Download presentation
Presentation is loading. Please wait.

1
Celiac Disease Gluten Sensitive Enteropathy

2
Celiac Disease: Immune mediated enteropathy caused by permanent sensitivity to gluten in genetically susceptible individuals. Pathogenesis: – –Gluten is the protein found in the grain of wheat, barley, rye. – –Gluten is a large complex molecule consist of four heterogeneous classes of protein (Gliadin, Glutenine, Albumin & Globulin)
.")
3
Celiac disease Autoimmune disorder with a prevalence of approximately 0.5 to 1 percent. (1 in every 100-200 persons) Inappropriate immune response to the dietary protein gluten, which is found in rye, wheat, and barley. After absorption in the small intestine these proteins interact with the antigen-presenting cells in the lamina propria causing an inflammatory reaction that targets the mucosa of the small intestine. Manifestations range from no symptoms to overt malabsorption with involvement of multiple organ systems and an increased risk of some malignancies.
 Inappropriate immune response to the dietary protein gluten, which is found in rye, wheat, and barley. After absorption in the small intestine these proteins interact with the antigen-presenting cells in the lamina propria causing an inflammatory reaction that targets the mucosa of the small intestine. Manifestations range from no symptoms to overt malabsorption with involvement of multiple organ systems and an increased risk of some malignancies..")
4
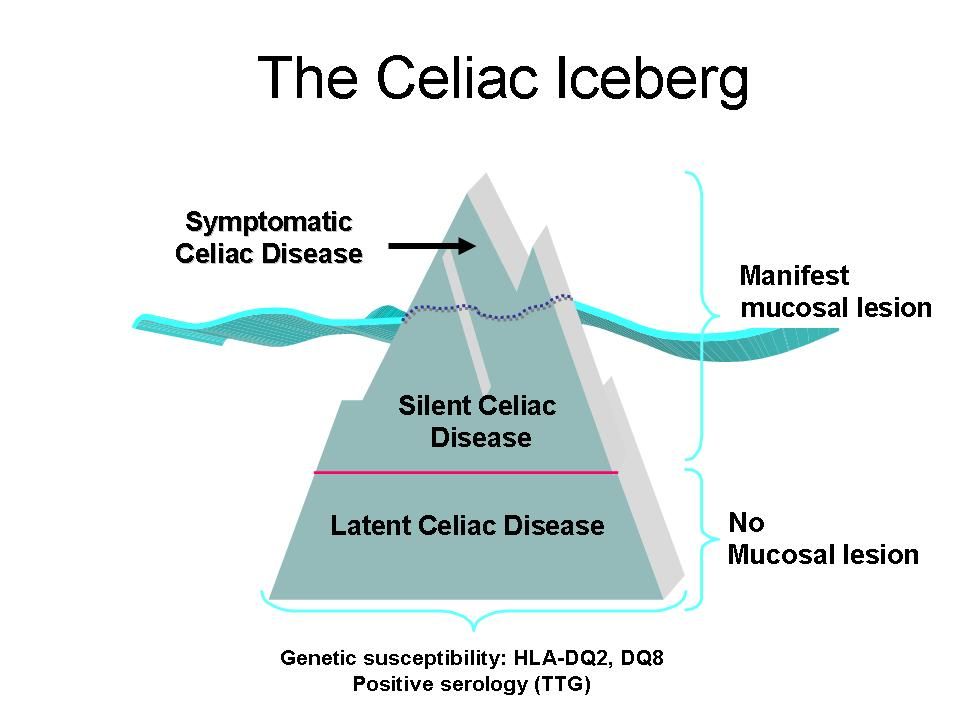
Most patients with celiac disease express human leukocyte antigen (HLA)-DQ2 or HLA-DQ8, which facilitate the immune response against gluten proteins Concordance rates of 70 to 75 % among monozygotic twins and 5 to 22 % among first-degree relatives.
-DQ2 or HLA-DQ8, which facilitate the immune response against gluten proteins Concordance rates of 70 to 75 % among monozygotic twins and 5 to 22 % among first-degree relatives.")
5
Associated Disorders with Celiac Disease(extraintestinal) Dermatitis Herpitiformis. Insulin Dependent -Diabetes Mellitus autoimmune thyroid disesae. autoimmune thyroid disesae. Selective IgA deficiency IgA Nephropathy. Down’s Syndrome. Primary Biliary Cirrhosis & Sclerosing Cholangitis. Sjogren’s Syndrome, alopecia areata, Addison’s disease, epilepsy and post. Cerebral calcification. First-degree relative with celiac disease

7
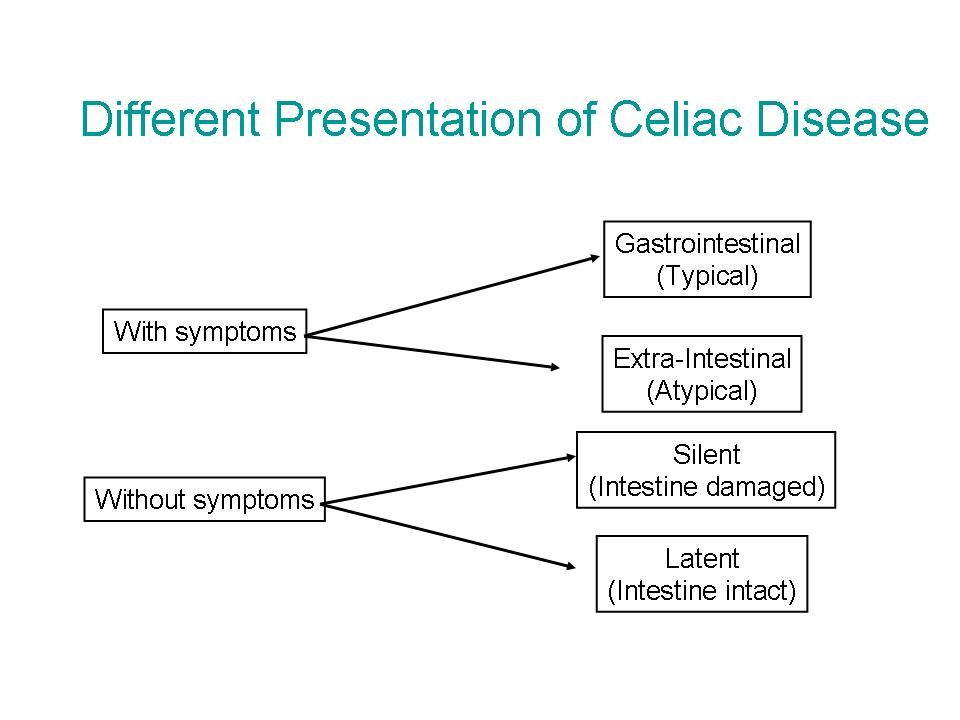
Clinical Features: Age of onset : variable, most children present between one & five years of age but they may present for the first time at any time from infancy to old age. Classic GI pediatric cases usually appear in children aged 9-18 months. Age of onset : variable, most children present between one & five years of age but they may present for the first time at any time from infancy to old age. Classic GI pediatric cases usually appear in children aged 9-18 months. “ Latent interval ”: the time period between the introduction of gluten into the diet and the development of clinical manifestation, varies from months to years. “ Latent interval ”: the time period between the introduction of gluten into the diet and the development of clinical manifestation, varies from months to years.

8
Silent Celiac Disease: Abnormal small bowel mucosa characteristic of celiac disease but the child is Asymptomatic. Silent Celiac Disease: Abnormal small bowel mucosa characteristic of celiac disease but the child is Asymptomatic. Latent Celiac Disease: The small intestinal mucosa shows no flat villi but abnormal in the form of increasing intraepithelial lymphocyte in addition to positive circulating antigliadin or antiendomysial antibodies. Latent Celiac Disease: The small intestinal mucosa shows no flat villi but abnormal in the form of increasing intraepithelial lymphocyte in addition to positive circulating antigliadin or antiendomysial antibodies.

10
Signs and Symptoms Common Diarrhea Diarrhea Fatigue and muscle wasting Fatigue and muscle wasting Borborygmus Borborygmus Abdominal pain Abdominal pain Weight loss, FTT and short stature Weight loss, FTT and short stature Abdominal distention Abdominal distention Flatulence FlatulenceUncommon Osteopenia/ osteoporosis Abnormal liver function Nausea and Vomiting Dental enamel hypoplasia Iron-deficiency anemia resistant to treatment Neurologic dysfunction: ataxia, epilepsy, PNP Constipation Delayed puberty Psychiatric disorders Up to 38 % Asymptomatic

11
Diarrhea: The most common presentation Acute, chronic or recurrent Stool is characteristically pale, loose and very offensive, often one large bulky stool, but could more frequent, some children might have recurrent attacks of more severe diarrhea. Few children with CD have constipation. Stool is characteristically pale, loose and very offensive, often one large bulky stool, but could more frequent, some children might have recurrent attacks of more severe diarrhea. Few children with CD have constipation.

12
Diagnosis of Celiac Disease Clinical picture. Small intestinal biopsy: the gold standard. Serological markers: IgA Antiendomysial, IgA and IgG antigliadin,and IgA Anti-tissue transglutaminase antibodies. + Tissue transglutaminase (tTG) antibodies had sensitivity and specificity > 95%. +Testing for gliadin antibodies is no longer recommended because of the low sensitivity and specificity for celiac disease. +The tTG antibody test is less costly because it uses an enzyme-linked immunosorbent assay; it is the recommended single serologic test for celiac disease screening in the primary care setting.
 antibodies had sensitivity and specificity > 95%. +Testing for gliadin antibodies is no longer recommended because of the low sensitivity and specificity for celiac disease. +The tTG antibody test is less costly because it uses an enzyme-linked immunosorbent assay; it is the recommended single serologic test for celiac disease screening in the primary care setting..")
13
SMALL BOWEL BIOPSY Required to confirm the diagnosis of celiac disease for most patients. Should also be considered in patients with negative serologic test results who are at high risk or in whom the physician strongly suspects celiac disease. Findings: -Short, flat villi -increased number of lymphocytes in the epithelial layer -crypt hyperplasia -crypt hyperplasia

14
Reported causes of flat small intestinal mucosa in childhood: Celiac Disease Celiac Disease Cow’s milk and Soy protein allergy. Cow’s milk and Soy protein allergy. Gastroenteritis and post enteritis syndromes. Gastroenteritis and post enteritis syndromes. Giardiasis. Giardiasis. Autoimmune enteropathy. Autoimmune enteropathy. Microvillous atrophy. Microvillous atrophy. Acquired hypogammaglobulinemia. Acquired hypogammaglobulinemia. Protein-energy malnutrition. Protein-energy malnutrition.

15
Normal small intestine Celiac DiseaseVillous atrophy Normal villi

16
Differential Diagnosis of Celiac Disease Anorexia nervosa Autoimmune enteropathy Bacterial overgrowth Collagenous sprue Crohn's disease Giardiasis Human immunodeficiency virus enteropathy Hypogammaglobulinemia Infective gastroenteritis Intestinal lymphoma Irritable bowel syndrome Ischemic enteritis Lactose intolerance Pancreatic insufficiency Soy protein intolerance Tropical sprue Tuberculosis Whipple's disease Zollinger-Ellison syndrome

17
Patient presents with symptoms of celiac disease Perform serologic IgA tTG antibody testing Positive Negative Small bowel biopsy High clinical suspicion? Positive Negative Small bowel biopsy Low probability of celiac disease; consider total IgA test to R/O IgA deficiency Dx confirmed, Gluten-free diet F/U and consider Other dx, consider Repeat bx Positive Negative Tx and monitor Celiac ruled out, Look for other cause Improvement? Yes No Dx confirmed Evaluate for possible secondary cause of symptoms Yes No Evaluation for Celiac Disease

18
Treatment Avoidance of food products that contain gluten proteins for life: Improve the appetite, Improve the appetite, decrease the diarrhea, decrease the diarrhea, reverse osteopenia, reverse osteopenia, prevent lymphoma, prevent lymphoma, enhance appropriate growth and puberty enhance appropriate growth and puberty Key elements to successful treatment include the motivation of the patient, the attentiveness of the physician to comorbidities that need to be addressed. Formal consultation with a trained dietitian is necessary. National celiac disease support organizations can provide patients invaluable resources for information and support. Replacement of nutritional deficiencies as vitamins, iron, calories

19
COMORBIDITIES Osteoporosis (common finding) Thyroid dysfunction Deficiencies in folic acid, vitamin B12, fat- soluble vitamins, and iron Increased mortality due to increased risk of malignancy Intestinal lymphoma (3-6x more likely) Intestinal lymphoma (3-6x more likely) Most common is intestinal non- Hodgkin's lymphoma Most common is intestinal non- Hodgkin's lymphoma
 Thyroid dysfunction Deficiencies in folic acid, vitamin B12, fat- soluble vitamins, and iron Increased mortality due to increased risk of malignancy Intestinal lymphoma (3-6x more likely) Intestinal lymphoma (3-6x more likely) Most common is intestinal non- Hodgkin s lymphoma Most common is intestinal non- Hodgkin s lymphoma")
20
Screening Screening an asymptomatic patient for celiac disease must be weighed against the psychological, emotional, and economic impact of a false positive result. Also, it would necessitate further evaluation with small bowel biopsy. The need to follow a strict diet indefinitely can adversely affect the patient's perceived quality of life. Routine screening of the general population is not recommended. Persons at high risk for celiac disease who exhibit any level of symptoms, appropriate testing is indicated.

Similar presentations






 Autoimmune disorder with a prevalence of approximately 0.5 to 1 percent in the United States. (1 in.>")












