Download presentation
Presentation is loading. Please wait.

2
Enteral Nutrition in Paediatric

3
EN in PAEDIATRICS Lecture objectives Nutritional support in children EN: Indications & contraindications How to choose site & route Selection of formula Complications

4
Nutritional Support in Sick Children GOALS To provide energy & nutrients to support: optimal growth neuromotor development minimize gastrointestinal symptoms promote normal feeding habits & skills To treat a disease (food allergy in infants, Crohn’s disease......)
")
5
Nutritional Interventions in Sick Children Depend on: Age Clinical picture Possibility of oral intake Absorptive & digestive capacity Dietary habits Costs

7
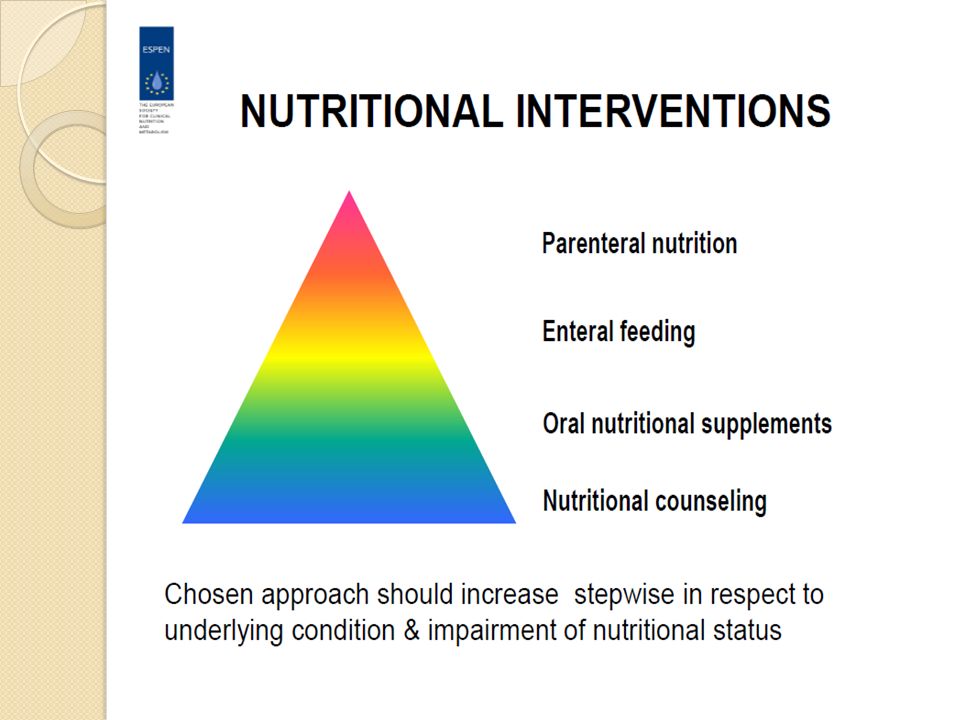
Management strategy: nutritional counselling Get children eat more without unnecessary restrictions simplest, cheapest & safest nutritional support Provide oral nutritional supplement 1. - whole protein based, pediatric formula, nicely flavored, with fibers 2. - energy enriched (1.3-1.5 kcal/ml) if more energy required
 if more energy required.")
8
Enteral Nutrition DEFINITION Feeding directly into stomach or duodenum / jejunum over tube or stoma Oral provision of dietary foods for special medical purposes

9
EN vs. PN: Rule of Thumb improves GUT function limits bacterial translocation & sepsis decreases incidence of multiorgan failure less expensive ENTERAL INTAKE Use GUT whenever possible & as much as possible

10
EN in Paediatrics W H E N?? Not growing well on oral intake Not growing well ??? Growth failure >1 months in child <2 y Growth failure >3 months in child >2 y Change on centile charts >2 growth channels Triceps skinfolds <5th percentile / age EN used as treatment of the disease (allergy, Crohn, Total feeding time >4 h/day in disabled child

11
EN: Clinical Indications

12
EN: Contraindications Necrotizing enterocolitis Intestinal perforation & obstruction Major intra-abdominal sepsis Mechanical & paralytical ileus

13
Selection of Formulae for EN

15
N6 FA Immune system

17
Enteral Formula Selection versus unsupplemented EN formula in: a. patients and healthy controls b. predominant symptom diarrhoea & constipation

18
EN in CHILDREN: Sites for delivery STOMACH physiologic antimicrobial effect gradual release tubes easily placed less diarrhoea, better osmotic tolerance JEJUNUM in patients with high risk of aspiration gastric outlet obstruction High energy and hyperosmolar???

19
Nasoenteral Tubes 1. Nasoenteral tubes 2. Nasogastric 3. Nasoduodenal 4. Nasojejunal short-term nutritional supplementation The tubes are typically made of flexible polyurethane or silicone with a diameter of 1.4 to 4.0 mm

20
EN in CHILDREN: Sites for delivery Silicon PVC Soft, flexible Atraumatic Expensive Long duration (4-6 weeks) Stiff, release phalate Traumatic Cheap Short duration (4-6 d)
 Stiff, release phalate Traumatic Cheap Short duration (4-6 d)")
21
Positioning of NG Tubes Suggested by acid pH (≤5) of the aspirate epigastric auscultation of injected air correct external length of tube If necessary check by abdominal x-ray no aspiration of gastric content pH >5 patient’s condition suggests aspiration
 of the aspirate epigastric auscultation of injected air correct external length of tube If necessary check by abdominal x-ray no aspiration of gastric content pH >5 patient’s condition suggests aspiration")
22
Positioning of the NG tube Measuring tube for children and infants and newborns

23
Administration bolus feedings administered in 5 to 20 minutes expensive than pump or gravity bolus feedings A 60-mL syringe 3-4 time

24
Intermittent Drip allow mobile patients more free time and autonomy compared with continuous A schedule is based on 4-6 feedings per day administered for 20 to 60 minutes. Formula administration is initiated at 100 to 150 mL per feeding aspiration

25
Continuous enteral feeding Continuous drip infusion of formula requires a pump. This method is appropriate for patients who do not tolerate large-volume infusions In SBS, after PN surgery, cancer therapy, or other physiologic (usually18 to 24 hours)
.")
26
PREVENTION & THERAPYCOMPLICATIONS Formula selection & delivery Osmolality, viscosity... Disease specific Gastrointestinal Diarrhoea, nausea, vomitting, Monitoring gastAspiration!! Tube, stoma selection & placement Endoscopy vs. surgery Technical Occlusion, migration, GIT lession Quality control & protocols hygiene Infective Gastroenteritis, septicaemia Monitoring Growth (weight, height/length, skinfolds) Hematology, biochemistry Metabolic Fluid, glucose, electrolytes Trace elements, vitamins TEAM APPROACH!!!Psychological Oral aversion, altered taste Assess elec, ½ -2/3 requirmrnt(60kcaj/kg in 7y) Supp:1mm/kg Na, 4k, 0.6Mg, 1po4, B1 B2 B6 B9 trece elem. Refeeding syndrome(Mg, k,p) annemia,weakness in child with AN, cancer,
 Hematology, biochemistry Metabolic Fluid, glucose, electrolytes Trace elements, vitamins TEAM APPROACH!!!Psychological Oral aversion, altered taste Assess elec, ½ -2/3 requirmrnt(60kcaj/kg in 7y) Supp:1mm/kg Na, 4k, 0.6Mg, 1po4, B1 B2 B6 B9 trece elem. Refeeding syndrome(Mg, k,p) annemia,weakness in child with AN, cancer,.")
27
Disorders where enteral nut needed SBS Severe diarrhoea IBS CF Chronic liver Diseases Abdominal

28
EN in CHILDREN: route PEG / PEJ

29
Management strategy: site & route

30
EN Initiation Gradual increase in rate and concentration Depends on: age clinical condition formula (osmolality !) delivery route (jejunum !)
 delivery route (jejunum !)")
31
Enteral Nutrition in Children 1.Use GUT whenever possible & as much as possible 2. Standard polymeric formulas useful in >90% patients with best cost / benefit ratio 3. EN is safe & effective method of nutr. therap

Similar presentations










, bypassing the oral.>")





 in Critically Ill Patients Liz Goddard.>")



. BMI currently.>")

