Download presentation
Presentation is loading. Please wait.

1
Management of Raised ICP Jon-Paul Chamoun

2
Case study Little Jimmy 24 year old male presents to ED post footy tackle with severe headstrike associated wth loss of consciousness 1 minute. -GCS 14 at the scene -Sore head -On examination HR 85 reg. BP 130/80 RR 22 36.8 CVS, Abdo, Resp NAD Neuro: PEARL UL + LL Normal Tone Power Reflexes Sensation and Coordination

3
Tea Break! Beep Beep ‘Hi Dr, please review little Jimmy. Drowsy ++’ Crap, I missed the SSSM Neurosurg topics!

4
Little Jimmy.. Now HR 40 BP 180/90 RR 8 36.8 Drowsy+++ Eyes crossed Pupils dilated…

5
PANIC = Neurons not firing

6
RIP Little Jimmy A bad referral leads to…

10
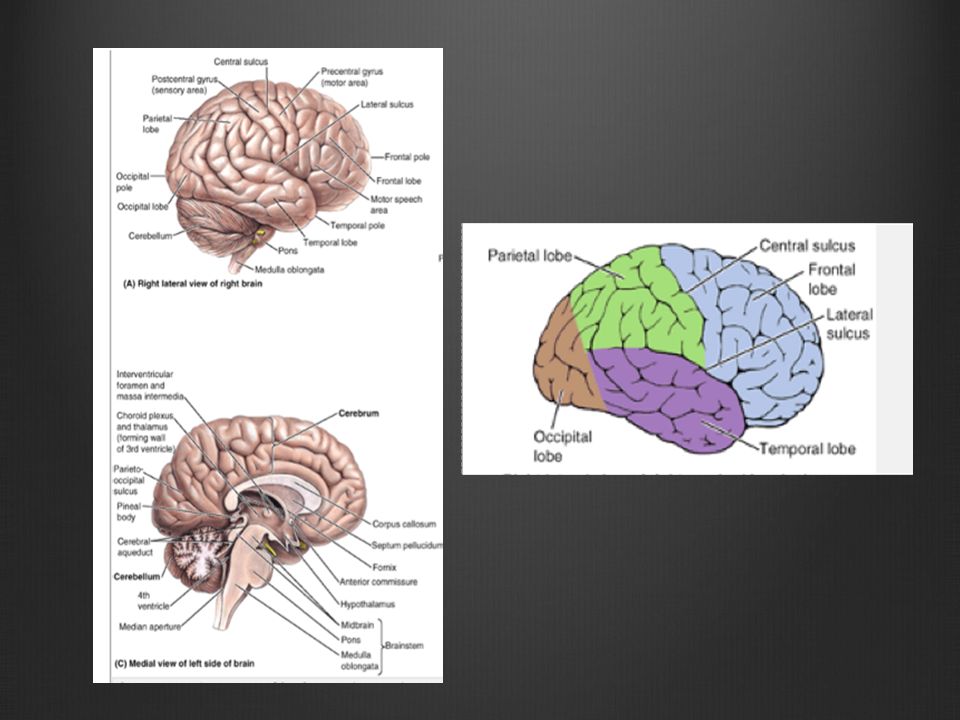
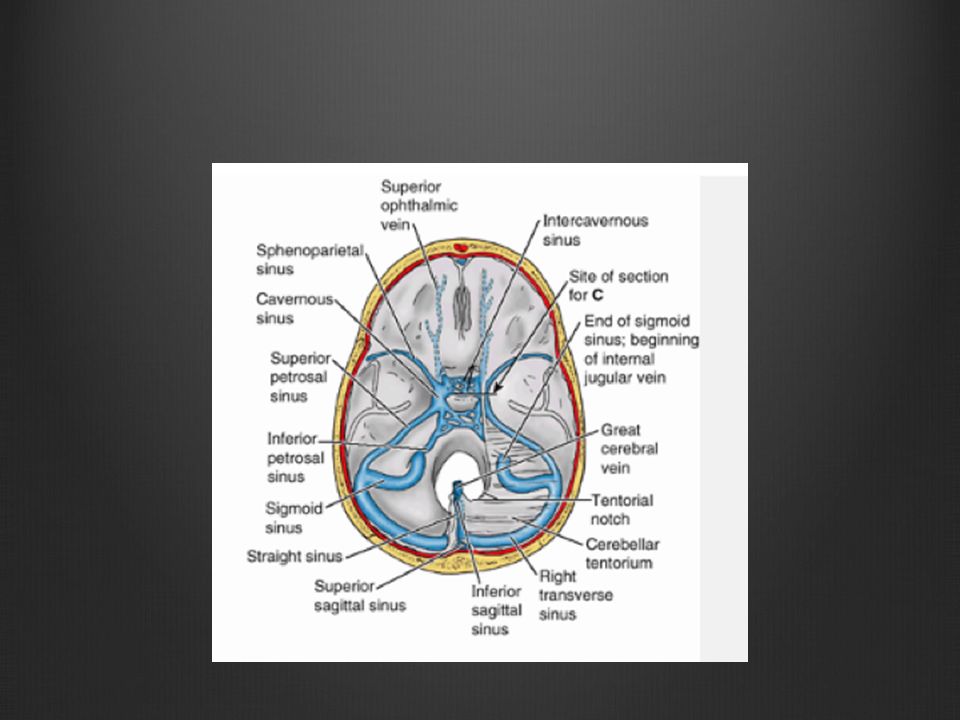
The drainage

11
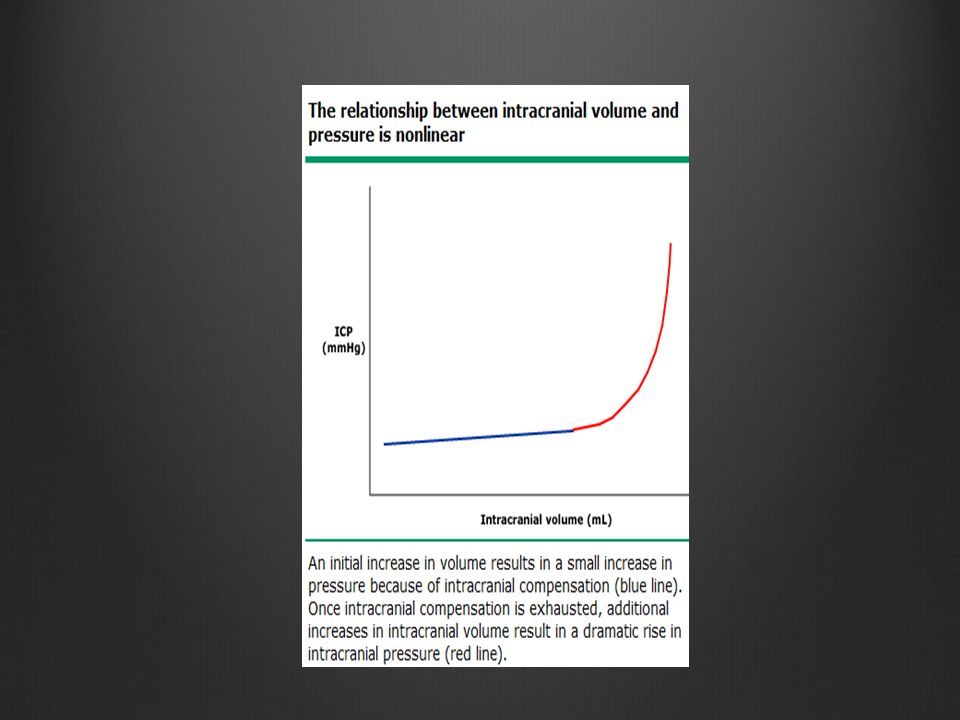
Physiology Inside the rigid Vault (~ 1500mls) -Brain (80%) -Blood (10%) -CSF (10%)
 -Brain (80%) -Blood (10%) -CSF (10%)")
12
Intracranial Pressure Normal : <15mmHg (adults) Lower in children than adults Transiently increases with sneezing, coughing and valsalva manouvres
 Lower in children than adults Transiently increases with sneezing, coughing and valsalva manouvres")
14
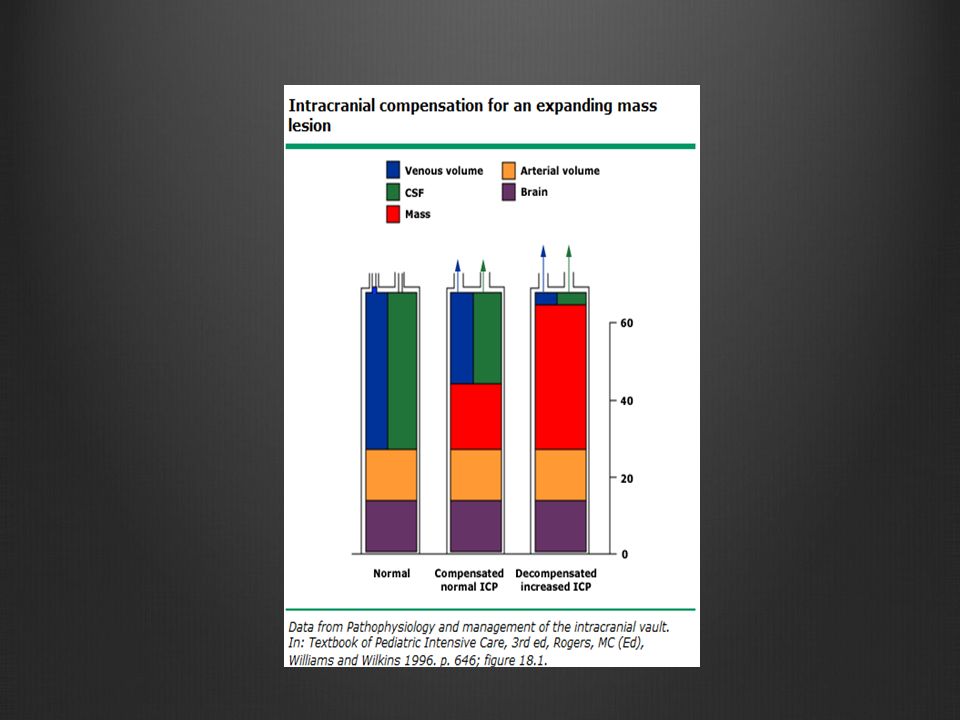
The overall volume of the cranial vault cannot change therefore an increase in the proportion of one component, or the presence of a pathologic component will result in displacement of structures, an increase in ICP or both. ….Who’s Doctrine is this??

15
The Monroe-Kellie Doctrine

17
Causes Too much Brain -Tumour, Haematoma, Oedema Too much CSF -Choroid plexus papilloma, Arachnoid granulation adhesions, Obstructive hydrocephalus Too much Blood - Obstruction of venous outflow (venous sinus thrombosis, jugular vein compression, neck surgery)
")
18
Consequences of Raised ICP 1. Cerebral blood flow -CBF = (CAP – JVP) / CVR -CPP = MAP - ICP 2. Brainstem compression 3. Both

19
What was happening to Jimmy? HeadacheVomiting Depressed Consciousness Fixed and dilated pupils A triad of Bradycardia, Hypertension and respiratory depression….Also known as who’s triad?

20
Cushing’s Triad

21
Papilloedema

22
Little Timmy (Jimmy’s Brother) 20 year old male presents to ED post footy tackle with severe headstrike associated wth loss of consciousness 1 minute.
 20 year old male presents to ED post footy tackle with severe headstrike associated wth loss of consciousness 1 minute.")
23
The next intern attended SSSM talks… D anger D anger R esponse (GCS) R esponse (GCS) S end for help (!!!!!!!) S end for help (!!!!!!!) A irway A irway B reathing B reathing C irculation C irculation D ont(EverForgetGlucose) D ont(EverForgetGlucose) IWho am I SWhats happened BWhat’s happening AWhat I think RWhat I need
 R esponse (GCS) S end for help (!!!!!!!) S end for help (!!!!!!!) A irway A irway B reathing B reathing C irculation C irculation D ont(EverForgetGlucose) D ont(EverForgetGlucose) IWho am I SWhats happened BWhat’s happening AWhat I think RWhat I need")
24
Eyes 4: Spontaneous eye opening 3: Eye opening in response to speech 2: Eye opening in response to pain 1: No eye opening Voice 5: Oriented 4: Confused conversation 3: Inappropriate speech 2: Incomprehensible speech 1: None Motor 6: Obeying commands 5: Localising response to pain 4: Withdraws to pain 3: Flexor response to pain 2: Extensor posturing to pain 1: No response to pain Glascow Coma Scale

25
How do we know there’s raised raised ICP? ICU! Monitoring of ICP is integral to treatment Monitor ICP and BP to determine CPP Many Types of monitors

26
Indications for ICP monitoring 1.History 2.Clinical findings 3.Imaging

27
CT

28
Treatment FIX THE CAUSE! REMOVE THE BLOOD CLOT RESECT THE TUMOUR SHUNT THE CSF TREAT THE METABOLIC DISORDER

29
Generally.. Apropriate resuscitation (ABC) A – GCS <8, intubate (carefully) B – Give O2 C – Ensure good end organ perfusion....and treat the raised ICP!
 A – GCS <8, intubate (carefully) B – Give O2 C – Ensure good end organ perfusion....and treat the raised ICP!.")
30
Specifically.. Sedation Elevate the head Hyperventilation Mannitol Removal of CSF Decompressive craniectomy

31
Sedation -Reduce metabolic demand -Reduce venous congestion -Reduce sympathetic response of hypertension and tachycardia

32
Position Elevate head to maximise venous outflow (as long as cerebral perfusion pressure remains appropriate) Minimise stimuli that can induce Valsalva responses (eg endotracheal suctioning)
 Minimise stimuli that can induce Valsalva responses (eg endotracheal suctioning)")
33
Mannitol Reduces brain volume by drawing free water our of the tissue and into the circulation Quick acting and Effects short lived Problems – Can lower BP and therefore CPP

34
Mechanical Hyperventilation Lowering PaCO2 to 26 to 30 mmHg has been shown to rapidly reduce ICP through vasoconstriction and a decrease in the volume of intracranial blood. Effects short lived. Used as an urgent intervention, not on a chronic basis. May cause critical decrease in local cerebral perfusion (minimise use in TBI or actue stroke)
.")
35
Removal of CSF Ventriculostomy to remove CSF http://www.uptodate.com/contents/image?imageKey=NEURO%2F56391&topicKey=NEURO%2F1659&rank=1%7E150&source=see_link&search=i cp&utdPopup=true

36
Decompressive craniectomy Circumvents Monroe-Kellie doctrine Lowers ICP by 70% Improves brain tissue oxygenation

37
Summary Management requires -Recognition -Monitoring -Therapy aimed at reducing ICP and treating the underlying cause

38
Neurosurgical Pop Quiz ‘Wacky, Wet and Wobbly’ is a good way to remember the symptoms of A. Someone with a weak bladder who’s had too many beers B. An overweight delirious patient coming out of a pool C. Normal Pressure Hydrocephalus

39
Neurosurgical Pop Quiz Which surgeon is known as ‘the father’ of modern neurosurgery?

40
Harvey Cushing

41
Questions?

Similar presentations





>")













