Download presentation
Presentation is loading. Please wait.

1
Case scenario- Multiple trauma
M K Alam

2
Case scenario 1 A 20 year old man was brought to ED of a small hospital. His small car skidded and hit a lamp post.

3
Report from ambulance man
Not wearing seat belt Front wind screen was shattered BP 90/60 mmHg Pulse 112/ min RR 32/ min Management: Oral airway, cervical collar, O₂, iv fluid, spinal board

4
Pre-hospital management
Oral airway Cervical collar IV crystalloid infusion O₂ Spinal board

5
Vital signs on arrival to ED
BP 90/66 mmHg Pulse 116/ min RR 34/ min Temperature 36.8° C What to do?

6
A Unresponsive to your questions. Bleeding from facial lacerations
What to do?

7
A- Airway Clear airway by suctioning Unstable jaw Oxygen Open collar
Distended neck vein Orotracheal intubation Surgical cricothyroidotomy

8
Slight improvement in respiration.
What to do?

9
B- Breathing Right chest: Diminished movement on
Soft tissue crepitation Hyper resonant Diminished breath sound Normal heart sound

10
? Diagnosis Tension pneumothorax Management Needle thoracocenteasis ICT Improvement in RR (22/ min) BP - 98/ 66 mm Hg, pulse 112/ min. What next? What other life threatening injuries?

11
C- Circulation Why hypotension? ?Haemorrhage ?Cardiogenic ?Neurogenic

12
C- Circulation 2nd IV line started (1st iv line – pre-hospital)
2L RL- rapid infusion Pulse oximetry, ECG ? Foley catheter (?PR exam)- clear urine Facial laceration bleeding- minimal Abdomen slightly distended, pelvis stable Limbs- no swelling, deformity or laceration BP – 100/ 70 mmHg, Pulse 98/ min. NG tube (? Which route) FAST
- clear urine. Facial laceration bleeding- minimal. Abdomen slightly distended, pelvis stable. Limbs- no swelling, deformity or laceration. BP – 100/ 70 mmHg, Pulse 98/ min. NG tube ( Which route) FAST.")
13
FAST- Focused abdominal sonography in trauma
Rapid & accurate. Sensitivity up to 99%. Detects small amount (100 ml) of blood. Four views: 1.Pericardiac 2.Perihepatic Perisplenic 4.Pelvic Helpful in management of unstable patients.
 of blood. Four views: 1.Pericardiac 2.Perihepatic 3 Perisplenic 4.Pelvic. Helpful in management of unstable patients.")
14
FAST

15
FAST Free fluid in abdomen Multiple liver laceration Management ?

16
D- Disability What to do?

17
Glasgow Coma Scale (GCS), Total = 15
Eye response Vocal response Motor response Spontaneous 4 Oriented Obeys commands 6 To voice Confused Purposeful movement to pain 5 To pain Inappropriate words 3 Withdraw from pain 4 None Incomprehensible words 2 Flexion to pain *** None Extension to pain None

18
D- Disability E2, M4, V1 Pupil- R= 4 mm, L= 5.5mm, both reacting to light >1 mm suggests intracranial injury Neurosurgery consultation

19
E- Exposure/ environment control
What to do?

20
E- Exposure/ environment control
Full exposure Areas missed? Protect from hypothermia.

21
Preparation for Surgery
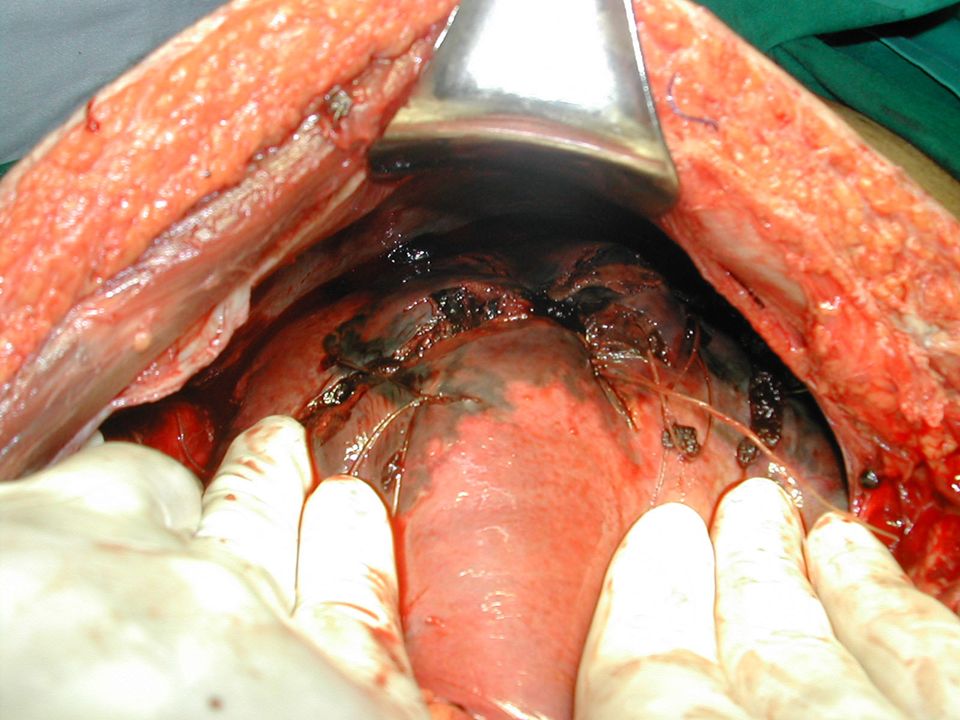
?Priority Consent Blood Skin preparation Laparotomy: ? Incision Intraoperative: Suture liver laceration, perihepatic packing

22
Liver injury Spontaneous hemostasis- 50% of small lacerations.
Profuse bleeding from deep hepatic lacerations. Mortality : 8%- 10% Morbidity : 18%-30%. Diagnosis: Hemodynamically unstable- FAST Hemodynamically stable- FAST, CT scan Management based on hemodynamic status

23
Liver injury- pathophysiology
Susceptible to injury due to large size( g) Covered by bony thoracic cage Injury frequency - only 2nd after spleen( personal series) Highly vascular- only 4% of body weight but 28% of total body blood flow Double blood supply- portal vein & hepatic artery Draining hepatic veins- short and thin walled
 Covered by bony thoracic cage. Injury frequency - only 2nd after spleen( personal series) Highly vascular- only 4% of body weight but 28% of total body blood flow. Double blood supply- portal vein & hepatic artery. Draining hepatic veins- short and thin walled.")
24
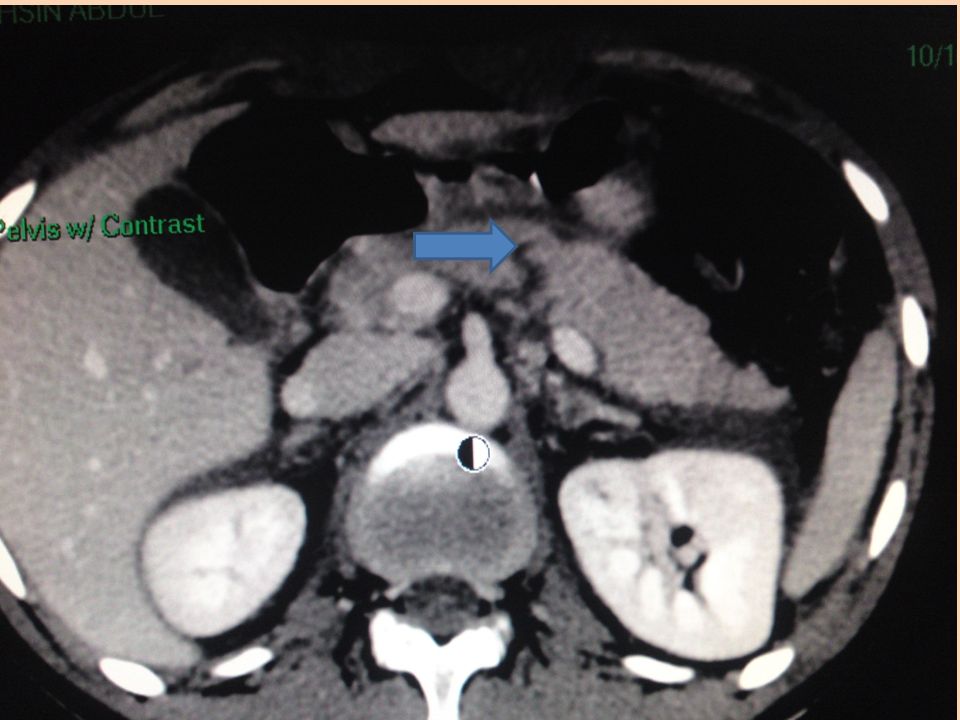
Liver injury- CT scan

25
Liver injury- Non-operative management
Hemodynamically stable. patients CT scan. No other indications for abdominal exploration. ICU admission for close observation. Serial hemoglobin estimation. Transfusion requirements of <2 units of blood. Surgery- if become unstable.

26
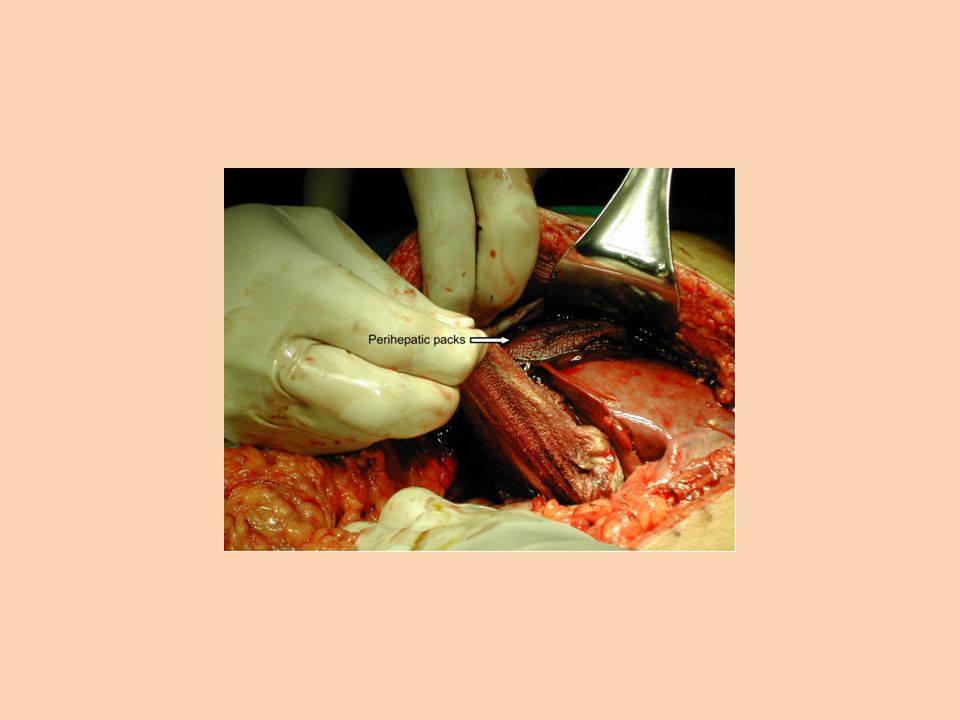
Liver injury-Surgical management
Principles of surgical management: control of bleeding, removal of devitalized tissue, and adequate drainage. Bleeding vessels & biliary radicles are individually ligated. Pringle’s maneuver. Perihepatic packing- fail to control bleeding. Packs removed in 48 hours.

30
Abdominal injuries 25% of all trauma victims require abdominal exploration. PE: inadequate to identify intra-abdominal injuries Diagnostic modalities- CXR, FAST, DPL,CT & laparoscopy Blunt trauma: Hemodynamically stable- FAST , CT scan Hemodynamically unstable- FAST

31
Diagnostic peritoneal lavage (DPL)
Insert catheter below umbilicus under LA. Bloody aspirate- laparotomy. 1L NS infusion into peritoneum. Returning fluid is bloody- positive lavage. Rapid and safe Do not determine origin of blood Too sensitive Does not evaluate retroperitoneal injury Replaced by FAST and CT scan

32
Diagnostic peritoneal lavage (DPL)
")
33
Splenic injury Most frequently injured in blunt trauma (personal series) History of injury to the left side of the chest, flank, or left upper part of the abdomen Bruising, pain tenderness- lower chest and upper abdomen on left side Diagnosis- CT in hemodynamically stable patients FAST or exploratory laparotomy in an unstable patients

34
Splenic injury (CT scan)
")
35
Splenic injury-Non-surgical management (70%)
Hemodynamically stable. FAST, CT scan. No other intra-abdominal injury requiring operation ICU admission for continuous monitoring. Serial hemoglobin. Repeated abdominal assessment. If hypotension develops - for surgery.

36
Splenic injury-Surgical management
Hemodynamically unstable. FAST: splenic injury, free fluid (hemoperitoneum). Surgery- splenectomy . Polyvalent pneumococcal vaccine (pneumovax).
. Surgery- splenectomy . Polyvalent pneumococcal vaccine (pneumovax).")
37
Pancreatic injuries Uncommon. Penetrating injury or direct blow.
Diagnosis: difficult CT scan, elevated serum amylase may help No duct injury: simple drainage Ductal injury: distal resection

39
Bowel injuries Mostly- penetrating trauma.
Less common after blunt trauma. Features of peritonitis. CT scan free air in peritoneum/ contrast leak. Small bowel: Suture repair Colon: Suture repair ± proximal colostomy

40
Bowel injuries CT: contrast leak (C) & free air Intraoperative
 & free air Intraoperative")
41
Renal injuries Minor- renal contusion (85%) Conservative management
Major: Deep medullary injuries with extravasation Vascular injuries Surgical repair

42
Case scenario- 2 A young male was stabbed in a car park after a dispute over parking space
ABCDE: Fully conscious, hemodynamically stable, well oriented of time and place Abdomen: 2 cm wound just above the umbilicus. Abdomen moving well with respiration. No active bleeding from the wound. Non tender Bowel sound present

43
Penetrating Abdominal injuries
Gun shot injuries- urgent surgery Stab (knife) injury: Hemodynamically stable- wound exploration under LA, CT scan, Surgery- if intra-abdominal injuries found. Hemodynamically unstable- surgery
 injury: Hemodynamically stable- wound exploration under LA, CT scan, Surgery- if intra-abdominal injuries found. Hemodynamically unstable- surgery.")
44
Thank you!

Similar presentations




 advance ET tube B) needle thoracostomy.>")















