Download presentation
Presentation is loading. Please wait.

2
Anatomy. Examination method. Congenital & developmental anomalies. Retinal inflammation. Vascular disorder. Age-related macular degeneration. Retinal detachment. Retinal dystrophies. Retinal tumor.

3
Anatomy The retina is transparent light sensitive membrane, lines inside of the eye ball behind the orra serrata which is the anterior termination of retina. The retina divided into :- 1- inner neurosensory layer. 2- outer retinal pigment epithelium.

4
Retina firmly adherent to vitreous base, separated from the vitreous by inner limiting membrane. Bruch’s membrane separate chorio- capillaries from retina pigment epithelium

5
Layers of retina 1- Inner limiting membrane. 2- Layer of optic nerve fibers. 3- Layer of ganglion cells. 4- Inner plexiform layer. 5- Inner nuclear layer. 6- Outer plexiform layer. 7- Outer nuclear layer. 8- Outer limiting membrane. 9- Layer of rods and cones. 10-Retinal pigment epithelium. 11-Bruch’s membrane.

6
Macula lutea Yellow spot in posterior pole of the retina. It has a diameter 5.5 mm. The horizontal diameter is slightly greater than vertical. The center of the macula is marked by depression called fovea centralis.

7
Macula is approximately 2 disc diameter away from the temporal margin of optic disc and about 1mm below the horizontal meridian. The fovea centeralis is a highly differentiated spot, here only cones are present and the other layers of retina are almost absent. It is the most sensitive part of the retina and has the maximal visual acuity.

8
Blood supply of retina The inner layers of retina are supplied by the central retinal artery and its branches. These arteries are end arteries and the outer layers of retina up to outer nuclear layer get their nourishment by diffusion from chorio-capillaries.

9
The venous drainage of the inner layers of retina is through the retinal veins, the outer layers are drained by vortex veins. Pulsation in the retinal vein is normal; pulsation in retinal arteries is abnormal The neurosensory retina has no sensory supply.

10
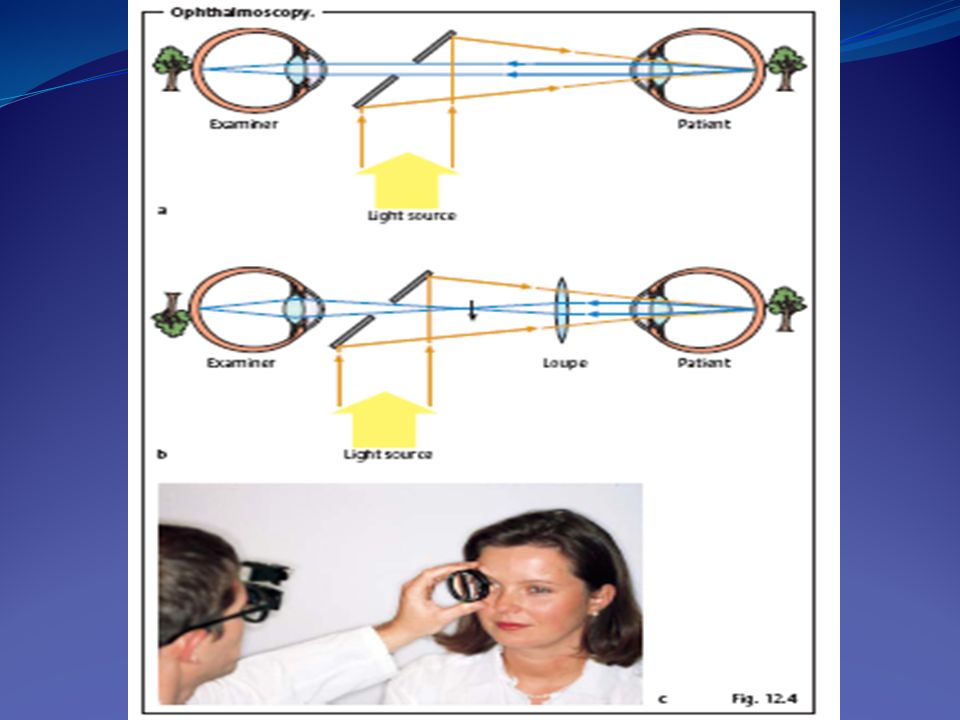
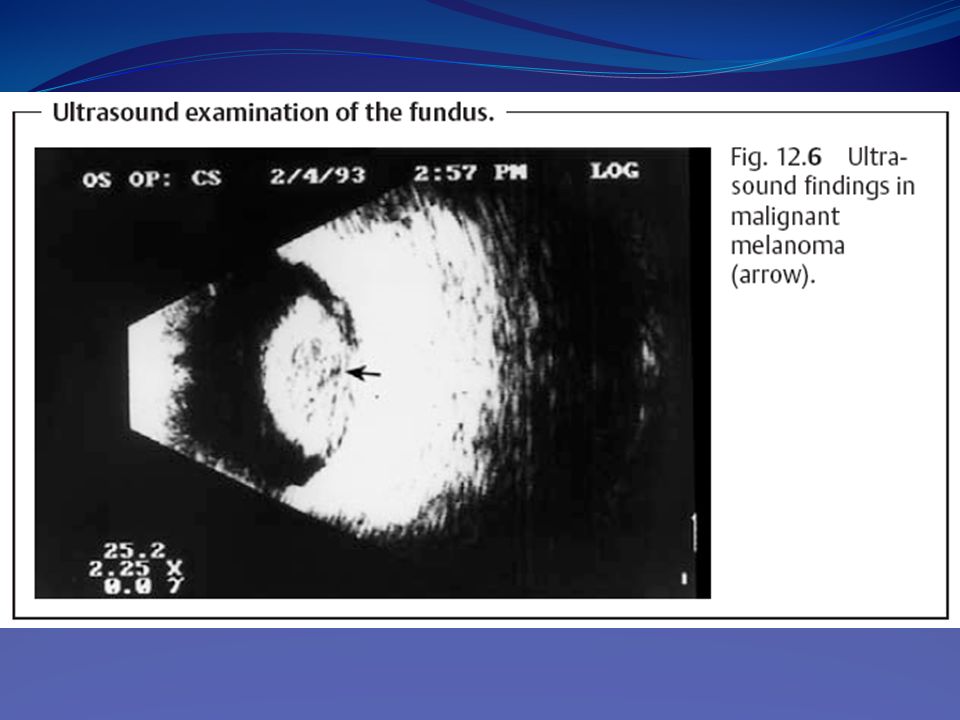
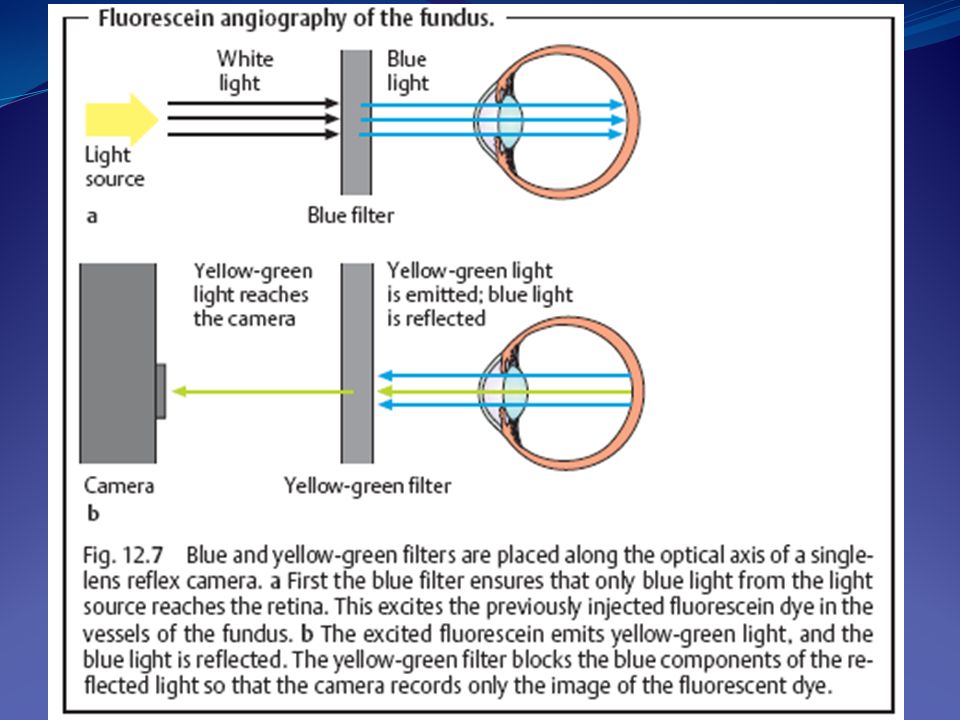
Method of examination A. Visual acuity. B. Examination of the fundus 1- Direct ophthalmoscopy. 2- Indirect ophthalmoscopy. 3- Contact lens examination 4- ultrasonogaphy. 5- Fundus photography. 6- Fluorescein angiography.

16
C. Color vision Color vision defect may be congenital (especially in men as they are inherited as X-linked recessive) or acquired for example macular diseases
 or acquired for example macular diseases.")
17
D. Electrophysiologic examination method 1. Elctroretinagram (ERG): to record the electrical response of the retina to flashes of light as in retinitis pigmentosa. 2. Electrooculogram (EOG): to detect abnormal changes in RPE such as macular dystrophy. 3- Visual effort potential (VEP): to diagnose damage along visual pathway.
: to record the electrical response of the retina to flashes of light as in retinitis pigmentosa. 2. Electrooculogram (EOG): to detect abnormal changes in RPE such as macular dystrophy. 3- Visual effort potential (VEP): to diagnose damage along visual pathway..")
18
Congenital & Development anomalies of the retina 1- Coloboma of the retina : A typical coloboma of retina associated with coloboma of the choroid,is situated downward & inwards. The retina fails to develop in the region due to the non-closure of the optic fissure.

19
2- Medullated nerve fibers (opaque nerve fibers): The myelination of the optic nerve progresses from brain toward the periphery and stop at the lamina cribrosa. It is usually completed shortly after birth.

20
3- Congenital pigmentation of the retina : It is not rare to see small oval, black polygonal spot, in the retina lying below venules.

21
Inflammation of the retina Inflammation of retina is called retinitis. It is often secondary to inflammation of choroid (chorio-retinitis). Primary inflammation it is uncommon and it is either : a. Acute purulent retinitis occur due to the infection of retina by pyogenic organism. b. Subacute infective retinitis or septic retinitis of Roth.
. Primary inflammation it is uncommon and it is either : a. Acute purulent retinitis occur due to the infection of retina by pyogenic organism. b. Subacute infective retinitis or septic retinitis of Roth..")
23
c. Chronic granulomatous inflammation of the retina usually secondary to chorioditis, e.g : Toxoplasmosis : common cause of chorio- rtenitis most of the condition congenital due infection during pregnancy, but some of causes are acquired. Causative agent toxoplasmosis gondi. Congenital associated with anterior & posterior uveitis and retinitis. Diagnosis done by ELISA test.

25
Toxocara infection Caused by toxocara canis from dogs. Usually in children and we get granuloma in macula or in periphery of retina. Rubella infection Is the commonest type of infection that occur in children, the infection occur in the first trimester, causing rubella syndrome (microopthalmia, cataract, glaucoma and retinal pigmented layer destruction in the form of salt and pepper appearance).
..")
27
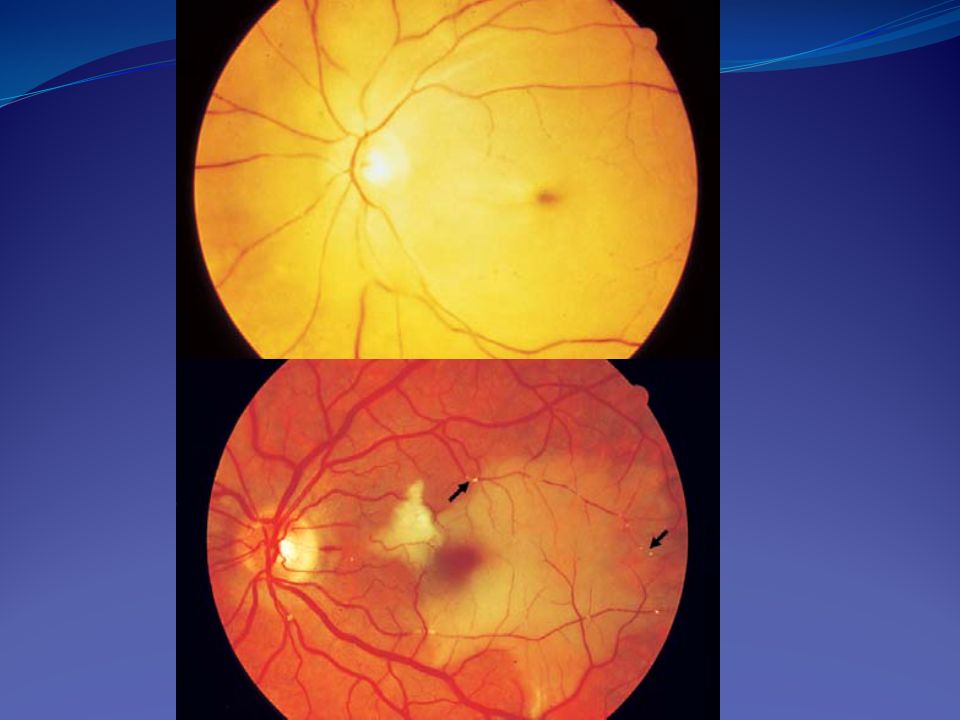
Vascular disorder Central retinal vein occlusion : The main symptom is painless sudden loss of vision ; therefore the patient should be sent for medical assessment of hypertension, DM & polycythemia.

28
Fundus examination It is a mandatory, the optic disc which is swollen, congested blood vessel, engorged veins and they are tortuous, a lot of retinal micro-infarct and hemorrhage. The disc is surrounded by cotton-wool spot usually in the macula lesion. One of the local cause is glaucoma and should be excluded and sent the patient to physician.

30
The CRVO can be divided into ischemic and non-ischemic form. The ischemic form characterized by developing of a lot of capillaries and carries high risk of developing neovascular glaucoma i.e 100 days glaucoma.

31
Treatment By observing the patient and once the ischemia changes develop Laser photo-coagulation done, not to preserve vision but to stop development of neovascular glaucoma (blind painful eye).
.")
32
Complication. Preretinal neovascularization.. Retinal detachment.. Rubeosis iridis with angle closure glaucoma. Prognosis. One third of all patients improved.. One third remain unchanged.. One third become worsen.

33
Central retinal artery occlusion It is much less common, the symptoms are sudden painful or painless loss of the vision, usually secondary to temporal arteritis or giant cell arteritis. Pain in the CRAO usually occur in patients above 55 – 60 year old and once occurred we should exclude giant cell arteritis.

34
The diagnostic feature of the condition is that the ESR is high (over 100 mm/h). If the condition is not diagnosed and treated early, the other eye will involved and leading to total blindness.

35
On examination the vision is reduced and also light perception reduced or some time we see ill-sustained pupillary reaction (Marcus-Gunn pupil). Fundus examination - Cherry red spot at the fovea. - Optic disc swollen and pale. - Attenuated retinal blood vessels (like very thin threat indicate occlusion. - Cotton-wool spot.

37
Causes of CRAO 1- Giant cell arteritis. 2- Cardiac valvular lesion. 3- Carotid artery diseases. 4- Systemic vascular diseases as hypertension. 5- Sickle cell anemia. 6- DM. painless.

38
Diagnosis 1- Thorough examination and investigation. 2- Doppler for carotid. 3- Carotid angiography. 4- valvular study.

39
Treatment If we catch the condition early within 4-6 h. we may save the eye by : 1- intensive digital massage to lower IOP. 2- I.V. acetazolamide. 3- paracentesis of the eye from anterior chamber to lower IOP suddenly and causing some perfusion to optic disc region, this procedure done under local anesthesia 4- use of anticoagulant as aspirin.

40
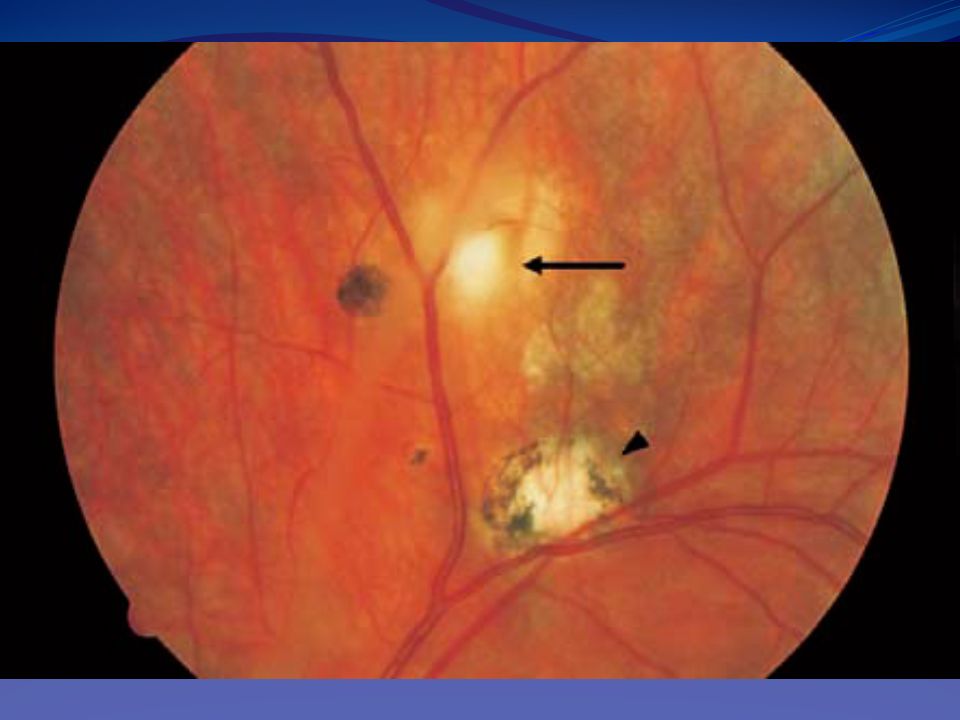
Age-related macular degeneration. It is the leading cause of blindness in the western world. It affect people above 60 year and therefore also known as senile macular degeneration. It is start with one eye then extend to involve the other eye, so it is bilateral but not equal, it will lead to loss of central vision but not involve the peripheral, the patient retaining navigational vision.

41
Classification 1. Dry type: area of sharply circumscribed retinal atrophy, the lesion flat and not elevated. FAG dose not reveal any leakage of dye. 2. Wet (exudative) type: circumscribed dome shaped area of elevation of retina, sometime areas of hemorrhage and exudate. FAG shows leakage of the dye due to subretinal neovascular membrane.
 type: circumscribed dome shaped area of elevation of retina, sometime areas of hemorrhage and exudate. FAG shows leakage of the dye due to subretinal neovascular membrane..")
Similar presentations







 Waxman MD PhD>")


 pigment.>")






 occludes a branch of the central retinal vein Blockage causes bleeding from that branch Concerned about neovascularization.>")





>")

