Download presentation
Presentation is loading. Please wait.

1
POTASSIUM BALANCE Alan C. Pao, M.D. Division of Nephrology paoman@stanford.edu Cell: 415-999-5072

2
Why devote 2 lectures to K+? Disorders of plasma K+ affect cell functions Disorders of K+ affect muscle function and nerve conduction Disorders of K+ cause death - often sudden

3
GOALS Tissue distribution of K+ Urinary excretion of K+ Clinical disorders of K+ balance and treatment

6
Diffusion of K+ out of cell sets up negative charge

9
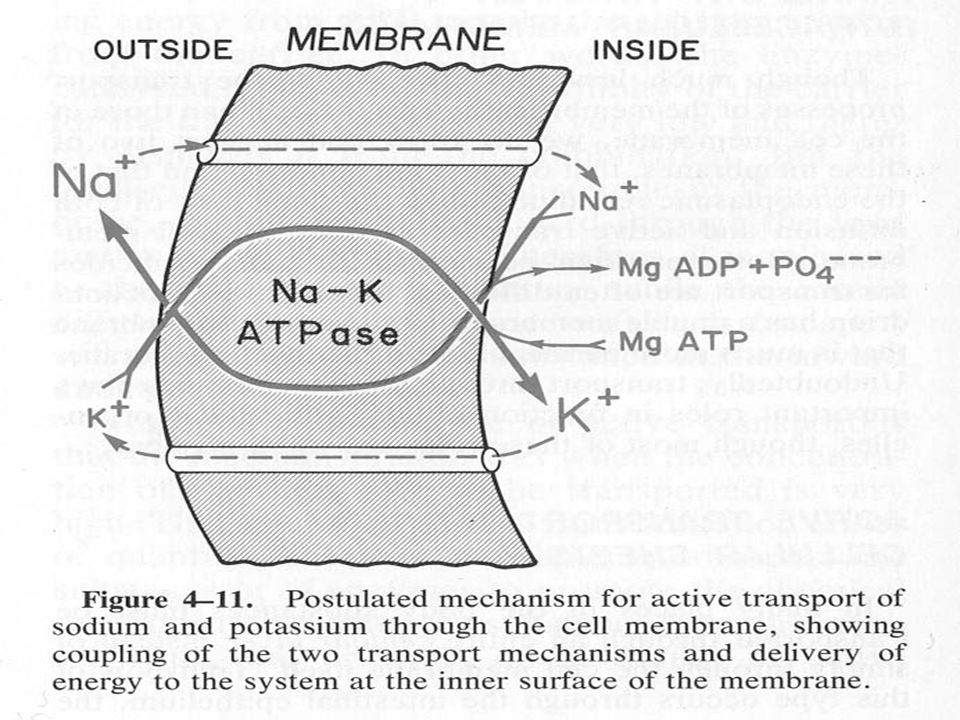
Sodium channels begin to open Na-K ATPase resets Action potential

14
GOALS Tissue distribution of K+ Urinary excretion of K+ Clinical disorders of K+ balance and treatment

16
Na/K ATPase can be stimulated Insulin Catecholamines

18
ACID BASE BALANCE Can affect the serum potassium level

20
Alkalosis shifts K in to cells Cell K+K+ H+H+ OH - added Extracellular Fluid

21
Conditions that shift K+ into cells Insulin administration Stress reaction Alkalosis

22
GOALS Tissue distribution of K+ Urinary excretion of K+ Clinical disorders of K+ balance and treatment

31
ALDOSTERONE Na+ K+ H+ HCO3- - - - - - - - - -

33
Hypokalemia- Low Plasma Potassium Hyperkalemia- High Plasma Potassium

35
HYPOKALEMIA Definition is serum K+ < than 3.5 mEq/L Decreased intake Shifting of K+ into cells Increased renal losses Increased stool losses

37
Poor oral intake of potassium Starvation Vomiting Malabsorption Clay

40
Conditions that shift K+ into cells Insulin administration Stress reaction Alkalosis

41
CASE 20 y.o. Asian male seen in ER for one day of acute onset muscle weakness –Leg > arm weakness –Thigh > calf ms weakness –Could not get out of bed and cannot walk –No muscle aches Over past 3 months: 35 pound weight loss, attributed to boxing training regimen Eats pasta frequently for training regimen

42
FH father with hyperthyroidism No PMH, No Meds No EtOH, tobacco, IVDA

43
VS T 36.4 P 91 BP 125/60 RR 18 Neuro exam a and o x 4 CN 2-12 intact Motor grip 4/5, elbow flexion/extension 4/5 Shoulder abduction/adduction 4/5 Motor dorsiflex/plantar flex 3/5 Knee extension/flex 4/5 Hip flexion/extension 3/5 Sensory grossly intact Reflexes 1+ throughout

44
Labs CSF normal CK 617 Utox neg TSH < 0.1 141 2.627 104

46
Increased stool losses Diarrhea Laxative abuse Tumors that cause K+ secretion into stool

47
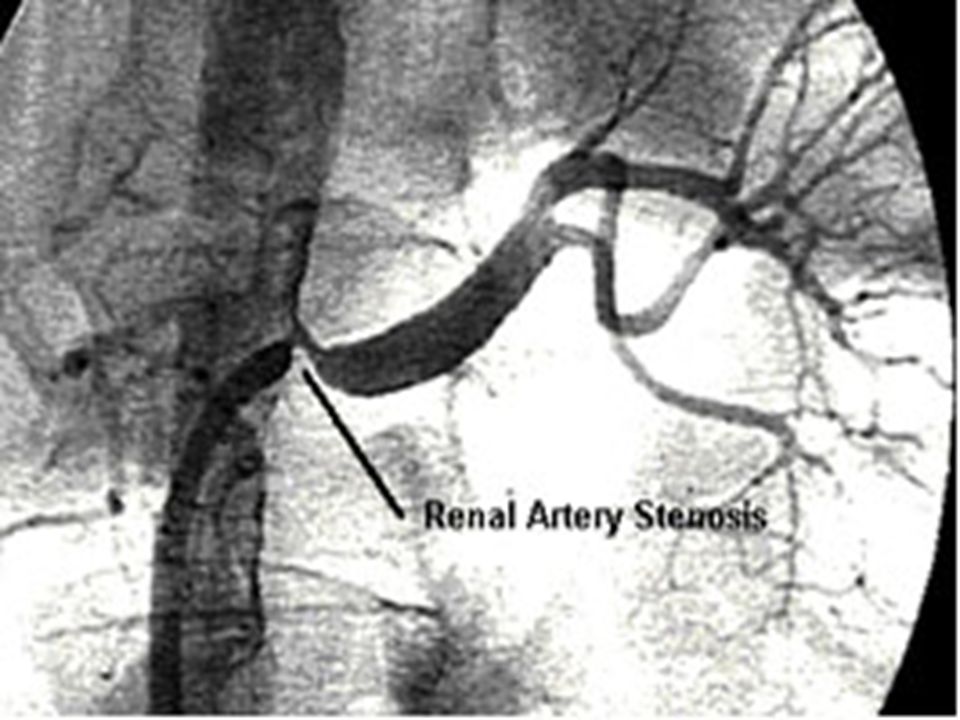
Increased Renal Losses Diuretic medications

50
ALDOSTERONE Na+ K+ H+ HCO3- - - - - - - - - -

51
Increased Renal Losses Diuretic medications Mineralocorticoid excess Amphotericin B Hypomagnesemia

52
ALDOSTERONE Na+ K+ H+ HCO3- - - - - - - - - -

53
CASE 63 year old male with severe HTN Serum potassium of 3.0

54
CASE 63 year old male with severe HTN Serum potassium of 3.0 Serum bicarbonate of 30

55
ALDOSTERONE Na+ K+ H+ HCO3- - - - - - - - - -

57
CASE 63 year old male with severe HTN Serum potassium of 3.0 Serum bicarbonate of 30 Renin level is suppressed Aldosterone level elevated

58
ALDOSTERONE Na+ K+ H+ HCO3 147 3.030 - - - - - - - - -

63
ALDOSTERONE Na+ K+ H+ HCO3 147 3.129 RENIN - - - - - - - - -

66
Treatment of Hypokalemia Find the underlying cause and treat it Stop the clay, stop the laxatives, reduce the diuretics etc. Administer K+ orally or intravenously Replace magnesium

67
HYPERKALEMIA Definition is serum K+ > than 5.3 mEq/L Increased intake Shifting of K+ out of cells Decreased renal losses

69
Increased intake of K+ Oral intake such as bananas, tomatoes K+ supplements Intravenous KCL

71
Conditions that shift K+ out of cells Insulin deficiency Adrenergic blocking medications Acidosis Cell lysis

73
Decreased urinary K+ excretion Renal failure Hypoaldosteronism Potassium sparing diuretic such as spironolactone

74
ALDOSTERONE Na+ K+ H+ HCO3-

75
132 5.1 110 21 10 1.3

83
GOALS Tissue distribution of K+ Urinary excretion of K+ Clinical disorders of K+ balance and treatment

Similar presentations






















































 Major determinant of resting membrane potential. (arrhythmia’s etc) Long term =>")






