Download presentation
Presentation is loading. Please wait.

1
Dermatopathology Dr. Amitabha Basu

3
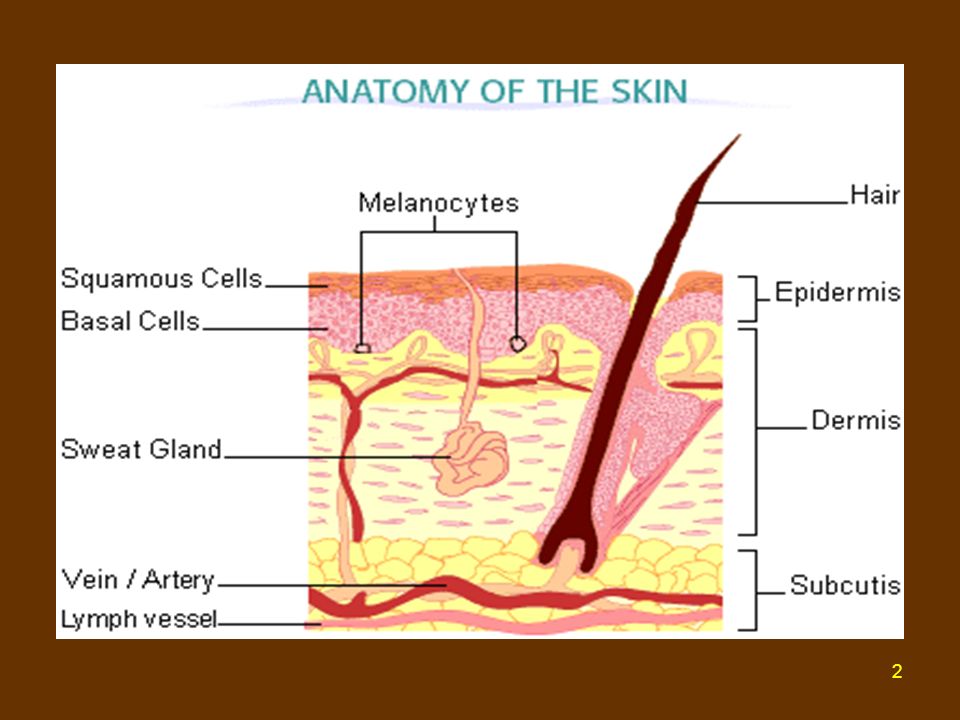
The normal histologic appearance of the skin is shown here.

4
This is normal skin from a person with a dark complexion
This is normal skin from a person with a dark complexion. The amount of skin pigmentation varies among races and individuals.

5
Here are normal adnexal structures of the skin

6
The Pilosebaceous unit.
Here are sebaceous glands, located next to a hair shaft ,forming the pilosebaceous unit.

7
Terms user in Dermatopathology
MACROSCOPIC TERMS MICROSCOPIC TERMS

8
MACROSCOPIC TERMS Macule Papule Plaque Nodule Vesicle Bulla, blister
Scale

9
Macroscopic Terms Macule: A circumscribed change in skin color without elevation or depression.

10
Papule : A solid elevated lesion usually 5 mm or less in diameter.

11
Plaque : A raised flat topped lesion that has a greater than 5 mm across.

12
Nodule: A palpable solid lesion of varying size, greater than 5 mm in diameter, which may be present in the epidermis, dermis or subcutis.

13
Vesicle: A circumscribed elevated lesion which contains free fluid
Vesicle: A circumscribed elevated lesion which contains free fluid. Vesicles are 5 mm or less in diameter.

14
Bulla ( blister ) more than 5mm across.
 more than 5mm across.")
15
Scale: Dry , horny plate like excrescence[ due to imperfect cornification].
![Scale: Dry , horny plate like excrescence[ due to imperfect cornification].](http://slideplayer.com/slide/9408928/28/images/15/Scale%3A+Dry+%2C+horny+plate+like+excrescence%5B+due+to+imperfect+cornification%5D..jpg "Scale: Dry , horny plate like excrescence[ due to imperfect cornification].")
16
MICROSCOPIC TERMS Hyperkeratosis Parakeratosis Acanthosis Dyskeratosis
Papillomatosis Spongiosis

17
Hyperkeratosis Hyperplasia of the stratum Corneum
Hyperkeratosis Hyperplasia of the stratum Corneum. Qualitative abnormality of keratin.

18
Parakeratosis Keratinization characterized by retention of the nuclei.

19
Acanthosis Epidermal hyperplasia

20
Dyskeratosis Abnormal Keratinization occurring prematurely.

21
LOSS OF INTERCELLULAR CONNECTION RESULTING IN LOSS OF COHESION.
Acantholysis LOSS OF INTERCELLULAR CONNECTION RESULTING IN LOSS OF COHESION.

22
Papillomatosis. Hyperplasia of the papillary dermis with elongation of the dermal papilla.

23
Spongiosis Intracellular edema of the epidermis.

24
Topic Benign Pigmented Lesion
Benign and Premalignant Epithelial Lesions Malignant disease of skin Acute inflammatory Dermatosis Chronic inflammatory dermatosis Bullous Disease

25
Pigment disorder Vitiligo
Depigmented multiple patches on skin.Mo melanocytes in effected area. Characterized by loss of melanocytes. It has to be differentiated from albinism. Melasma Blotch of hyperpigmented patches on face. OCP use.“ Musk of pregnancy” Freckles Light brown macule in face. Sunlight ecposure. Linear melanocytic hyperplasia.

26
Characterized by patchy loss Autoimmune
In albinism: this is melanocyte but no melanin formation Characterized by patchy loss of melanocytes. Autoimmune

27
Benign Pigmented Lesion
Nevocellular Nevus Melanocytic nevi (aka, "moles") are pigmented, benign neoplasms composed of modified melanocytes (nevus cells); they may be congenital or acquired lesions.
 are pigmented, benign neoplasms composed of modified melanocytes (nevus cells); they may be congenital or acquired lesions.")
28
These are benign nevi. Small brown flat to slightly raised nevi
These are benign nevi. Small brown flat to slightly raised nevi. They are usually less than a centimeter in diameter. IT IS A CONGENITAL LESION

29
This is a larger flat 4 cm long pigmented nevus on the upper back
This is a larger flat 4 cm long pigmented nevus on the upper back. Such larger nevi are often congenital.

30
Nevocellular Nevus Nests of small blue nevus cells.

31
Histologically : Compound and Junctional Nevus.
Compound Nevus Definition: A type of mole formed by groups of nevus cells found in the epidermis and dermis . Junctional Nevus. Definition: A mole found in the junction (border) between the epidermis and dermis layers of the skin.
 between the epidermis and dermis layers of the skin.")
32
Compound Nevus

33
Junctional Nevus.

34
Congenital nevus A nevus present at birth, may be pre-malignant depending on the size of the lesion .

35
Blue nevus Raised, bluish lesion on his upper back.

36
Blue nevus : contain spindle cells

37
Potential precursor to malignant melanoma often more than 5 mm across.
Dysplastic Nevus Potential precursor to malignant melanoma often more than 5 mm across.

38
Dysplastic Nevus Tendency to occur in sun exposed as well as non-sun exposed body surfaces. Dysplastic nevi generally develop in early adolescence or adulthood, and are present in large numbers. Can occur in multiple members of the family and prone to develop melanoma. [ Heritable Melanoma Syndrome]

39
Benign and Premalignant Epithelial Lesions.
SEBORIC KERATOSIS KERATOACANTHOMA ACTINIC KERATOSIS

40
SEBORIC KERATOSIS : usually a benign and indolent neoplasm.
If occur suddenly and Multiple in number you should suspect an internal malignancy [Paraneoplastic Syndrome]

41
SK's are common over the face, neck, and upper trunk
SK's are common over the face, neck, and upper trunk. They are raised, rough-surfaced and brown coin-like plaques.

42
Broad bands of normal-appearing epidermal cells have large keratin-filled "horn cysts" within them.

43
Neoplasm that mimics Well Differentiated Squamous Cell Carcinoma
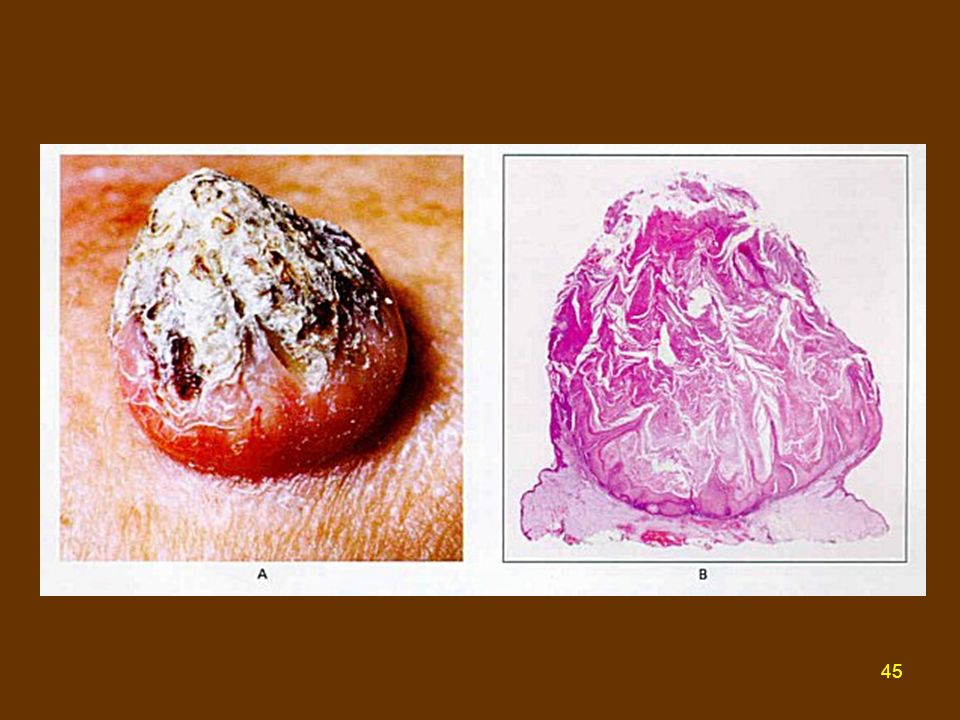
KERATOACANTHOMA Flesh Coloured dome shaped nodule , with a central keratin filled plug. Site: check, ear, nose. Neoplasm that mimics Well Differentiated Squamous Cell Carcinoma

44
Keratoacanthoma: Neoplasm that mimics Well Differentiated Squamous Cell Carcinoma: heals spontaneously

46
Less than 1 cm in diameter and sandpaper like consistency.
ACTINIC KERATOSIS Less than 1 cm in diameter and sandpaper like consistency. It a dysplastic change and damage in the skin following Chronic Sun Exposure. Seen in Sun Exposed areas.

47
A premalignant Condition.
Actinic Keratosis A premalignant Condition.

48
Actinic Keratosis Hyperkeratosis (increased amount of keratin)
Parakeratosis (presence of cell nuclei in the keratin layer, this is a sign of decreased turnover time of the epidermis) Dysplasia (abnormal maturation of the epidermis; the cells have atypical morphology cytologically) Solar elastosis (in which the dermis is stained blue rather than pink resembling the elastic tissue; this is a sign of sun damage)
 Dysplasia (abnormal maturation of the epidermis; the cells have atypical morphology cytologically) Solar elastosis (in which the dermis is stained blue rather than pink resembling the elastic tissue; this is a sign of sun damage)")
49
Biopsy of the skin showing Solar Elastosis [ pale blue colored area, beneath the epidermis]
![Biopsy of the skin showing Solar Elastosis [ pale blue colored area, beneath the epidermis]](http://slideplayer.com/slide/9408928/28/images/49/Biopsy+of+the+skin+showing+Solar+Elastosis+%5B+pale+blue+colored+area%2C+beneath+the+epidermis%5D.jpg "Biopsy of the skin showing Solar Elastosis [ pale blue colored area, beneath the epidermis]")
50
Major factor : Ultraviolet ray B
Lesions due to Sun exposure : Malignancy Malignant melanoma Squamous Cell Carcinoma Basal Cell carcinoma Major factor : Ultraviolet ray B

51
Malignant Melanoma Skin, Oral, anogenital, esophagus, meninges.
Metastasis: Regional Lynph node, lung, liver , brain. It can occur even after the surgical removal of the tumor.

52
Malignant Melanoma Warning signs are A,B,C,D,E's of a Pigmented lesion. Asymmetry, Irregular Border, Variegated Color, larger than 5mm Diameter, Elevation.

53
Compare a benign nevus and a melanoma ( right).
.")
54
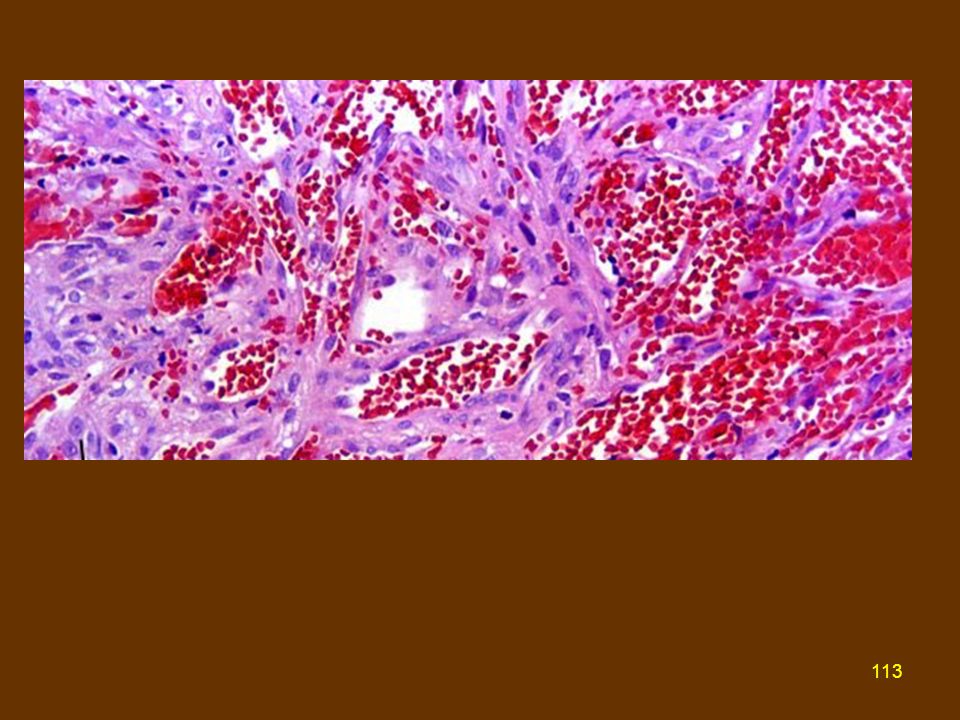
This is the microscopic appearance of a malignant melanoma.

55
Description Large polygonal cells (or spindle cells in some cases) have very pleomorphic nuclei which contain prominent nucleoli. The neoplasm is making brown melanin pigment.

57
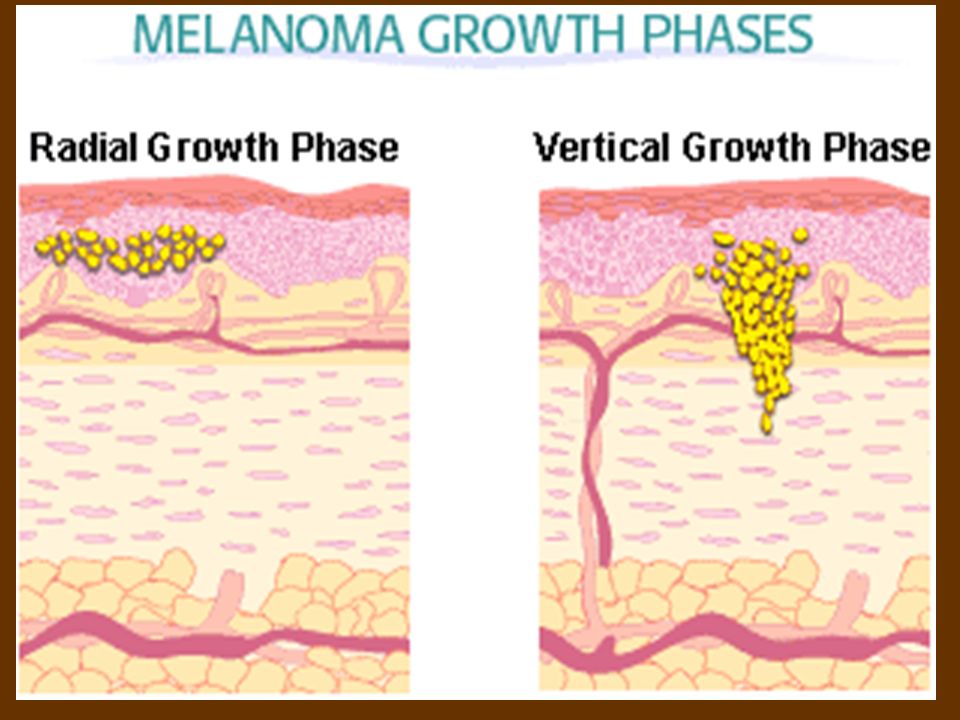
Vertical Growth Phase. There is a worse prognosis because the dermal invasion is apt to be deep at the time of initial presentation of the patient - resulting in an increased risk of metastases.

58
The neoplastic cells shown here stain positively with HMB-45, suggesting that the primary neoplasm is a melanoma.

59
Squamous cell Carcinoma

60
Risk Factor for SCCA Besides sun exposure, risk factors for squamous cell carcinoma arising in skin include carcinogens such as Tars, Chronic ulcers, Burn scars, Arsenic poisoning, and Radiation exposure. XERODERMA PIGMENTOSA

61
SCCA : It actually arose in a draining sinus tract from chronic osteomyelitis of the humerus.

62
The neoplastic cells extend downward into the dermis.

63
Basal cell Carcinoma Occur in case of immunodeficiency
Xeroderma Pigmentosa [ Defect in DNA repair ]

64
Pearly lesion and telangiectasia in the surface in BCC

65
Rodent Ulcer-Ulcerated BCC

66
BCCA These rarely metastasize, but are slow-growing and progressive over time. Early detection and excision is a must. A BCC can grow quite large and invade surrounding tissues, but it virtually never metastasizes.

67
The cells of a basal cell carcinoma are dark blue and oblong with scant cytoplasm: Mimic cells of basal layer.

68
The typical nest has a palisaded arrangement of cells around the periphery.

69
Basal Cell Carcinoma( Biological Behavior)
These neoplasms can be multifocal. Metastases are quite rare. SO, PROGNOSIS IS GOOD.

70
MOLECULAR GENETIC OF SKIN CANCER
Nevoid basal cell carcinoma syndrome PTCH/PTCH gene DNA repair defect Multiple BCCA Autosomal dominant Cowden syndrome PTEN, MMAC1 Tumor of skin appendage and adenocarcinoma Xeroderma Pigmentosa XPA/XPA gene Skin cancer (SCCA, BCCA)
")
71
MOLECULAR GENETIC OF SKIN CANCER
SCCA Sporadic: No inheritances, DNA damage and Immunosuppression by sunlight. Mutation of p53 in actinic Keratosis induced SCCA is noted. Melanoma Occur in familiar setting(10-15%), In dysplastic nevus syndrome-it is associated with deletion of p16INK4A gene. p16INK4A =Cyclin-dependent kinase inhibitor 2
, In dysplastic nevus syndrome-it is associated with deletion of p16INK4A gene. p16INK4A =Cyclin-dependent kinase inhibitor 2.")
72
Acute inflammatory Dermatosis
Urticaria (hives) Acute Eczematous Dermatitis
 Acute Eczematous Dermatitis.")
73
Urticaria (hives) Caused due to Local mast cell Degranulation.
Occur in the areas exposed to the pressure, trunk, distal extremities, ears. This lesion will fade normally if no such exposure occur further

74
What are responsible antigens ?
Pollen Food Drugs(opiates) Insect venom Drug rash due to Cephalosporin
 Insect venom. Drug rash due to Cephalosporin.")
75
Acute Eczematous Dermatitis
Papulovesicular , oozing and crusted lesion Contact reaction to poison ivy, laundry detergent.

76
This is contact dermatitis, a form of type IV hypersensitivity reaction that is localized.
Other forms: Atopic and Drug (penicillin) related dermatitis.
 related dermatitis.")
77
Histology: Dermatitis
Spongiosis (edema) of epidermis.
 of epidermis.")
78
Erythema Multiforme The classic "target" lesion has a central vesicle surrounded by a zone of erythema.

79
Erythema Multiforme These lesions are "multiform" because macules, papules, vesicles, and bullae may be seen grossly. Sites : Lip, oral cavity, conjunctiva, urethra, anogenital Region.

80
Erythema Multiforme Etiology: A hypersensitivity reaction to
Infection, Drugs, Neoplasia, or Collagen vascular diseases.

81
Erythema Multiforme Infection: Mycoplasma, leprosy, Typhoid
Drug: sulphonamide, barbiturate, salicylates Malignancy: Carcinoma and lymphoma Collagen disorder: Lupus erythematous.

82
Chronic inflammatory dermatosis
Psoriasis Lichen Planus

83
Lichen Planus : p3 Pruritic, purple, polygonal papules.
White lines: Wickham Striae

84
Civatte Body in Lichen Planus and sawtoothing of epidermis
It is an anucleated necrotic Basal cells.

85
Psoriasis

86
Psoriasis : It is a common Inflammatory Dermatosis.
This is psoriasis. The thick, silvery, scaling lesions are most often found over bony prominences, scalp, genitalia, and hands.

87
Psoriasis It occurs when there is abnormal proliferation of epithelial cells. Sensitize T cell mediated tissue damage. It will bleed if you scraped off this!- auspitz sign.

88
Nail Change : Onycholysis
The scalp, elbows, and knees are the most common sites for psoriasis

89
Psoriasis Psoriasis is an autoimmune disease.
Genetic and immune factors involved.

90
Munro microabscess Munro microabscess. Important microscopic features.

91
Bullous Disease Secondary phenomenon of infections , dermatitis.
Bulla ( blister ) more than 5mm across.
 more than 5mm across.")
92
Subcorneal Bulla

93
Supra basal Bulla

94
Subepidermal Bulla

95
Pemphigus Rare autoimmune blistering disorder
( Type II hypersensitivity reaction) Age : middle age Sex : Women : Men :: 1:1 Cause of Bulla formation : Acantholysis. Type of Bulla: Supra basal Bulla.
 Age : middle age. Sex : Women : Men :: 1:1. Cause of Bulla formation : Acantholysis. Type of Bulla: Supra basal Bulla.")
96
Site: Scalp, face, axilla and also in the point of pressure.
Pemphigus Pemphigus vulgaris [ most common] Site: Scalp, face, axilla and also in the point of pressure.

97
Pemphigus vulgaris [ bulla rupture easily and will be covered by dried serum and crust.]
![Pemphigus vulgaris [ bulla rupture easily and will be covered by dried serum and crust.]](http://slideplayer.com/slide/9408928/28/images/97/Pemphigus+vulgaris+%5B+bulla+rupture+easily+and+will+be+covered+by+dried+serum+and+crust.%5D.jpg "Pemphigus vulgaris [ bulla rupture easily and will be covered by dried serum and crust.]")
98
Pemphigus vulgaris [ Suparabasal bulla ]
![Pemphigus vulgaris [ Suparabasal bulla ]](http://slideplayer.com/slide/9408928/28/images/98/Pemphigus+vulgaris+%5B+Suparabasal+bulla+%5D.jpg "Pemphigus vulgaris [ Suparabasal bulla ]")
99
Deposition of IgG and Complement along the cell membrane, giving a Fish Net appearance.

100
Pemphigus vulgaris Sera of the patient contains IgG antibody to desmogleins [ intercellular cement substance] .
![Pemphigus vulgaris Sera of the patient contains IgG antibody to desmogleins [ intercellular cement substance] .](http://slideplayer.com/slide/9408928/28/images/100/Pemphigus+vulgaris+Sera+of+the+patient+contains+IgG+antibody+to+desmogleins+%5B+intercellular+cement+substance%5D+..jpg "Pemphigus vulgaris Sera of the patient contains IgG antibody to desmogleins [ intercellular cement substance] .")
101
Bullous pemphigoid. Seen in adult Do not rupture easily unlike pemphigus Heal without scarring. The target antigen is hemidesmosome. Autoantibody produces against this protein.

102
There is a large, tense bulla at the center and a small bulla at the left.

103
Sites : Inner aspect of thigh, forearm axilla, groin and Mucosa

104
Bullous pemphigoid : Subepidermal Bulla

105
IgG and complement staining pattern in Bullous pemphigoid
IgG and complement staining pattern in Bullous pemphigoid. [ Linear Deposit ]

106
Dermatitis herpetiformis
Urticaria and grouped (herpetiform vesicles.

107
Site; extensor surface elbow, knees upper back.

108
Dermatitis herpetiformis : Subepidermal Blisters
It can occur in association to intestinal celiac disease and respond to a gluten free diet.

109
The inflammatory cells within the vesicle are PMN's
The inflammatory cells within the vesicle are PMN's. Slight basophilia is seen in the partly necrotic dermal papilla.

110
IgA granular basement membrane zone with stippling in dermal papillae (40x)
")
111
Kaposi's sarcoma Late Lesion Early lesion

112
The lesions can start as small reddish to red-purple plaques or patches. Over time, the lesions become nodular and larger and more numerous. If the HIV test is positive, then KS is diagnostic of AIDS

114
End of Dermatopathology
Thank You .

Similar presentations







 Pathogenesis` (Mechanisms:inflammation) Clinical Features (Signs and Symptoms) Fever,>")





>")





