Download presentation
Presentation is loading. Please wait.

1
Delirium Detection Eric Mauri Michael Marquis Matthew Kasztejna Advised by: Dr. Wes Ely

2
Delirium Overview Brain’s form of organ dysfunction Defined as a disturbance of consciousness characterized by an acute onset and fluctuating course of impaired cognitive functioning. Direct consequence of medical conditions, medication, toxin exposure or a combination of all of these. Major contributing factor: Lack of REM sleep Ely et al. Seminars in Respiratory and Critical Care Medicine, Vol. 22, Num. 2, 2001.

3
Delirium Demographics Occurs in 15-60% of general patients Develops in over 80% of ICU patients Complicates hospitalization of 2-3 million people yearly (affecting mostly the elderly) Involves over 17.5 million inpatient days. Over $4 billion in Medicare expenditures. Development of delirium selected as one of the top three most important areas for quality of care improvement in older adults. Ely et al. Seminars in Respiratory and Critical Care Medicine, Vol. 22, Num. 2, 2001.

4
How is it detected? Arousal and Attention Assessment –Confusion Assessment Method (CAM-ICU) 1.Acute onset of mental changes 2.Inattention 3.Disorganized thinking 4.Alertness Patients are determined to be CAM- positive if they have both features 1 & 2 and either feature 3 or 4.
 1.Acute onset of mental changes 2.Inattention 3.Disorganized thinking 4.Alertness Patients are determined to be CAM- positive if they have both features 1 & 2 and either feature 3 or 4..")
5
CAM-ICU Cont. Example Questions –As part of the inattention assessment patients are shown a set of 5 pictures, then a set of 10 pictures (5 of which were in the original set). They are asked whether the picture was in the first set, if they get more than 3 wrong then they are inattentive. –As part of the disorganized thinking assessment they are asked questions like: Will a stone float on water? Are there fish in the sea? Can you use a hammer to pound a nail? Problems –Subjective –No Standardization –Time Intensive http://www.aacn.org/pdfLibra.NSF/Files/TrumanB/$file/TrumanB.pdf
. They are asked whether the picture was in the first set, if they get more than 3 wrong then they are inattentive. –As part of the disorganized thinking assessment they are asked questions like: Will a stone float on water. Are there fish in the sea. Can you use a hammer to pound a nail. Problems –Subjective –No Standardization –Time Intensive")
6
Project Objective Develop system that can continuously measure delirium in ICU patients Solution –Quantitative EEG –Acquire digital signal –Transform it into the frequency domain –Focus on certain frequency bands that have been clinically shown to be important to sleep. –Benefits –Inexpensive –Noninvasive –Software reduces man hours –Most importantly several studies have shown that EEG can be effectively used to monitor sleep

7
Stages of Sleep Stage 1 – Frequency 4 to 8 Hz, 5% of total sleep –consists mostly of theta waves (high amplitude, low frequency (slow)) –brief periods of alpha waves, similar to those present while awake Stage 2 – Frequency 8 to 15 Hz, 50 % of total sleep –peaks of brain waves become higher and higher (sleep spindles) –k-complexes (peaks suddenly drastically descend and then pick back up) follow spindles Stage 3 & 4 - Frequency.5 to 4 Hz, 7 & 11% respectively –very slow brain waves, called delta waves (lower frequency than theta waves) REM - Frequency > 12 Hz, ~ 25% increases as night goes on –beta waves have a high frequency and occur when the brain is quite active, both in REM sleep and while awake www.dreamviews.com/sleepstages.html www.silentpartners.org
) –brief periods of alpha waves, similar to those present while awake Stage 2 – Frequency 8 to 15 Hz, 50 % of total sleep –peaks of brain waves become higher and higher (sleep spindles) –k-complexes (peaks suddenly drastically descend and then pick back up) follow spindles Stage 3 & 4 - Frequency.5 to 4 Hz, 7 & 11% respectively –very slow brain waves, called delta waves (lower frequency than theta waves) REM - Frequency > 12 Hz, ~ 25% increases as night goes on –beta waves have a high frequency and occur when the brain is quite active, both in REM sleep and while awake")
8
Possible Systems Gold Standard EEG – Sleep Labs Bispectral Index (BIS) – Aspect Medical Sleep I/T Vitaport – Temec SNAP – Nicolet Biomedical
 – Aspect Medical Sleep I/T Vitaport – Temec SNAP – Nicolet Biomedical")
9
Ideal System Measures amount of REM sleep and capable of making real-time measurements Small (155 x 90 x 57 mm), cost-effective, comfortable and practical Real-Time measurements, data storage and analysis of information (software) Maximum of 3 to 5 leads Capability to store up to 48 hrs worth of data on a removable data card for easy data transfer
, cost-effective, comfortable and practical Real-Time measurements, data storage and analysis of information (software) Maximum of 3 to 5 leads Capability to store up to 48 hrs worth of data on a removable data card for easy data transfer")
10
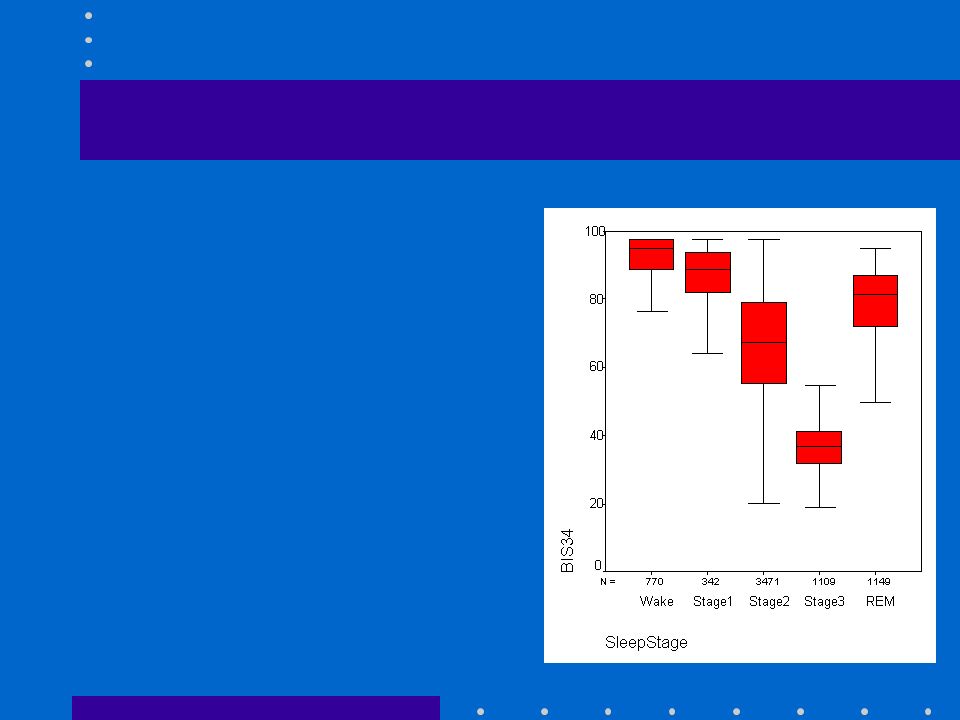
Ruled out systems Gold standard EEG –Most complex, 26 lead system is too complicated for use in the ICU. BIS –Simplest, 3-lead system which produces a single number to describe changes in EEG that relate to levels of sedation and consciousness. –BIS is only effective for the first 3 stages of sleep, the BIS number decreases as sleep progress from the first to third stage, yet the number increases during REM sleep due to increased glucose metabolism in the brain. Sleep I/T –Outdated, better technology exists

11
Vitaport Full clinical polysomnographs (EEG, EOG, EMG, EKG, respiratory effort, oxygen saturation) 16 channel EEG; 600 grams; Flexible Electrically efficient: 48 hrs of continuous monitoring with a set of AA batteries Can be configured to 3-5 leads Various software options independently selectable for each of the 16 channels Cost: $6,500 for Vitaport 3 recorder base with setup software –Leasing available; depending upon length of lease, it would be 10%-15% of the sales price (per month)
 16 channel EEG; 600 grams; Flexible Electrically efficient: 48 hrs of continuous monitoring with a set of AA batteries Can be configured to 3-5 leads Various software options independently selectable for each of the 16 channels Cost: $6,500 for Vitaport 3 recorder base with setup software –Leasing available; depending upon length of lease, it would be 10%-15% of the sales price (per month)")
12
SNAP Portable, battery-operated, handheld-based single channel EEG monitoring tool 3 lead system Enables accurate measuring of EEG with convenience and versatility of a handheld computer (PDA) Outputs a numerical value (SNAP index) –0, fully suppressed, no active EEG signal –100, fully active EEG brain state Cost: $4,500 plus $200 for the PDA
 Outputs a numerical value (SNAP index) –0, fully suppressed, no active EEG signal –100, fully active EEG brain state Cost: $4,500 plus $200 for the PDA")
13
Recommendations SNAP and Vitaport are best equipped for ICU setting Both are compact, lightweight and extremely flexible Compatible with review and analysis software applications, which will help reduce staff hours Cost-effective

14
A Learning Process Unforeseen Obstacles –Licensing and leasing issues –Contradicting schedules and unexpected cancellations –Lengthy delivery times –Project involved research and collaborating with a network of different professionals, each with conflicting agendas and personal interests

Similar presentations



 This is used to measure electrical activity in the brain This is used to measure electrical.>")




 Purpose: Provide initial and ongoing screening of patients for identification of signs and symptoms of delirium. Initiate.>")







>")


