Download presentation
Presentation is loading. Please wait.

2
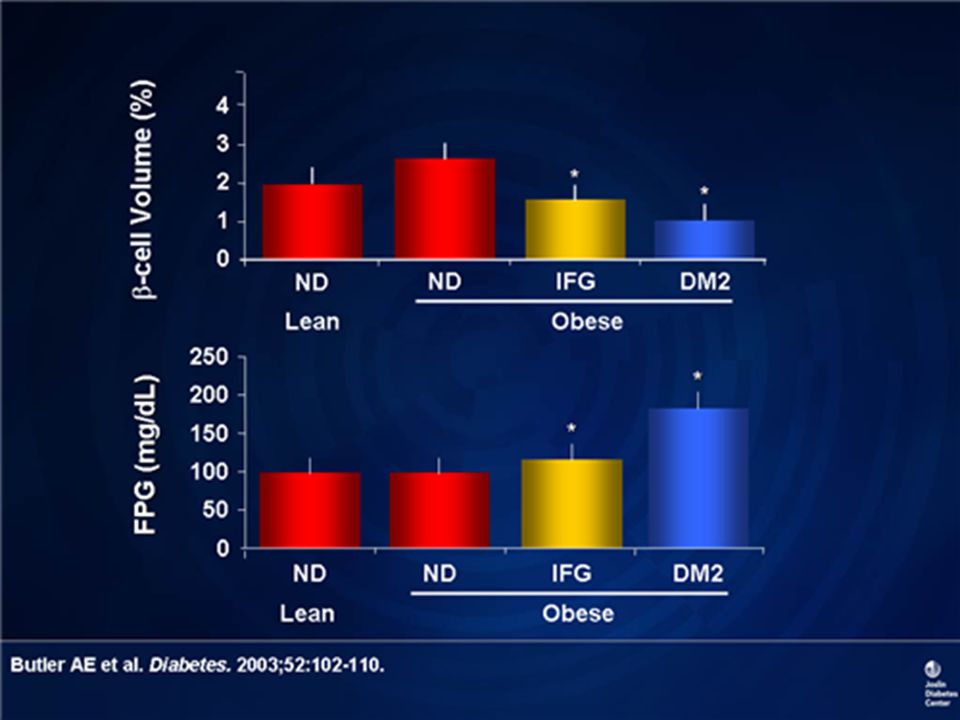
DM2

3
Criteria for the Diagnosis of Diabetes A1C ≥6.5% OR Fasting plasma glucose (FPG) ≥126 mg/dl (7.0 mmol/l) OR Two-hour plasma glucose ≥200 mg/dl (11.1 mmol/l) during an OGTT OR A random plasma glucose ≥200 mg/dl (11.1 mmol/l) ADA. I. Classification and Diagnosis. Diabetes Care 2011;34(suppl 1):S13. Table 2.
:S13. Table 2..")
9
Components of the Comprehensive Diabetes Evaluation: ADA. V. Diabetes Care. Diabetes Care 2011;34(suppl 1):S17. Table 8. Physical examination (1) Height, weight, BMI Blood pressure determination, including orthostatic measurements when indicated Fundoscopic examination* Thyroid palpation Skin examination (for acanthosis nigricans and insulin injection sites) *See appropriate referrals for these categories.
:S17. Table 8. Physical examination (1) Height, weight, BMI Blood pressure determination, including orthostatic measurements when indicated Fundoscopic examination* Thyroid palpation Skin examination (for acanthosis nigricans and insulin injection sites) *See appropriate referrals for these categories..")
10
Components of the Comprehensive Diabetes Evaluation: ADA. V. Diabetes Care. Diabetes Care 2011;34(suppl 1):S17. Table 8. *See appropriate referrals for these categories. Physical examination : Comprehensive foot examination – Inspection – Palpation of dorsalis pedis and posterior tibial pulses – Presence/absence of patellar and Achilles reflexes – Determination of proprioception, vibration, and monofilament sensation
:S17. Table 8. *See appropriate referrals for these categories. Physical examination : Comprehensive foot examination – Inspection – Palpation of dorsalis pedis and posterior tibial pulses – Presence/absence of patellar and Achilles reflexes – Determination of proprioception, vibration, and monofilament sensation.")
11
Initial Metabolic Evaluation Referrales

12
Laboratory evaluation: A1C, if results not available within past 2–3 months If not performed/available within past year – Fasting lipid profile, including total, LDL- and HDL-cholesterol and triglycerides – Liver function tests – Test for urine albumin excretion with spot urine albumin/creatinine ratio – Serum creatinine and calculated GFR – TSH in type 1 diabetes, dyslipidemia, or women >50 years of age ADA. V. Diabetes Care. Diabetes Care 2011;34(suppl 1):S17. Table 8.
:S17. Table 8..")
13
Referrals: Annual dilated eye exam Family planning for women of reproductive age Registered dietitian for MNT Diabetes self-management education Dental examination Mental health professional, if needed ADA. V. Diabetes Care. Diabetes Care 2011;34(suppl 1):S17. Table 8.
:S17. Table 8..")
19
Correlation of A1C with Estimated Average Glucose (eAG) Mean plasma glucose A1C (%)mg/dlmmol/l 61267.0 71548.6 818310.2 921211.8 1024013.4 1126914.9 1229816.5 These estimates are based on ADAG data of ~2,700 glucose measurements over 3 months per A1C measurement in 507 adults with type 1, type 2, and no diabetes. The correlation between A1C and average glucose was 0.92. A calculator for converting A1C results into estimated average glucose (eAG), in either mg/dl or mmol/l, is available at http://professional.diabetes.org/GlucoseCalculator.aspx.
, in either mg/dl or mmol/l, is available at")
20
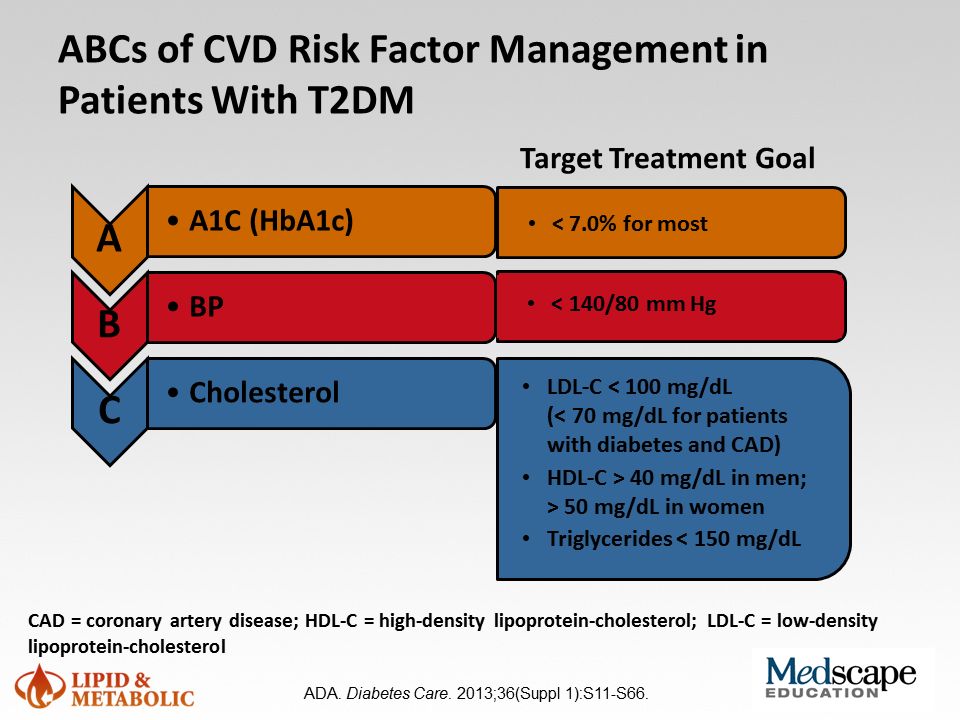
Outpatient Management: Bp control Lipid management Cigar discontinuous Glycemic control

23
PREDIABETES PREDIABETES

24
FPG 100-125 mg/dl (5.6-6.9 mmol/l): IFG or 2-h plasma glucose in the 75-g OGTT 140-199 mg/dl (7.8-11.0 mmol/l): IGT or A1C 5.7-6.4% Prediabetes: IFG, IGT, Increased A1C *For all three tests, risk is continuous, extending below the lower limit of a range and becoming disproportionately greater at higher ends of the range. ADA. I. Classification and Diagnosis. Diabetes Care 2011;34(suppl 1):S13. Table 3.
:S13. Table 3..")
25
The natural history of both IFG and IGT is variable, with 25% progressing to diabetes, 50% remaining in their abnormal glycemic state, and 25% reverting to NGT over an observational period of 3 – 5 years.

26
The Australian Diabetes, Obesity, and Lifestyle Study (AusDiab) These findings suggest that strategies to prevent premature mortality, particularly CVD death, need to be targeted not only to people with diabetes mellitus but also toward people with milder forms of abnormal glucose metabolism.
 These findings suggest that strategies to prevent premature mortality, particularly CVD death, need to be targeted not only to people with diabetes mellitus but also toward people with milder forms of abnormal glucose metabolism.")
27
AACE Guidelines for Prediabetes Management : The management of prediabetes involves intensive lifestyle management and setting treatment goals of blood pressure and lipid level control matching those for diabetes, according to a consensus statement.

28
The first goal is aggressive lifestyle management to prevent the progression to type 2 diabetes.

29
Two randomized controlled trials of individuals with IGT found that lifestyle intervention studies reduce the risk of progressing to diabetes by 58%.

30
Diet should be low in total fat, saturated fat, and trans-fatty acids and should include adequate dietary fiber. For blood pressure control, lower sodium intake and avoidance of excess alcohol are recommended.

31
All patients with prediabetes should have intensive lifestyle management, which is safe and effective in improving glycemia and in decreasing cardiovascular risk. Treatment goals for blood pressure and lipid control should match those for diabetes.

32
Recommended Lifestyle Changes Daily calories Fat: < 25 to 30 percent Saturated fat: < 10 percent Carbohydrates: 50 to 60 percent Protein: 15 to 20 percent Daily fiber intake: > 15 g for every 1,000 calories consumed Foods: salad, vegetables,fruits, whole grains fish high in omega-3 fatty acids, legumes, lean meat; minimal intake of refined sugars Exercise*: moderate-intensity physical activity, such as brisk walking or biking, for 150 minutes per week Weight loss goal*: 5 to 7 percent of body weight1 Counseling by professionals on weight reduction

33
Individuals with prediabetes should lose 5% to 10% of body weight and maintain it long term. Regular, moderate-intensity physical activity is recommended for 30 to 60 minutes daily at least 5 days weekly.

34
societal change : We need to build our communities and cities in a way that encourages people to walk and to be more physically active. We need to build our communities and cities in a way that encourages people to walk and to be more physically active.

35
For persons with prediabetes at particularly high risk, pharmacologic glycemic treatment may be considered in addition to lifestyle strategies.

36
Metformin and acarbose are safe and effective in helping prevent diabetes. Although thiazolidinediones decrease the risk for progression from prediabetes to diabetes, safety concerns include congestive heart failure or fractures.

37
The oral hypoglycaemic drugs metformin and acarbose have also been shown to be effective, but less so than the life style measures.

38
individuals with IFG/IGT are treated with metformin, the Panel recommends that routine monitoring should be performed with A1C testing semi-annually. If not on drug therapy, the patient should be seen annually.

39
the Panel recommends that only metformin be considered as drug therapy for individuals with IFG/IGT. In the DPP, the subsets of the study cohort that had substantially increased benefit from metformin were those participants 35 kg/m2.

40
Since individuals with associated risk factors for diabetes, e.g., family history in first- degree relatives, elevated triglycerides, low HDL cholesterol, and hypertension, are more likely to progress to diabetes, the presence of one or more of these factors may contribute to the decision to treat with metformin.

41
Metformin and acarbose are safe and have strong evidence for a reduction in the development of diabetes from prediabetes. Thiazolidinediones also reduce the risk for progression from prediabetes to diabetes, but there are safety concerns including congestive heart failure or fractures.

42
Treating prediabetes with metformin: CONCLUSION Metformin decreases the rate of conversion from prediabetes to diabetes. This was true at higher dosage (850 mg twice daily) and lower dosage (250 mg twice or 3 times daily); in people of varied ethnicity; and even when a sensitivity analysis was applied to the data.
 and lower dosage (250 mg twice or 3 times daily); in people of varied ethnicity; and even when a sensitivity analysis was applied to the data..")
43
Patients with prediabetes should have the same target blood pressure as do persons with diabetes (systolic < 140 mg Hg; diastolic 80 mm Hg). Angiotensin-converting enzyme inhibitors or angiotensin receptor blockers are recommended as first-line agents and calcium channel blockers as second-line treatment of hypertension.

44
Thiazides and/or β-blockers should be used with caution because of adverse effects on glycemia.

45
Lipid level goals for persons with prediabetes should be the same as for those with established diabetes. Statins are recommended if needed to achieve treatment goals for low-density lipoprotein cholesterol levels (100 mg/dL), nonhigh-density lipoprotein cholesterol levels (130 mg/dL), and apolipoprotein B (90 mg/dL).
, nonhigh-density lipoprotein cholesterol levels (130 mg/dL), and apolipoprotein B (90 mg/dL)..")
46
How should prediabetes and its treatment be monitored? Monitoring for patients with prediabetes should include an annual glucose tolerance test and twice-yearly testing for microalbuminuria and fasting plasma glucose, hemoglobin A1C, and lipid levels. Highest-risk patients should be monitored more often.

47
Get serious FPG >99 mg/dl

Similar presentations











 describes relative weight for height: weight (kg)/height (m 2 ) Overweight = 25–29.9 BMI Obesity = >30 BMI.>")












![LIFESTYLE MODIFICATIONS FOR PREVENTING HEART DISEASE [e.g. HEART ATTACKS] [ primary prevention of coronary artery disease ] DR S. SAHAI MD [Med.], DM [Card]](/19/5810187/big_thumb.jpg "LIFESTYLE MODIFICATIONS FOR PREVENTING HEART DISEASE [e.g. HEART ATTACKS] [ primary prevention of coronary artery disease ] DR S. SAHAI MD [Med.], DM [Card]>")



 2.>")