Download presentation
Presentation is loading. Please wait.

1
در مرکز پزشکی هسته ای دکتر دباغ – دکتر صادقی در خدمت شما هستیم مشهد، ملاصدرا 11 ، پلاک 1/4 www.DSNMC.ir Tel:+98(51) 38411524; +98(51)38472927
 ; +98(51)")
2
www.DSNMC.ir Pulmonary Embolism (cases and a brief review) V. R. Dabbagh Kakhki, M.D. Nuclear Medicine Specialist Associate Professor DSNMC Nuclear Medicine Research Center (NMRC; MUMS)
.")
4
Pretest Probability Epidemiology Extremely common subclinically Found at 70% of autopsies Clinical diagnosis is extremely inaccurate Only 33% of patients referred for V/Q scans

5
Pretest Probability Epidemiology Course of Disease 11% experience sudden death Diagnosis is not made in 63% Have 30% mortality rate 26%: Diagnosis is made and treated : 8% mortality rate

6
Clinical assessment Nonspecific Either dyspnea or tachypnea occur in 96% 85% have Po 2 <80 mm Hg Clinical symptoms of DVT Very insensitive and non-specific

7
Approach Respiratory symptoms Imaging of the chest for PE Diagnosis remain uncertain Venous imaging Pulmonary angiography

8
Venous imaging Contrast Venography Diagnostic standard of reference for DVT If negative excludes clinically significant DVT Induces DVT in as many as 8%

9
Venous imaging Ultrasonography Very sensitive and specific (95%) for DVTs above knee Less accurate for Calf & pelvis DVTs Asymptomatic DVTs (65% sensitive)
 for DVTs above knee Less accurate for Calf & pelvis DVTs Asymptomatic DVTs (65% sensitive)")
10
Pulmonary imaging Chest X-Ray Insensitive and non-specific for PE Signs suggesting PE Westermark’s sign Fleischner sing Hampton’s hump Most common signs Consolidation Atelectasis Small pleural effusion Diaphragmatic elevation To exclude clinical mimics of PE For comparison with the V/Q study

11
Pulmonary Imaging V/Q scan Lungs are composed of Pulmonary circulation Segmental distribution Bronchial circulation PE is segmental in nature

12
Pulmonary imaging V/Q scan

13
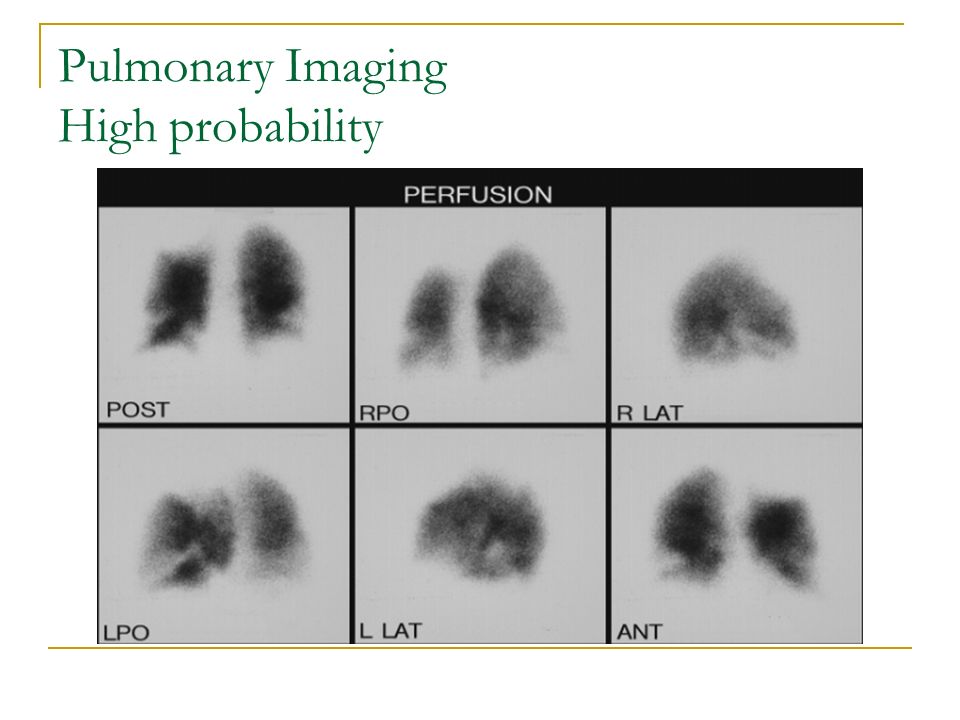
Pulmonary imaging Lung Perfusion Scan Performed with 99m Tc-MAA Shows regional perfusion of the lungs Very sensitive for PE

14
Pulmonary Imaging Lung perfusion scan Normal lung perfusion scan virtually excludes PE for practical purposes

15
Pulmonary Imaging Lung perfusion scan: Normal

16
Pulmonary Imaging Lung perfusion scan PE causes defects which are Segmental Pleural based Wedge-shaped

17
Pulmonary Imaging Lung perfusion scan

18
Many lung pathologies induce perfusion defects Ventilation scan and chest X-Rays are mandatory for comparison

19
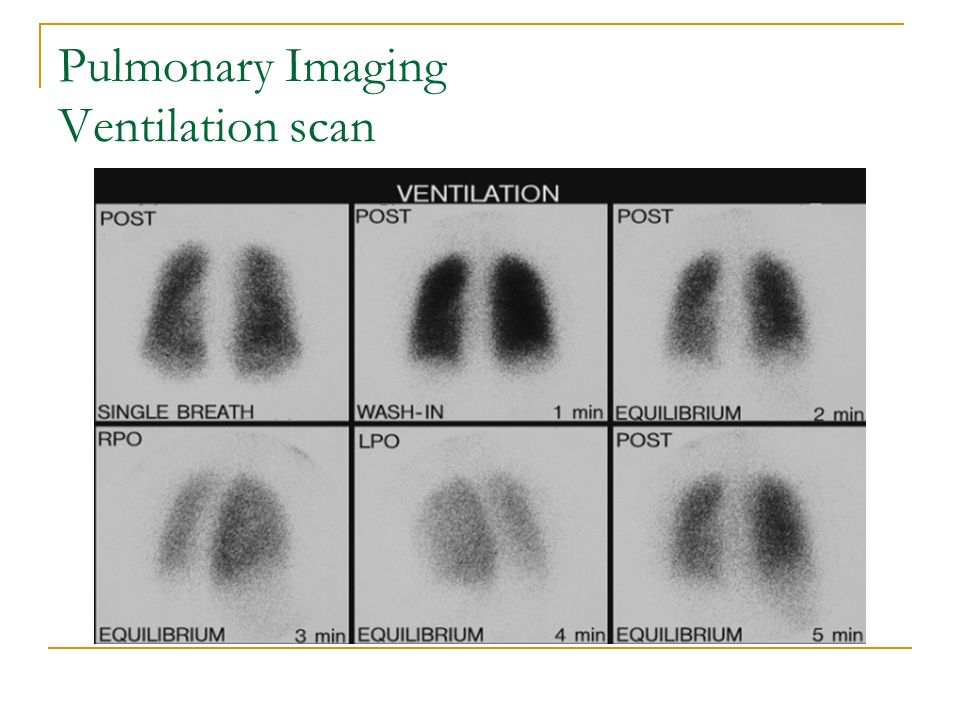
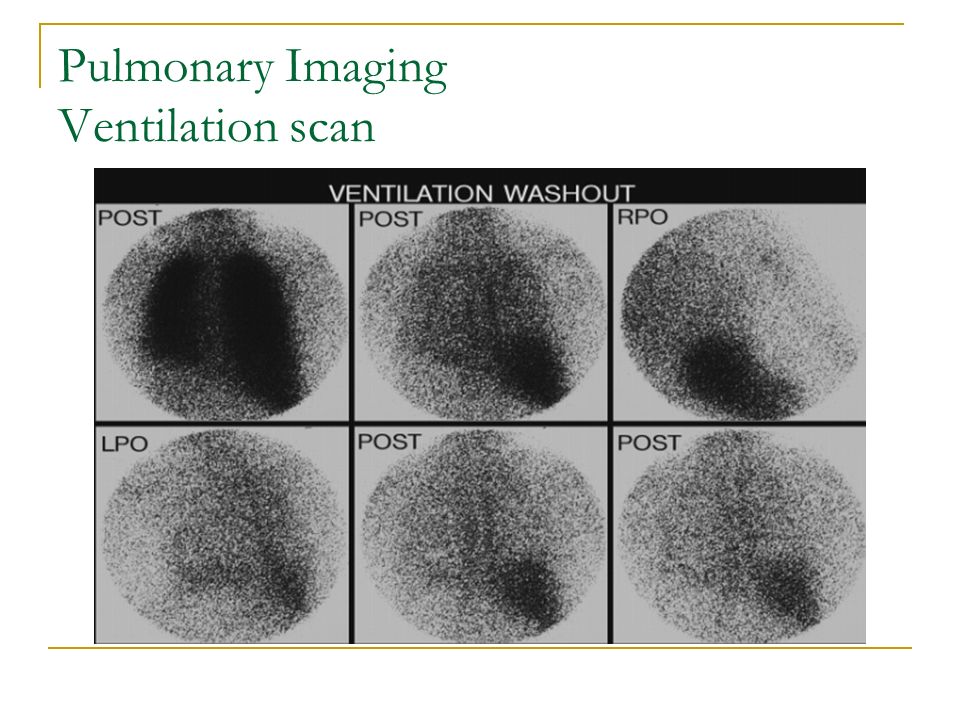
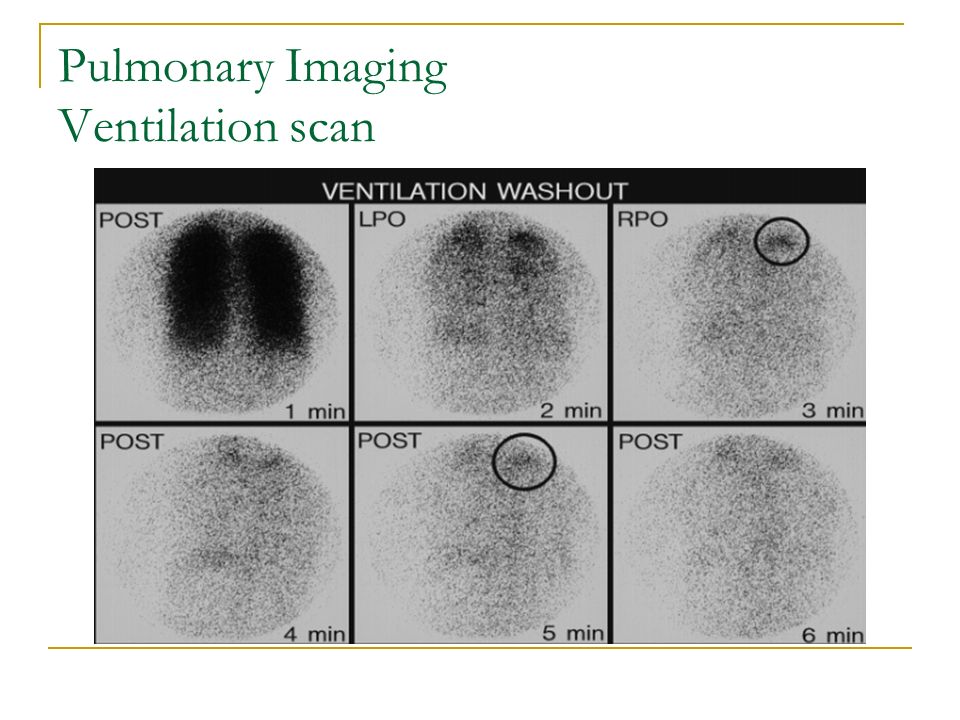
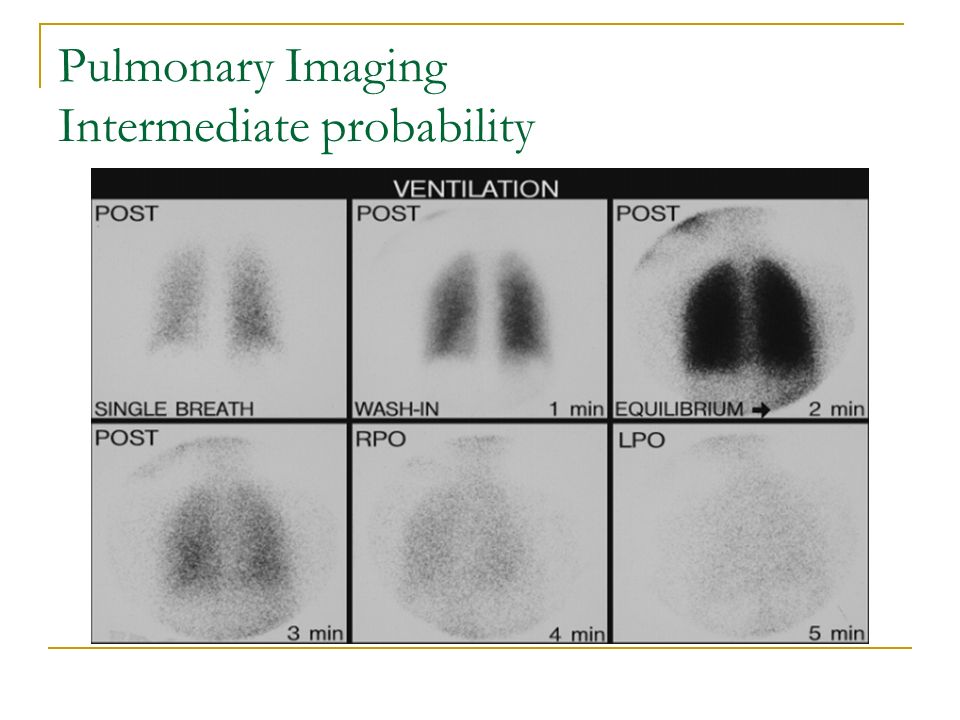
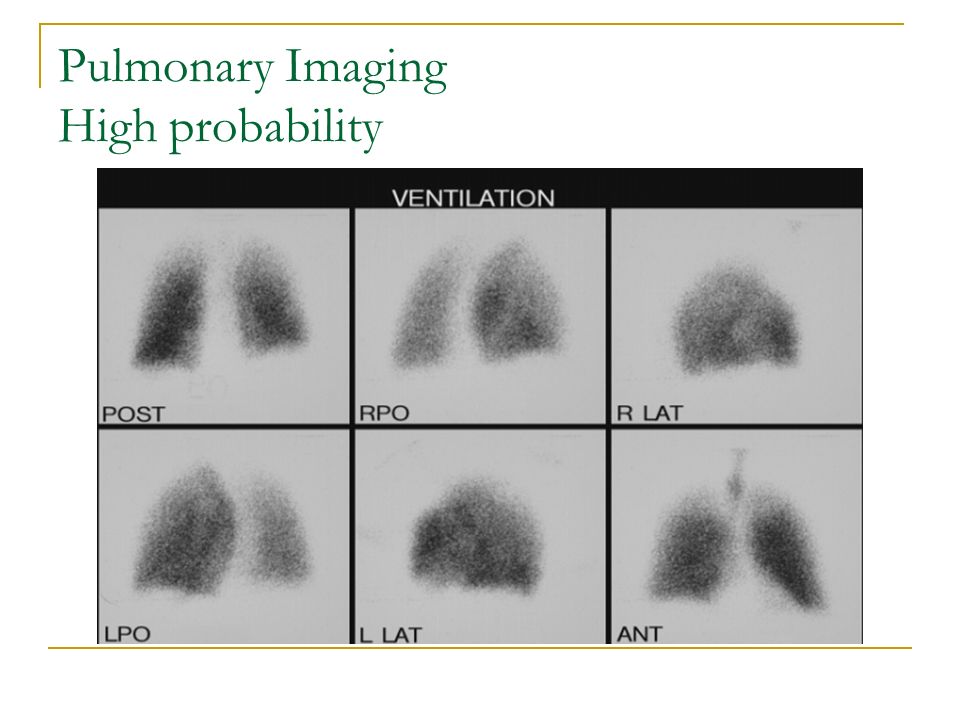
Pulmonary Imaging Ventilation scan Performed with 133 Xe(80 kev) A first-breath image(100 kcount) Equilibrium images Washout Phase 81m Kr 99m Tc labeled aerosols 99m Tc-DTPA 99m Tc-PYP 99m Tc-Technegas
 A first-breath image(100 kcount) Equilibrium images Washout Phase 81m Kr 99m Tc labeled aerosols 99m Tc-DTPA 99m Tc-PYP 99m Tc-Technegas")
20
Pulmonary Imaging Ventilation scan

24
PE Mimics Unresolved previous PE(35%) Intravenous drug abuse Hilar or mdiastinal involvement(LC) Other process occurring in the pulmonary arterial lumen(embolism of other than thrrombus, tumor) Arterial wall(vasculitis,TB,..) Vascular anomalies (peripheral coarctation) Extrinsic compression of pulmonary vessels
 Intravenous drug abuse Hilar or mdiastinal involvement(LC) Other process occurring in the pulmonary arterial lumen(embolism of other than thrrombus, tumor) Arterial wall(vasculitis,TB,..) Vascular anomalies (peripheral coarctation) Extrinsic compression of pulmonary vessels")
25
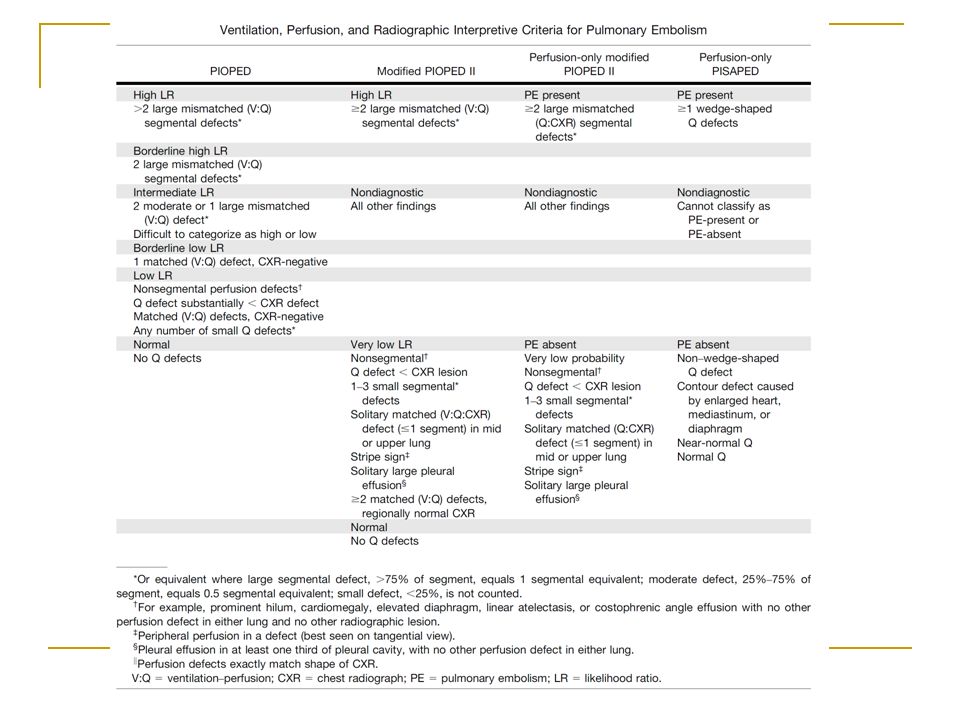
V/Q Scan Diagnostic Criteria PIOPED criteria modified PIOPED II criteria PISAPED criteria

26
Gestalt interpretation The experienced nuclear medicine physician may be able to provide a more accurate interpretation of the V/Q scan than is provided by the criteria alone V/Q Scan Diagnostic Criteria

28
Pulmonary Imaging PIOPED criteria By comparison of V,Q and chest X-Ray, V/Q study can be categorized as Low probability for PE <20% Intermediate Probability for PE 20-79% High probability for PE ≥80%

29
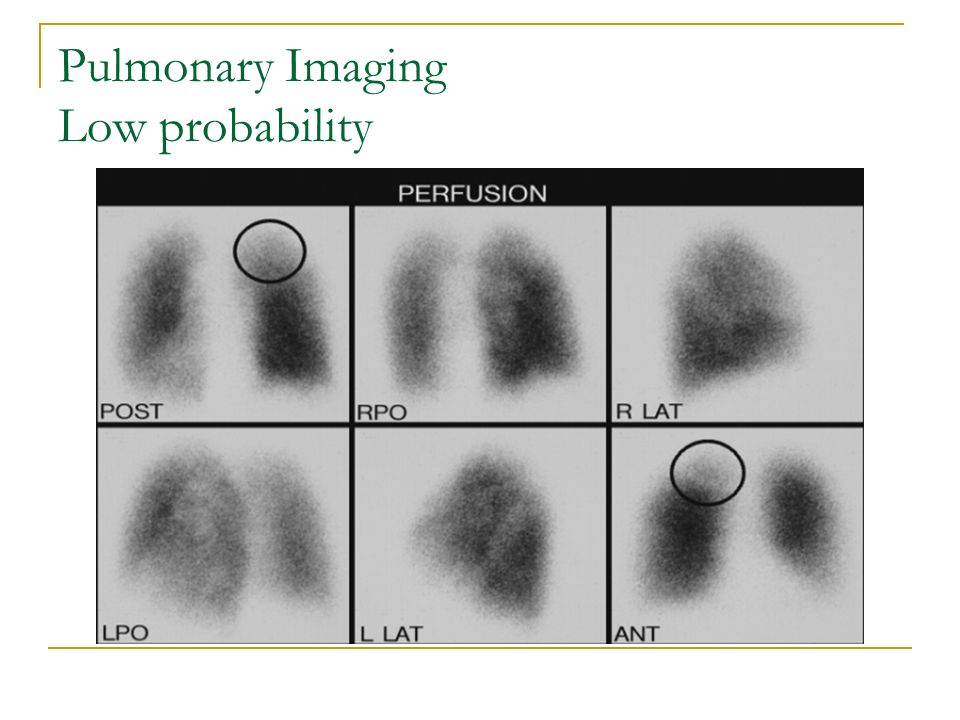
Pulmonary Imaging Low probability

31
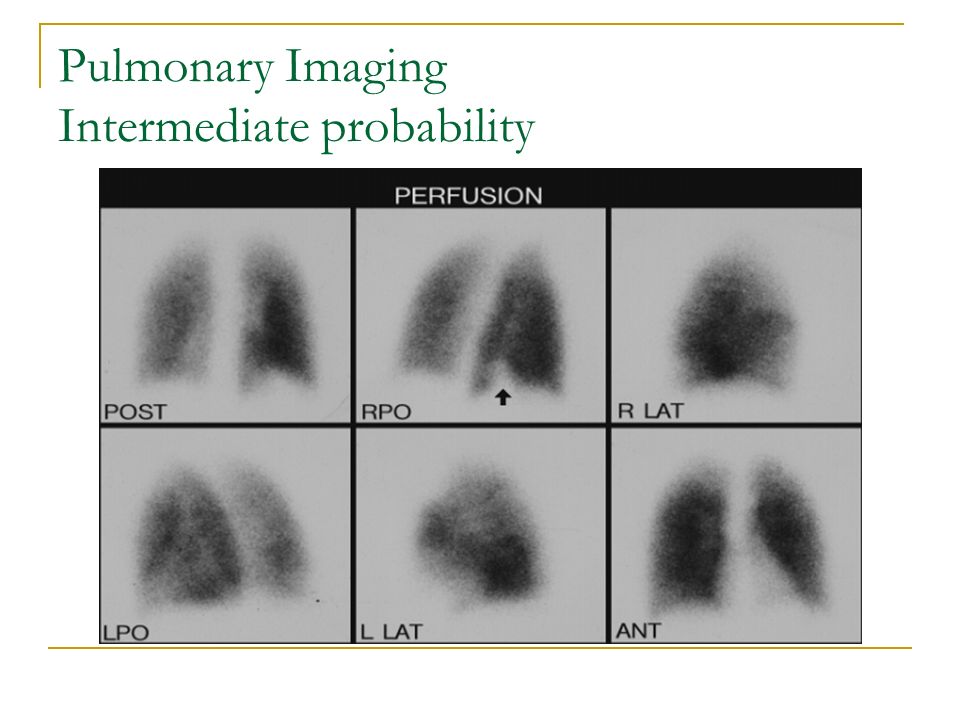
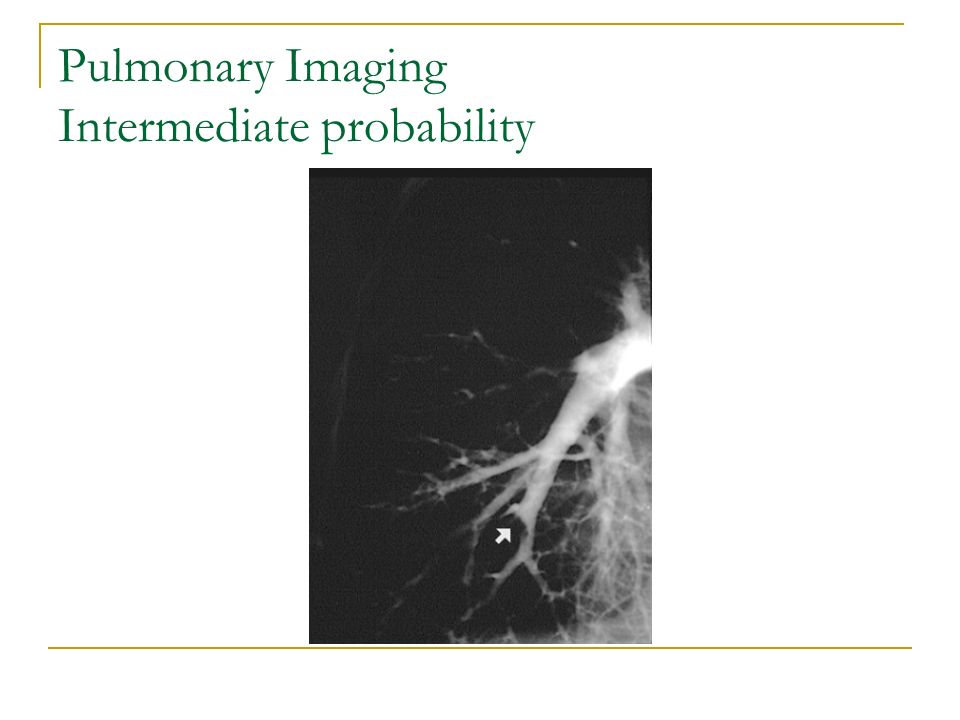
Pulmonary Imaging Intermediate probability

35
Pulmonary Imaging High probability

38
Pulmonary Imaging Spiral CT scan Overall sensitivity and specificity 80-85% and 90-95% Lower sensitivity than V/Q scan Not clinically relevant Indirect CT of the legs after pulmonary imaging Very promising for DVT detection

39
Assessment For PE

40
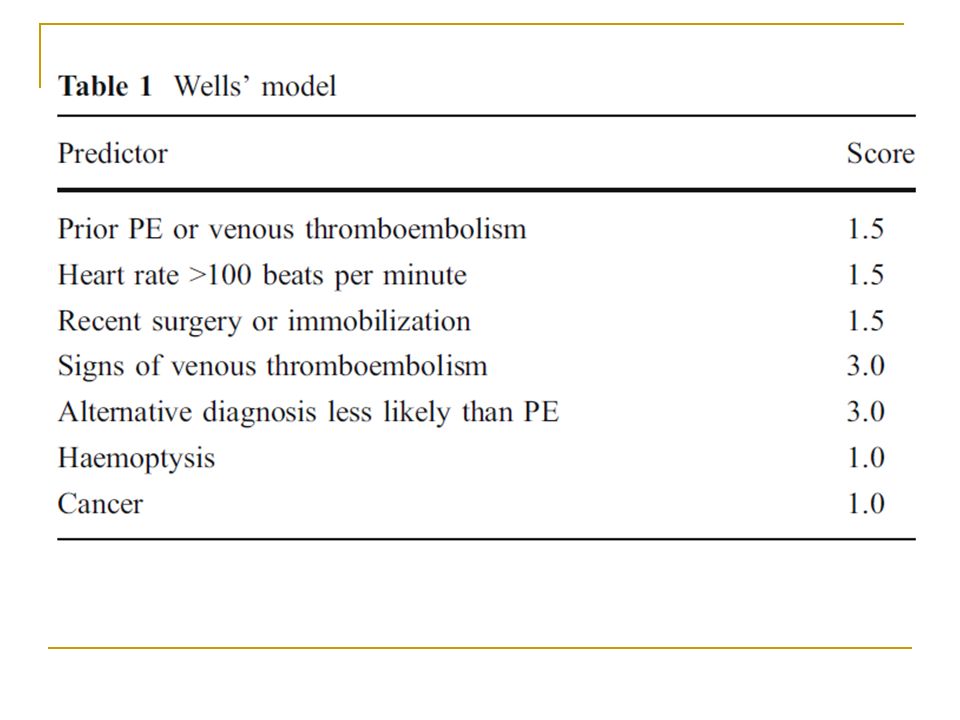
Assessment of the clinical probability of PE Wells’ model: the most frequently used prediction rule for suspected PE 7 variables The Wells’ model seems better suited to rule out rather than to rule in the diagnosis of PE and its performance is likely to be better in clinical settings where the prevalence of the disease is expected to be low

42
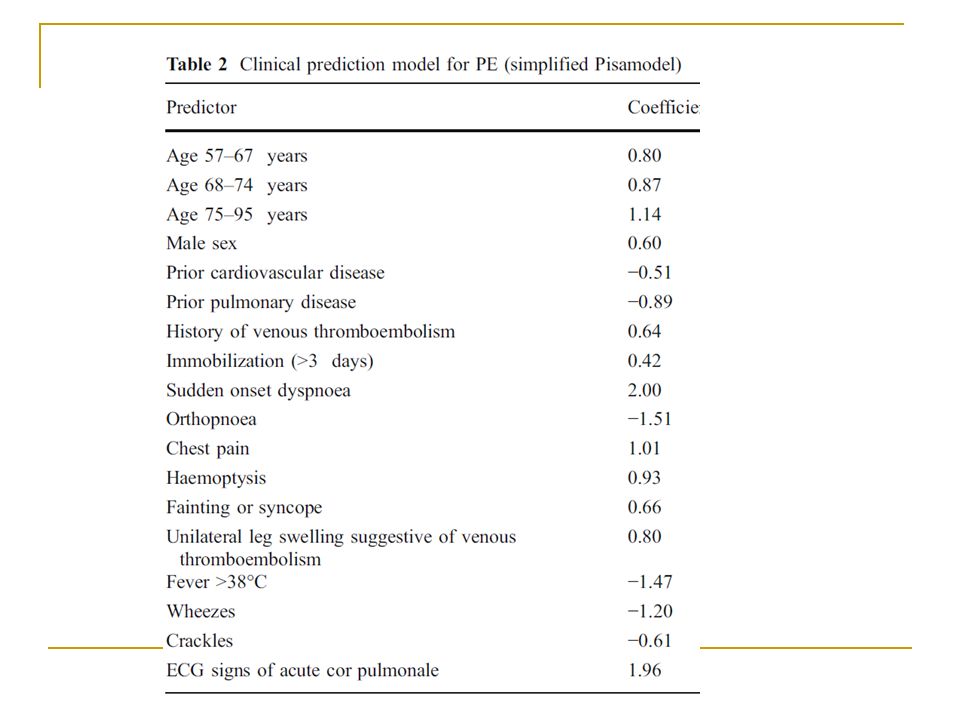
Simplified Pisamodel: Recently, a more precise prediction model 16 variables It performs equally well in detecting and in ruling out PE. Assessment of the clinical probability of PE

44
Clinical algorithm for investigation of patients with suspected PE

45
Stable Patients Diagnostic strategy in stable patients according to clinical probability of PE

46
Haemodynamically unstable PE Diagnostic strategy in patients with severe hypotension or shock

47
Diagnostic algorithms PE, when suspected, must be confirmed or refuted to avoid the risks of both over and under treatment: This requires imaging tests. Only optimal techniques are recommended. These are MDCT and V/Q Scan (SPECT) with holistic interpretation.
 with holistic interpretation..")
48
In each center, the algorithm applied for the diagnosis of PE must be based upon local circumstances, and first and foremost upon the availability of V/Q SPECT and MDCT. Diagnostic algorithms

49
V/Q SPECT carries no risk associated with contrast agent injection V/Q SPECT gives a much lower radiation burden V/Q SPECT yields a lower rate of nondiagnostic reports V/Q SPECT has higher sensitivity at similar specificity V/Q SPECT allows better estimation of PE extension based upon the functional impact of PE. V/Q Scan vs. MDCT

50
V/Q SPECT offers considerable advantages over other imaging techniques for the diagnosis of PE. its high sensitivity and specificity lower and predictable radiation burden its suitability for follow-up of patients with PE research into the natural history of PE V/Q Scan vs. MDCT

51
Algorithm for diagnostic imaging of patients with clinically suspected acute PE A: Clinical suspicion derived from Prediction Models. B: V/P SPECT is the procedure of choice V/Q = V/P

52
Algorithm for diagnostic imaging of patients with clinically suspected acute PE C: V/P SPECT is interpreted according to the holistic principle in which clinical pretest probability is a part. V/Q = V/P

53
Algorithm for diagnostic imaging of patients with clinically suspected acute PE D: a normal V/P SPECT is observed in the majority of cases and excludes PE in almost 100%.

54
Algorithm for diagnostic imaging of patients with clinically suspected acute PE E: Few cases are non-diagnostic; further diagnostic procedures are recommended, such as MDCT or in special cases PA. F: positive findings should lead to treatment in nearly all cases;

55
Algorithm for diagnostic imaging of patients with clinically suspected acute PE G: V/P Planar, holistically interpreted, or MDCT is recommended when V/P SPECT is not readily available.

56
Algorithm for diagnostic imaging of patients with clinically suspected acute PE H: V/P PLANAR is preferred on the basis of its better negative predictive value, no contraindications and much lower radiation exposure.

57
Algorithm for diagnostic imaging of patients with clinically suspected acute PE I: If V/P PLANAR or MDCT is positive treatment is warranted in most cases; in the context of a low pretest probability, a positive V/P PLANAR or a MDCT without direct visualization of the embolism is an indication for further investigation.

58
Algorithm for diagnostic imaging of patients with clinically suspected acute PE J: When V/ PPLANAR or MDCT is negative, further tests are indicated. K: When V/P PLANAR or MDCT is negative and the clinical suspicion of PE persists, further tests for PE should be performed.

59
Algorithm for diagnostic imaging of patients with clinically suspected acute PE L: V/P SPECT is the preferred additional test; if not available, MDCT should be followed by V/P PLANAR or vice versa; PA remains an alternative if the diagnosis remains unclear.

60
Algorithm for diagnostic imaging of patients with clinically suspected acute PE M: a normal V/P PLANAR excludes PE; where the V/P PLANAR is abnormal but negative for PE, or the MDCT is negative, PE is ruled out in those patients in whom clinical suspicion of PE is low

61
V.R.Dabbagh; DSNMC; www.DSNMC.ir

Similar presentations