Download presentation
Presentation is loading. Please wait.

1
Valvular Heart Disease
Dr James Peerless June 2015

2
Valvular Heart Disease
Valvular heart disease affects 5% of patients >65y in the developed world Stenotic valvular heart disease (AS & MS) are most clinically significant. In assessment: assess the significance of the lesion in relation to the proposed surgery plan according to the haemodynamic picture
 are most clinically significant. In assessment: assess the significance of the lesion in relation to the proposed surgery. plan according to the haemodynamic picture.")
3
Aortic Stenosis

4
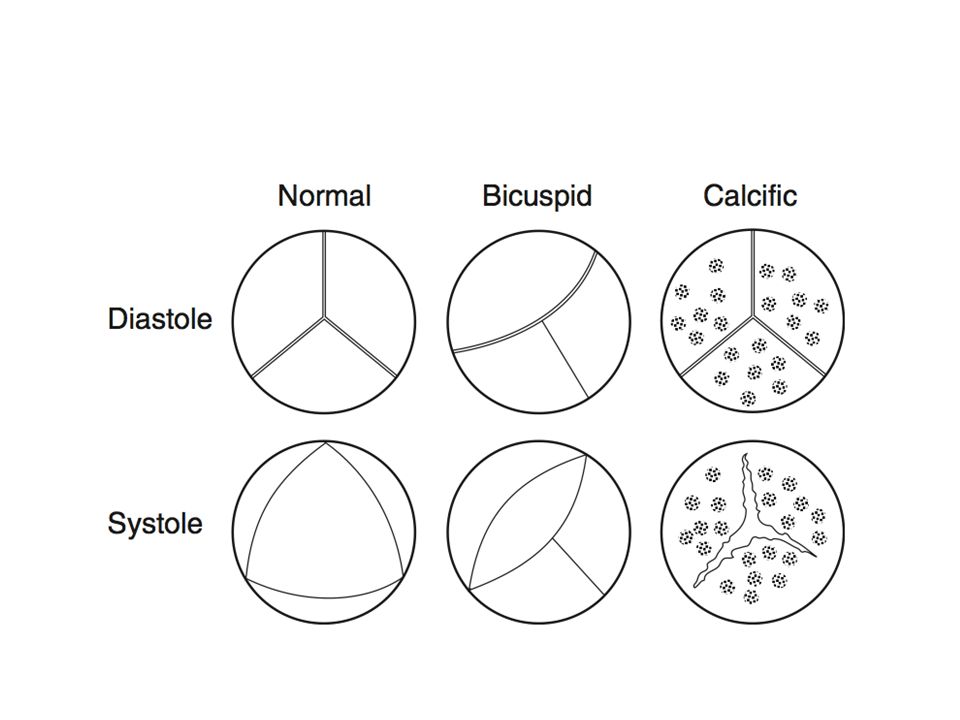
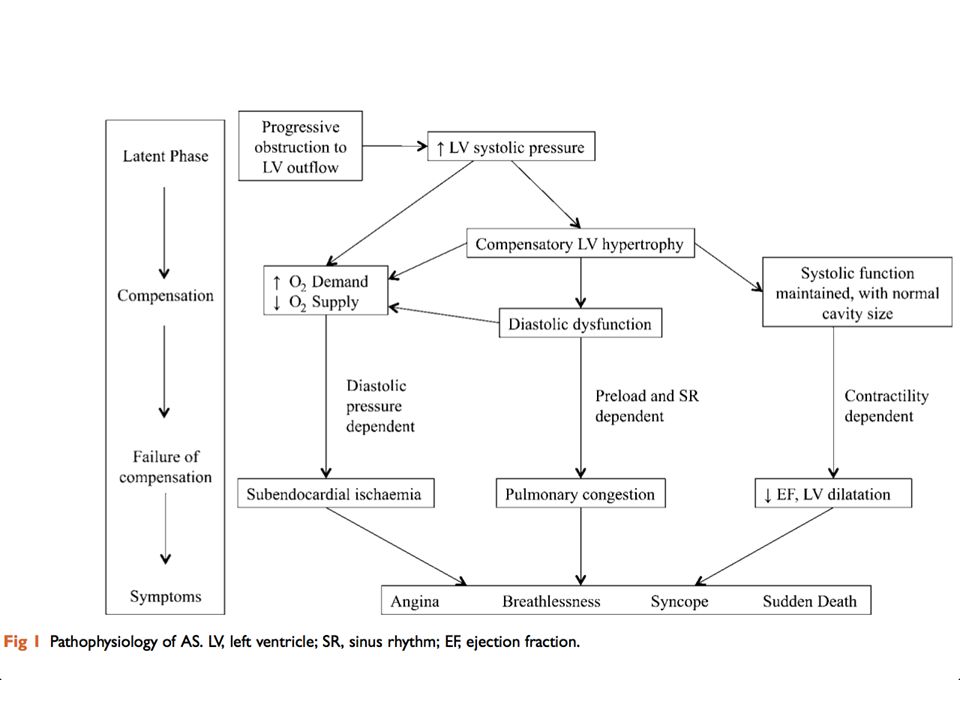
AS - Pathophysiology AS fixed cardiac output
unable to compensate for reduction in SVR caused by the vasodilating effect of GA 2% of >65 have severe AS 4% of >85 have severe AS Male > female Degenerative calcific AS Congenital bicuspid AS (2% of ppln.)
")
6
Presentation History (symptoms correlate poorly with disease severity)
Chest pain Syncope SOB (symptoms correlate poorly with disease severity) Examination Slow rising pulse Narrow PP Ejection sys. murmur
 Examination. Slow rising pulse. Narrow PP. Ejection sys. murmur.")
7
Presentation ECG CXR Echocardiography LVH with strain ?LA enlargement
remains normal until left ventricle begins to fail calcified aortic annulus Echocardiography

8
Grading of AS Normal Mild Moderate Severe Critical Valve Area (cm2)
3 – 4 > 1.5 1 – 1.5 < 1 < 0.6 Peak Gradient (mmHg) < 10 < 40 < 65 > 65 Mean Gradient (mmHg) < 5 < 25 > 40 > 70 Ao Jet Velocity (ms-1) < 2 < 3 < 4 > 4
 < 10. < 40. < 65. > 65. Mean Gradient (mmHg) < 5. < 25. > 40. > 70. Ao Jet Velocity (ms-1) < 2. < 3. < 4. > 4.")
10
Pre-operative Care Assessment of AS severity and LV function if possible, by echo If surgery cannot be delayed, treat as per moderate/severe AS Stenosis typically worsens ~0.1 cm2.yr-1

11
Peri-operative Care Monitoring Goals
To maintain haemodynamic stability A-line CVP (for inotropes, and fluid management) Goals Avoid hypotension ( myocardial hypoperfusion and ischaemia) Maintain SVR, and adequate volume loading Sinus rhythm Low-normal HR Normal electrolyte concentrations
 Goals. Avoid hypotension ( myocardial hypoperfusion and ischaemia) Maintain SVR, and adequate volume loading. Sinus rhythm. Low-normal HR. Normal electrolyte concentrations.")
12
Peri-operative Care Regional anaesthesia must be approached with extreme caution In severe cases, e.g. and including obstetrics, access to CPB should be available.

13
Post-operative Care Low threshold for HDU admission Fluid balance
Appropriate BP Vasoconstrictor infusions may be required Pain management

14
Mitral Stenosis

15
Mitral Stenosis Valve Area/ cm2 Normal Valve 4 – 6 Mild 1.5 – 2.5
Moderate 1.0 – 1.5 Severe < 1

16
Mitral Stenosis Cause Pathophysiology
Normal LV, but is small and poorly filled. Rheumatic fever, streptococcal infection Majority are mixed valve disease Pathophysiology Left atrial dilatation (maintains low PAP) Increasing LAP pulm. HTN Pulm. HTN right heart hypertrophy Secondary RH failure with PV & TV regurg.
 Increasing LAP pulm. HTN. Pulm. HTN right heart hypertrophy. Secondary RH failure with PV & TV regurg.")
17
Presentation History Examination Dyspnoea Haemoptysis
Recurrent bronchitis Fatigue Palpitations Examination Malar flush Peripheral cyanosis Tapping apex beat Low-pitched diastolic murmur Right heart failure

19
Presentation Investigations ECG CXR Echocardiography P mitrale AF
Valve calcification Large LA; evidence of pulmonary congestion Splaying of carina Echocardiography Gradient and valve area measurements

21
Pre-operative Care Hx, Ex, Invx
Patients frequently dyspnoeic from lung transudates Increased work of breathing Reduced compliance Poor functional capacity patients (<4METs) should be considered for MV replacement
 should be considered for MV replacement.")
22
Peri-operative Care Relatively fixed cardiac output, similar to AS.
LV filling is optimised with a slow HR Monitor CVP, treat arrhythmias aggressively. Regional anaesthesia may be very hazardous. Risk of pulm. oedema Large boluses, head-down position Uterine contractions

23
Peri-operative Care Goals Low-normal HR Maintain Sinus rhythm
Adequate preload High-normal SVR Avoid increasing PVR (pH, PaO2, PaCO2)
")
24
MCQs

25
MCQs In assessing severity of aortic stenosis:
The pressure gradient across the valve is the most accurate method. Angiography is not always required. Exercise tolerance is a good measure of severity. The pressure gradient measured at angiography will be higher than that found on the echocardiogram. The pressure gradient severity tends to be over estimated in pregnancy.

26
MCQs Important factors in the intraoperative care of the patient with aortic stenosis include: Avoiding hypotension. Maintaining systemic vascular resistance. Avoiding tachycardias. Never using regional anaesthesia. Avoiding intubation.

27
MCQs When considering the aetiology of aortic stenosis:
Aortic sclerosis is a benign variant. Stenosis is common without calcification. Bicuspid valves are more common in younger patients. Rheumatic disease is a common cause of isolated aortic stenosis. Bicuspid valves are best seen on echo in diastole.

28
Reference CEACCP 12(3) CEACCP 5(1)

Similar presentations










 CPP = aortic diastolic.>")



 Assistant Professor of Medicine Medical Unit-4 LUMHS, Jamshoro.>")

 For Broker/Dealer Use Only.>")




