Download presentation
Presentation is loading. Please wait.

1
Lecture – 8: Acid Base Balance RENAL SYSTEM PHYSIOLOGY Dr Shahab Shaikh PhD, MD College of Medicine Al Maarefa Colleges of Science & Technology College of Medicine Al Maarefa Colleges of Science & Technology

2
OBJECTIVES Identify the normal range of pH values, and the upper and lower limits compatible with life. Identify the role of kidney in regulation of acid base balance Explains the mechanism of reabsorption of HCO3- and secretion of H+ by nephron Describe the adjustments in filtered load and HCO3 reabsorption (H+ secretion) by alterations in systemic acid-base balance. Describe net acid excretion by the kidneys, treatable acid, the importance of urinary buffers, and the production and excretion of ammonium.
 by alterations in systemic acid-base balance. Describe net acid excretion by the kidneys, treatable acid, the importance of urinary buffers, and the production and excretion of ammonium..")
3
Introduction Acid-Base Balance involves various physiologic processes responsible for the maintenance of the acidity of body fluids at levels that allow optimal function of the whole individual. The importance of Acid-Base regulation stems from the critical importance of the hydrogen ion (H + ) concentration on the operation of many cellular enzymes and function of vital organs. The task of maintaining Acid-Base homeostasis is large because... – Metabolic pathways are continuously consuming or producing H + – The daily load of waste products for excretion in the form of volatile and fixed acids is substantial – Based on diet, Ingestion of acidic substances may be variable and huge.
 concentration on the operation of many cellular enzymes and function of vital organs. The task of maintaining Acid-Base homeostasis is large because... – Metabolic pathways are continuously consuming or producing H + – The daily load of waste products for excretion in the form of volatile and fixed acids is substantial – Based on diet, Ingestion of acidic substances may be variable and huge..")
4
Acid-Base Balance Acid–Base balance refers to the precise regulation of free (unbound) hydrogen ion concentration [H + ] in the body fluids. Acids are hydrogen-containing substances that dissociate in solution to liberate free H + A strong acid has a greater tendency to dissociate in solution than a weak acid does. The extent of dissociation for a given acid is always constant and is expressed as its dissociation constant (K)
![Acid-Base Balance Acid–Base balance refers to the precise regulation of free (unbound) hydrogen ion concentration [H + ] in the body fluids.](http://images.slideplayer.com/29/9490612/slides/slide_4.jpg "Acids are hydrogen-containing substances that dissociate in solution to liberate free H + A strong acid has a greater tendency to dissociate in solution than a weak acid does. The extent of dissociation for a given acid is always constant and is expressed as its dissociation constant (K).")
5
Acid-Base Balance Base is a substance that can combine with a free H + and thus remove it from solution. A strong base is one that can bind H + more readily than a weak base.

6
The pH Concept The pH is a measurement without units and represents the free Hydrogen ion concentration [H + ] within a given solution. The concept of pH was developed to express the low value of [H + ] more conveniently. pH represents the inverse logarithmic scale of hydrogen ion activity pH = log 10 1/[H + ] = - log 10 [H + ] The fact that the pH scale is inverse & logarithmic (log 10) means that for each reduction of one in pH, there is a 10-fold increase in the hydrogen ion concn.
![The pH Concept The pH is a measurement without units and represents the free Hydrogen ion concentration [H + ] within a given solution.](http://images.slideplayer.com/29/9490612/slides/slide_6.jpg "The concept of pH was developed to express the low value of [H + ] more conveniently. pH represents the inverse logarithmic scale of hydrogen ion activity pH = log 10 1/[H + ] = - log 10 [H + ] The fact that the pH scale is inverse & logarithmic (log 10) means that for each reduction of one in pH, there is a 10-fold increase in the hydrogen ion concn..")
7
The pH Concept The pH of pure H 2 O is 7.0, which is considered chemically neutral. Because an equal number of acidic H + and basic OH - are formed, H 2 O is neutral, being neither acidic nor basic. Solutions having a pH less than 7.0 contain a higher [H + ] than pure H 2 O and are considered acidic. Solutions having a pH value greater than 7.0 have a lower [H + ] than pure H 2 O and are considered basic, or alkaline.

8
The normal pH The [H + ] in the ECF is normally: = 0.00000004 mol/L = 0.00004 mmol/L = 40 nmol/L = 7.4 on pH scale Normal pH range in body is 7.35 - 7.45. An arterial pH of less than 6.8 or greater than 8.0 is not compatible with life.
![The normal pH The [H + ] in the ECF is normally: = mol/L = mmol/L = 40 nmol/L = 7.4 on pH scale Normal pH range in body is](http://images.slideplayer.com/29/9490612/slides/slide_8.jpg "An arterial pH of less than 6.8 or greater than 8.0 is not compatible with life..")
9
pH: physiological importance The pH has two major physiological effects: – Firstly, the pH will affect the ionization status of most molecules within the physiological range and is responsible for certain molecules remaining trapped within the cell. – Secondly, Every protein & enzyme has an optimal pH, and activity falls off either side of this optimal value. The majority of the body’s enzyme systems work optimally at physiological pH.

10
pH: physiological importance Consequences of fluctuations in pH: – Changes in excitability of nerve and muscle cells – Marked influence on enzyme activity – Changes influence K + levels in body In general, body produces more acids than bases. Sources of H+ in the body: – Volatile acid CO2 Carbonic acid formation CO2 + H20 ↔ H2CO3 ↔ H+ + HCO3- – Non volatile acids (fixed Acids) Inorganic acids produced during metabolism (sulfuric acid & phosphoric acid) Organic acids resulting from intermediary metabolism( lactic acid)
 Inorganic acids produced during metabolism (sulfuric acid & phosphoric acid) Organic acids resulting from intermediary metabolism( lactic acid).")
11
pH: Defense Against Changes Lines of Defense Against pH Changes: 1.Chemical buffers: – function almost immediately (seconds to minutes). 2.Respiratory mechanisms: – take minutes to hours. 3.Renal mechanisms: – may take hours to days.

12
1.Chemical Buffers First line of defense against pH change. Does not eliminate H+ from or add them to the body but only keep them tied up until balance can be reestablish ed by other mechanism s.

13
Importance of Buffer Systems Normal H + concentration = 0.00004 mmol/L Amount of non-volatile acid produced ~ 80 mmol/day 80 mmol /42 L = 1.9 mmol/L = 47,500 times > normal H + concentration

14
2.Respiratory Mechanism Second line of defense again changes in pH Acts at a moderate speed (minutes to hours) Regulates pH by controlling rate of CO 2 removal
 Regulates pH by controlling rate of CO 2 removal")
15
3.Renal Mechanism Third line of defense against change in hydrogen ion concentration. Kidneys require hours to days to compensate for changes in body-fluid pH. Controls pH of body fluids by adjusting – H + excretion – HCO 3 - excretion/ reabsorption – Production of new HCO 3 - – Ammonia secretion

16
H + secretion In luminal membrane H + ATPase pump Na – H + Antiporter

17
Mechanism of HCO 3 - Reabsorption and Na + - H + Exchange

18
H + secretion in Distal & Collecting Tubule

19
H + secretion and excretion couples with addition of HCO 3 to plasma

20
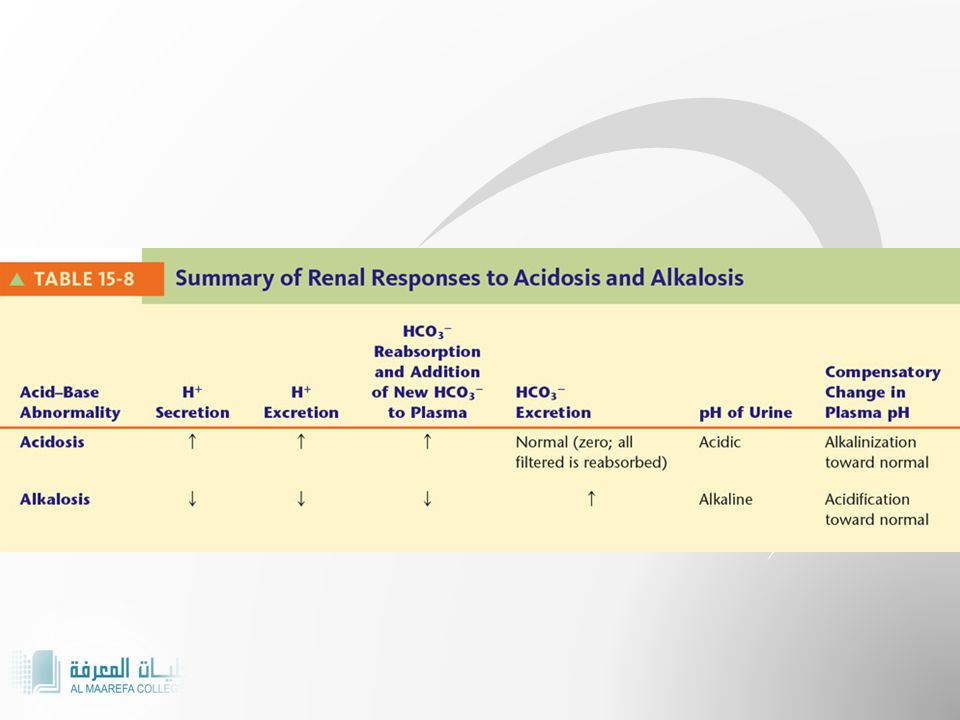
Renal handling of H + during acidosis and alkalosis Under normal circumstances proximal tubular cells and alpha intercalated cells promotes Net H + secretion HCO 3 - reabsorption This pattern of activity adjusted when pH deviates

21
Control of rate of tubular secretion & H+ reabsorption

23
Other Urinary Buffers the minimal urine pH is about 4.5. In order to excrete more H +, the acid must be buffered in tubular lumen. H + secreted into the tubular tubule and combines with HPO 4 -2 or NH 3. Phosphate is mostly ICF buffer and also the most abundant renal tubular buffer HPO 4 -2 + H + H 2 PO 4 -2 NH 3 + H + NH 4 +

24
Buffering of Secreted H + by Filtered phosphate (NaHPO 4 - ) and Generation of “New” HCO 3 - “New” HCO 3 -
 and Generation of New HCO 3 - New HCO 3 -")
25
Production and Secretion of NH 4 + and HCO 3 - by Proximal, Thick Loop of Henle, and Distal Tubules “New” HCO 3 - H + +NH 3

26
Buffering of Hydrogen Ion Secretion by Ammonia (NH 3 ) in the Collecting Tubules “New” HCO 3 - Figure 30-9; Guyton and Hall
 in the Collecting Tubules New HCO 3 - Figure 30-9; Guyton and Hall")
27
Henderson- Hasselbach’s Equation Normal levels: HCO3 = 21 – 28 mEq/L PCO2 = 35 – 45 mmHg

28
Acid-Base Imbalances Can arise from either respiratory dysfunction or metabolic disturbances Deviations divided into four general categories – Respiratory acidosis – Respiratory alkalosis – Metabolic acidosis – Metabolic alkalosis

29
Respiratory Acidosis Result of abnormal CO 2 retention arising from hypoventilation Possible causes – Lung disease – Depression of respiratory center by drugs or disease – Nerve or muscle disorders that reduce respiratory muscle activity – Holding breath

30
Respiratory Acidosis Compensations Chemical buffers immediately take up additional H + Kidneys are most important in compensating for respiratory acidosis

31
Respiratory Alkalosis Primarily due to excessive loss of CO 2 from body as result of hyperventilation Possible causes – Fever – Anxiety – Aspirin poisoning – Physiologic mechanisms at high altitude

32
Respiratory Alkalosis Compensations Chemical buffer systems liberate H + If situation continues a few days, kidneys compensate by conserving H + and excreting more HCO 3 -

33
Metabolic Acidosis Includes all types of acidosis other than those caused by excess CO 2 in body fluids Causes – Severe diarrhea – Diabetes mellitus – Strenuous exercise – Uremic acidosis

34
Metabolic Acidosis Compensations Buffers take up extra H + Lungs blow off additional H + generating CO 2 Kidneys excrete more H + and conserve more HCO 3 -

35
Metabolic Alkalosis Reduction in plasma [H + ] caused by relative deficiency of noncarbonic acids Causes – Vomiting – Ingestion of alkaline drugs
![Metabolic Alkalosis Reduction in plasma [H + ] caused by relative deficiency of noncarbonic acids Causes – Vomiting – Ingestion of alkaline drugs](http://images.slideplayer.com/29/9490612/slides/slide_35.jpg "Metabolic Alkalosis Reduction in plasma [H + ] caused by relative deficiency of noncarbonic acids Causes – Vomiting – Ingestion of alkaline drugs")
36
Metabolic Alkalosis Compensations Chemical buffer systems immediately liberate H + Ventilation is reduced If condition persists for several days, kidneys conserve H + and excrete excess HCO 3 - in the urine

37
Analysis of Simple Acid-Base Disorders Analysis of Simple Acid-Base Disorders Figure 30-10; Guyton and Hall

38
References Human physiology by Lauralee Sherwood, 8 th edition Text Book Of Physiology by Guyton & Hall, 11 th edition Review of Medical Physiology by Ganong. 24 th edition

39
39 THANK YOU

Similar presentations






![1. pH = - log [H + ] H + is really a proton Range is from 0 - 14 If [H + ] is high, the solution is acidic; pH < 7 If [H + ] is low, the solution.](/15/4651316/big_thumb.jpg "1. pH = - log [H + ] H + is really a proton Range is from 0 - 14 If [H + ] is high, the solution is acidic; pH < 7 If [H + ] is low, the solution.>")

![H + Homeostasis by the Kidney. H + Homeostasis Goal: To maintain a plasma (ECF) pH of approximately 7.4 (equivalent to [H + ] = 40 nmol/L Action needed:](/15/4651439/big_thumb.jpg "H + Homeostasis by the Kidney. H + Homeostasis Goal: To maintain a plasma (ECF) pH of approximately 7.4 (equivalent to [H + ] = 40 nmol/L Action needed:>")






 H + concentration in the body.>")
![Renal Acid-Base Balance. Acid An acid is when hydrogen ions accumulate in a solution. It becomes more acidic [H+] increases = more acidity CO 2 is an.](/20/5962628/big_thumb.jpg "Renal Acid-Base Balance. Acid An acid is when hydrogen ions accumulate in a solution. It becomes more acidic [H+] increases = more acidity CO 2 is an.>")

>")
