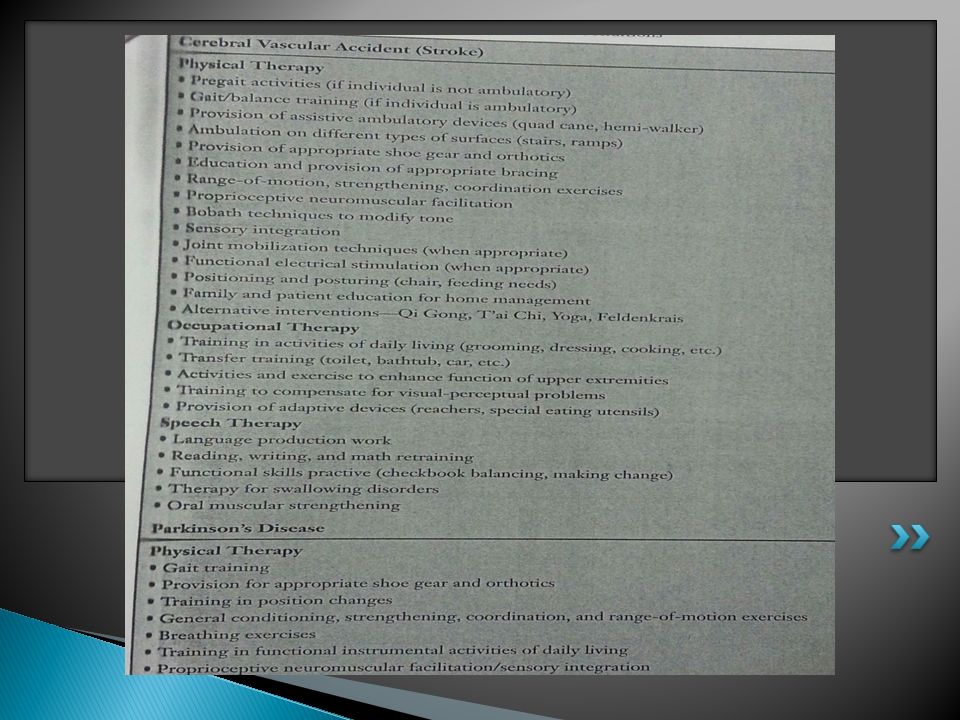
REHABILITATIVE MEASURES
Rehabilitation should be directed at preventing premature disability. Rehabilitation efforts should focus medically on : Reducing the inflammation through drugs or ice. Maintaining joint mobility during the acute phase(by modalities, assist in reducing oedema or physical therapy) Joint protection techniques and prescription of adaptive devices such as walker to protect the joint.
 Joint protection techniques and prescription of adaptive devices such as walker to protect the joint.")
18
Rehabilitation efforts should focus medically on
Provision for proper nutrition in light of medication and also vitamin C is crucial component in health. Social and psychological support to provide emotional and motivational support.

19
REHABILITATIVE MEASURES
Health Awareness and Beliefs Exercise programming : Exercises have potential for improving physical fitness, agility and speed of response. They also serve to improve muscle strength, flexibility, bone health and cardiovascular response. Exercise has been shown to provide social and psychological benefits affecting the quality of life and social well being.

20
REHABILITATIVE MEASURES
Pain management : Pain management is very important factor in geriatric rehabilitation. Pain is human perception or recognition of a noxious stimulus. In geriatric 2 types of pain : acute & chronic. Treatment of acute pain may include medications to reduce inflammation, ice, heat and gentle mobility exercises. Chronic pain is more frequently observed and difficult to control

21
ASSISTIVE DEVICES Assistive devices such as cane, a quad or walker can be prescribed to improve stability during ambulation and reduce stresses on the joint. Wheel chair prescription may be necessary for longer distances. Proper positioning and seating for individual who must sit for extended periods is required to decrease discomfort and keep pressures off of bony prominences, provide adequate postural support, facilitate feeding and prevent progression of joint contractures and deformities.

22
RESTRAINTS The use of physical restraints in an attempt to keep patients safe, continiues to be practised despite evidence that they often increase the incidence of falls. Decreasing the use of physical restraints continues to be a challenge for the health care team. Restraints are used to prevent injury to self, control of agitated or restless behavior, management of a resident’s cognitive deficit and poor judgement.

23
BENEFITS OF RESTRAINTS
Prevention/protection from falls and other injuries. Allows medical treatment to proceed without patient interference. Maintenance of body alignment. Increases patient’s feeling of security and safety.

24
RISKS OF RESTRAINTS Injury from falls.
Accidental death by strangulation Skin abrasions and breakdown. Immobilization sequelae (deconditioning, muscle atrophy, contractures, deep vein thrombosis) Decline in ADLs, functional mobility. Cardiac stress. Increased mortality.
 Decline in ADLs, functional mobility. Cardiac stress. Increased mortality.")
25
FALLS IN THE ELDERLY Falls are not part of normal ageing process, but are due to interaction of underlying physical dysfunction, medications and environmental hazards. Poor health status, impaired mobility from inactivity or chronic illness, postural instability. Medical conditions are often a cause of falling.

26
FALLS IN THE ELDERLY The fear of falling is often a cause for inactivity and is commonly seen an individual who has sustained a previous fall. Limitations of range of motion, decreased muscle strength and joint mobility, coordination problems can predispose an elderly individual to falling. Specific strengthening and gait training programs assist in preventing falls by improving overall strength and coordination and balance time.

27
FALLS IN THE ELDERLY Gait evaluation is one of the most important components in fall prevention. The ‘Get-up and Go” test is a method used often to test functional strength, balance, coordination and safety during gait. Balance exercises can be incorporated into functional activities for the aged. Moving from sit to stand and from stand to sit are examples of controlled voluntary weight shifting

28
Shifting the trunk forward and back and from side to side while sitting are examples of voluntary weight shifting.

29
WHAT TO DO IF YOU FALL AT HOME
Remain calm and assess your situation. Roll over slowly.Locate the nearest sturdy chair. Crawl or shuffle to the chair. Kneel, then stand up using the chair. Then turn and sit down. Call or wait for help.

30
ADAPTING THE ENVIRONMENT
The process of adapting to the environment or adapting environment to aged person is very important. Evaluation of the environment is more difficult than task analysis because the environment of concern is the one in which individual actually lives and has to function.

Similar presentations