Download presentation
Presentation is loading. Please wait.

1
Oral Anticoagulant and Antiplatelet Medications: Pharmacology Update
Stroke Fair 2015

2
Objectives Discuss guideline recommendations regarding use of oral antiplatelet and anticoagulant medications for stroke prevention. Review oral antiplatelet medications used for stroke prevention. Review oral anticoagulant medications used for stroke prevention.

3
Stroke Currently 5th leading cause of death in the US and a leading cause of disability. ~1 of every 20 deaths in the US ~795,000 strokes per year. 610,000 new 185,000 recurrent >690,000 ischemic By 2030, 3.88% of US population > 18 y/o is projected to have had a stroke. Increased prevalence of obesity increases in both HTN and DM Increased stroke burden among younger adults could increase dramatically Optimal treatment of risk factors critical to reduce stroke burden on society/individuals. Circulation. 2015;131:e29-e322. Stroke. 2013;44:

4
Risk Factors Modifiable Non-modifiable Age Sex Race/ Ethnicity
Physical inactivity Dyslipidemia Diet and nutrition Hypertension Obesity Diabetes Mellitus Smoking Atrial Fibrillation Other cardiac conditions (MI, cardiomyopathy, valvular heart disease, etc.) Age Sex Race/ Ethnicity Genetic Factors Family History of CVD at a young age Proinflammatory and prothrombotic factors >76 % of strokes are new events HTN considered most important, well-documented modifiable stroke risk factor Glycemic control reduces microvascular complications of DM, but inadequate evidence that improved control reduces risk of incident stroke. Effective prevention remains the best approach for reducing the burden of stroke. Age > 80 Black > white Usually women > men Stroke. 2013;44: Stroke. 2014; 45:
 Age. Sex. Race/ Ethnicity. Genetic Factors. Family History of CVD at a young age. Proinflammatory and prothrombotic factors. >76 % of strokes are new events. HTN considered most important, well-documented modifiable stroke risk factor. Glycemic control reduces microvascular complications of DM, but inadequate evidence that improved control reduces risk of incident stroke. Effective prevention remains the best approach for reducing the burden of stroke. Age > 80. Black > white. Usually women > men. Stroke. 2013;44: Stroke. 2014; 45:")
5
Antithrombotics for Primary Prevention
Atrial Fibrillation Anticoagulant or antiplatelet depending on risk factors Diabetes Mellitus Aspirin (unclear benefit for stroke prevention) Mechanical valves Warfarin + aspirin Bioprosthetic valves Aspirin +/- warfarin Mechanical mitral valve: INR low dose aspirin Bioprosthetic: aspirin + warfarin for first 3 months DM – several trials show no benefit vs no asa Stroke. 2014; 45:
 Mechanical valves. Warfarin + aspirin. Bioprosthetic valves. Aspirin +/- warfarin. Mechanical mitral valve: INR low dose aspirin. Bioprosthetic: aspirin + warfarin for first 3 months. DM – several trials show no benefit vs no asa. Stroke. 2014; 45:")
6
Atrial Fibrillation Non-valvular AF is associated with a 5-fold increased risk of stroke. AF-related stroke is likely to be more severe than non–AF-related stroke. Greater disability and mortality. Greater risk of recurrent stroke. Antithrombotic regimen is selected based on balance of risks and benefits. JACC. 2014; 64(21): e1-76.
: e1-76.")
7
CHA2DS2-VASc Risk Stratification for Nonvalvular AF
Risk Factor Score Congestive HF 1 Hypertension Age >/= 75 y/o 2 Diabetes mellitus Stroke/TIA/TE Vascular disease (prior MI, PAD, or aortic plaque) Age y Sex (female) 2014 AHA/ACC/HRS Guidelines for patients with non-valvular AF: Score = 0 (0.2% ischemic stroke rate per year) Reasonable to omit antithrombotic therapy. Score = 1 (0.6% rate) No antithrombotic therapy or treatment with an oral anticoagulant or aspirin may be considered. Score >/= 2 ( % rate) or prior stroke or TIA Oral anticoagulation recommended. When compared with the CHADS2 score, the CHA2DS2- VASc score for nonvalvular AF has a broader score range (0 to 9) and includes a larger number of risk factors (female sex, 65 to 74 years of age, and vascular disease) In a nationwide Danish registry from 1997 to 2008, the CHA2DS2-VASc index better discriminated stroke risk among subjects with a baseline CHADS2 score of 0 to 1 with an improved predictive ability. JACC. 2014; 64(21): e1-76.
 Age y. Sex (female) 2014 AHA/ACC/HRS Guidelines for patients with non-valvular AF: Score = 0 (0.2% ischemic stroke rate per year) Reasonable to omit antithrombotic therapy. Score = 1 (0.6% rate) No antithrombotic therapy or treatment with an oral anticoagulant or aspirin may be considered. Score >/= 2 ( % rate) or prior stroke or TIA. Oral anticoagulation recommended. When compared with the CHADS2 score, the CHA2DS2- VASc score for nonvalvular AF has a broader score. range (0 to 9) and includes a larger number of risk factors. (female sex, 65 to 74 years of age, and vascular disease) In a nationwide Danish registry from 1997 to 2008, the CHA2DS2-VASc index better discriminated stroke risk among subjects with a baseline CHADS2 score of 0 to 1 with an improved predictive ability. JACC. 2014; 64(21): e1-76.")
8
Treatment of Acute Ischemic Stroke and TIA
Antiplatelet agents Early initiation of ASA (within 48h) Do not administer antithrombotics within 24hr of treatment with IV alteplase Combination antiplatelet therapy may be beneficial Parenteral anticoagulation not recommended during the first 48 hours of acute ischemic stroke Increased risk of bleeding complications May be used for some ischemic stroke subtypes Limited evidence Antithrombotic treatment of acute ischemic stroke and transient ischemic attack. Uptodate.
 Do not administer antithrombotics within 24hr of treatment with IV alteplase. Combination antiplatelet therapy may be beneficial. Parenteral anticoagulation not recommended during the first 48 hours of acute ischemic stroke. Increased risk of bleeding complications. May be used for some ischemic stroke subtypes. Limited evidence. Antithrombotic treatment of acute ischemic stroke and transient ischemic attack. Uptodate.")
9
Secondary Prevention Noncardioembolic ischemic stroke or TIA
Antiplatelet agent ASA or ASA + dipyridamole Clopidogrel ASA + clopidogrel Anticoagulants (not recommended) Similar rate of vascular events but higher risk of bleeding with warfarin Newer anticoagulants not studied in recurrent stroke Cardioembolic stroke Recommendations vary with indication Clopidogrel – reasonable in place of ASA or Aggrenox; also in case of ASA allergy Clopidogrel + ASA – x21 days if initiated within 24hr of minor ischemic stroke or TIA (long-term use not recommended) Stroke. 2014; 45:
 Similar rate of vascular events but higher risk of bleeding with warfarin. Newer anticoagulants not studied in recurrent stroke. Cardioembolic stroke. Recommendations vary with indication. Clopidogrel – reasonable in place of ASA or Aggrenox; also in case of ASA allergy. Clopidogrel + ASA – x21 days if initiated within 24hr of minor ischemic stroke or TIA (long-term use not recommended) Stroke. 2014; 45:")
10
Selecting Antiplatelets for Secondary Prevention
Individualized decision to consider: patient risk factors, cost, tolerance, relative known efficacy. AHA guidelines: ASA or ASA + dipyridamole Clopidogrel may be used in place of the above or when pt is allergic to aspirin. Combination ASA + clopidogrel Can consider for initiation within 24 hr of minor ischemic stroke or TIA and continuation for 21 days. Long-term use increases risk of hemmorrhage. Stroke. 2014;45:

11
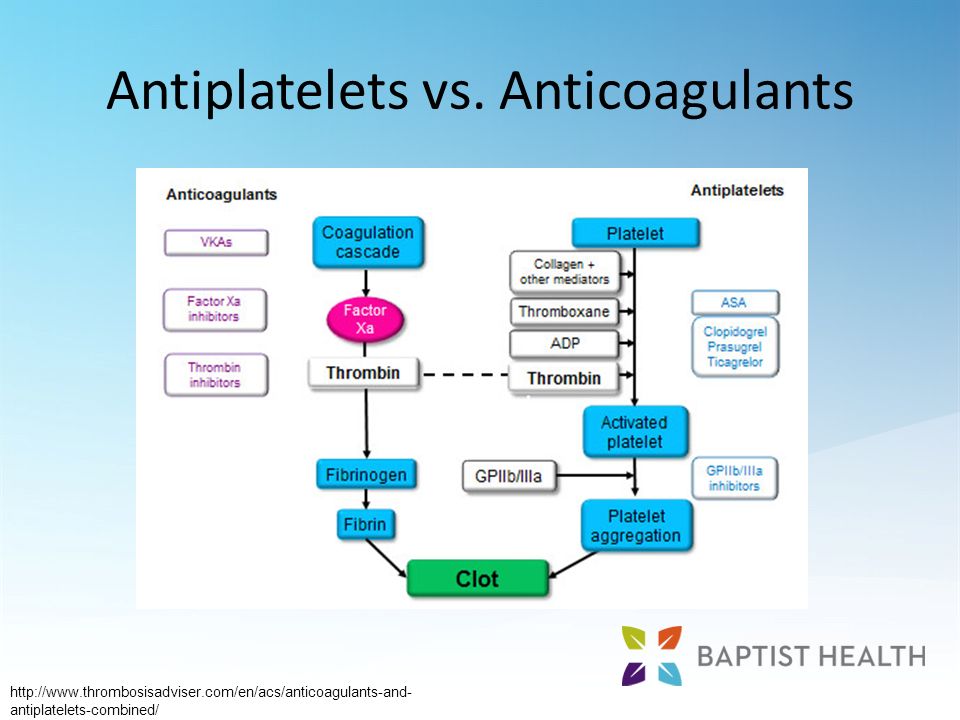
Antiplatelets vs. Anticoagulants
12
Antiplatelets Keep blood clots from forming by preventing platelet aggregation. Aspirin Cilostazol (Pletal) Clopidogrel (Plavix) Dipyridamole + Aspirin (Aggrenox) Prasugrel (Effient) Ticagrelor (Brilinta) Ticlopidine (Ticlid)
 Dipyridamole + Aspirin (Aggrenox) Prasugrel (Effient) Ticagrelor (Brilinta) Ticlopidine (Ticlid)")
13
Aspirin MOA: Inhibits cyclooxygenase, reducing production of thromboxane A2, a stimulator of platelet aggregation. Approved for: CVA, CVA prophylaxis, TIA treatment and prophylaxis. Available as immediate release and delayed release (enteric coated) Enteric coating protects against erosion but does not reduce GI bleeding incidence in studies Potential reduced efficacy of enteric coated ASA, especially at low doses GI injury severe enough to induce bleeding is thought to reflect systemic effects, not just local effects. Enteric coated ASA: should not be used for acute events – if used, should be crushed or chewed. For chronic administration, doses higher than 81mg may be necessary. Nonresponse and resistance to aspirin. Uptodate. NSAIDs (including aspirin): Primary prevention of gastroduodenal toxicity. Uptodate.
 Enteric coating protects against erosion but does not reduce GI bleeding incidence in studies. Potential reduced efficacy of enteric coated ASA, especially at low doses. GI injury severe enough to induce bleeding is thought to reflect systemic effects, not just local effects. Enteric coated ASA: should not be used for acute events – if used, should be crushed or chewed. For chronic administration, doses higher than 81mg may be necessary. Nonresponse and resistance to aspirin. Uptodate. NSAIDs (including aspirin): Primary prevention of gastroduodenal toxicity. Uptodate.")
14
Aspirin Dose: Most studies have found that lower doses of ASA are as effective as higher doses for secondary stroke prevention. Magnitude of benefit similar for doses ranging from mg. Higher doses associated with highest risk of GI toxicity. Side effects: GI upset, GI bleeding Low doses (</= 325mg) ASA at prolonged intervals annual risk of serious GI hemmorhage is ~0.4% (2.5 x the risk for non-users) Stroke. 2014;45:
 ASA at prolonged intervals annual risk of serious GI hemmorhage is ~0.4% (2.5 x the risk for non-users) Stroke. 2014;45:")
15
Dipyridamole + Aspirin (Aggrenox)
Dipyridamole: Impairs platelet function by inhibiting the activity of adenosine deaminase and phosphodiesterase. Beneficial effects of ASA and dipyridamole appear to be additive. As effective as ASA for secondary stroke prevention in trials. Stroke. 2014;45:

16
Dipyridamole + Aspirin (Aggrenox)
Dose: ASA 25mg/ dipyridamole 200mg PO twice daily Do not crush or chew Side effects: headache (incidence declines with continued use), GI upset, diarrhea. Higher rate of side effects and early discontinuation in clinical trials.
, GI upset, diarrhea. Higher rate of side effects and early discontinuation in clinical trials.")
17
Clopidogrel (Plavix) Irreversibly inhibits ADP-dependent platelet aggregation. Approved for: cerebrovascular accident prophylaxis. Dose: 75mg PO once daily Compared to ASA and ASA/dipyridamole (CAPRIE and PRoFESS trials): similar rates of primary outcomes. Stroke. 2014;45:
: similar rates of primary outcomes. Stroke. 2014;45:")
18
Clopidogrel (Plavix) Genetic differences in hepatic enzymes or P2Y12 receptor may affect response to clopidogrel. Not enough evidence to recommend routine genetic testing. Side effects: rash and diarrhea (>ASA); GI upset and GI bleeding (<ASA). Proton pump inhibitors may reduce effectiveness of clopidogrel. H2 blocker or pantoprazole preferred Carriers of at least 1 CYP2C19 reduced-function allele had a relative reduction of 32% in plasma exposure to the active metabolite of clopidogrel compared with noncarriers (P<0.001).
; GI upset and GI bleeding (<ASA). Proton pump inhibitors may reduce effectiveness of clopidogrel. H2 blocker or pantoprazole preferred. Carriers of at least 1 CYP2C19 reduced-function allele had a relative reduction of 32% in plasma exposure to the active metabolite of clopidogrel compared with noncarriers (P<0.001).")
19
Ticlopidine (Ticlid) Irreversibly alters the function of platelet membranes by preventing ADP from stimuating platelet-fibrinogen binding and subsequent interactions between platelets. Approved for: Prevention of thromboembolic stroke. Conflicting results in clinical trials. 3 randomized trials in patients with cerebrovascular disease: superior to placebo in one, superior to ASA in one, no benefit compared to ASA in the third Stroke. 2014;45:

20
Ticlopidine (Ticlid) Side effects: Rash, diarrhea
May cause severe neutropenia: biweekly CBC required for 3 months Not considered first line due to high cost and side effects

21
Cilostazol (Pletal) Phosphodiesterase 3 inhibitor
Non-FDA approved indication: cerebrovascular accident prevention. Mainly used for intermittent claudication in patients with peripheral artery disease. Controlled trials demonstrate effectiveness in preventing cerebral infarction (in Asian populations). Lower rate of intracranial hemorrhages. Higher cost, lower tolerability than aspirin. Stroke. 2014;45:
. Lower rate of intracranial hemorrhages. Higher cost, lower tolerability than aspirin. Stroke. 2014;45:")
22
Other Antiplatelets NOT approved for stroke prevention
Prasugrel (Effient) FDA approved indication: acute coronary syndrome (ACS) managed with percutaneous coronary intervention (PCI). Used with aspirin Do not use in patients with history of TIA or stroke (increased risk of bleeding). Not recommended in patients > 75 y/o. Ticagrelor (Brilinta) FDA-approved indication: ACS with or without PCI Do not use aspirin dose > 100mg daily. Potential reduced efficacy of ticagrelor ACS= unstable angina, NSTEMI, STEMI
 FDA approved indication: acute coronary syndrome (ACS) managed with percutaneous coronary intervention (PCI). Used with aspirin. Do not use in patients with history of TIA or stroke (increased risk of bleeding). Not recommended in patients > 75 y/o. Ticagrelor (Brilinta) FDA-approved indication: ACS with or without PCI. Do not use aspirin dose > 100mg daily. Potential reduced efficacy of ticagrelor. ACS= unstable angina, NSTEMI, STEMI.")
23
Oral Anticoagulants Disrupt parts of the coagulation cascade, preventing fibrin clots from forming or enlarging. Apixaban (Eliquis) Dabigatran etexilate (Pradaxa) Edoxaban (Savaysa) Rivaroxaban (Xarelto) Warfarin (Coumadin)
 Dabigatran etexilate (Pradaxa) Edoxaban (Savaysa) Rivaroxaban (Xarelto) Warfarin (Coumadin)")
24
Clotting Cascade

25
Vitamin K Antagonists Blocks regeneration of Vitamin K epoxide, inhibiting synthesis of vitamin K dependent clotting factors 2, 7, 9, 10, and the anticoagulant proteins C and S. Warfarin (Coumadin)
")
26
Warfarin (Coumadin) Oral anticoagulant approved for prophylaxis of thromboembolic disorders related to prosthetic cardiac valve and atrial fibrillation. Dose is based on INR (usual target 2-3) INR may be affected by vitamin K intake. Consistent dietary and supplement intake is necessary. Multiple drug interactions. For patients with tilting disk or bileaflet mechanical valve in the mitral position or caged ball or caged disk valves (combination with aspirin), a target INR of 3 (range, 2.5 to 3.5) is recommended
 INR may be affected by vitamin K intake. Consistent dietary and supplement intake is necessary. Multiple drug interactions. For patients with tilting disk or bileaflet mechanical valve in the mitral position or caged ball or caged disk valves (combination with aspirin), a target INR of 3 (range, 2.5 to 3.5) is recommended.")
27
Warfarin (Coumadin) Bridge therapy sometimes required
Routine lab monitoring required Reversal agent: Vitamin K Side Effects: Bleeding Purple toe syndrome Alopecia Nausea/vomiting Diarrhea Chills/ feeling cold

28
Warfarin (Coumadin) Discontinue approximately 5 days prior to surgery to provide sufficient time for INR to normalize Use with parenteral anticoagulants only for bridge therapy

29
Novel Oral Anticoagulants (NOACs)
Direct thrombin inhibitors and direct factor Xa inhibitors. No blinded head to head trial comparisons between NOACs For A. fib, NOACs associated with (compared to warfarin) – depending on the drug: Significant reduction in stroke/ systemic embolism Significant relative reduction in hemorrhagic stroke and all cause mortality Reduced major bleeding Reduced major bleeding: significant for Apixaban, edoxaban Reduced hemorrhagic stroke: All Significant reduction in stroke/ systemic embolism: superiority shown for dabigatran, apixaban; Noninferiority for rivaroxaban, edoxaban Atrial fibrillation: Anticoagulant therapy to prevent embolization. Uptodate.
 – depending on the drug: Significant reduction in stroke/ systemic embolism. Significant relative reduction in hemorrhagic stroke and all cause mortality. Reduced major bleeding. imageKey=CARD%2F80932&topicKey=CARD%2F1031&source=see_link&utdPopup=true. Reduced major bleeding: significant for Apixaban, edoxaban. Reduced hemorrhagic stroke: All. Significant reduction in stroke/ systemic embolism: superiority shown for dabigatran, apixaban; Noninferiority for rivaroxaban, edoxaban. Atrial fibrillation: Anticoagulant therapy to prevent embolization. Uptodate.")
30
NOACs Advantages Disadvantages Convenience
Lack of dietary interactions Fewer drug interactions Lack of efficacy and safety data in patients with severe CKD Lack of easily available monitoring of blood levels (and compliance) Higher cost Lack of reversal agents Potential for unanticipated side effects Atrial fibrillation: Anticoagulant therapy to prevent embolization. Uptodate.
 Higher cost. Lack of reversal agents. Potential for unanticipated side effects. Atrial fibrillation: Anticoagulant therapy to prevent embolization. Uptodate.")
31
Direct Thrombin Inhibitor
Prevents formation of clots by directly blocking thrombin. Can be reversed with Praxbind 5mg once Dabigatran (Pradaxa)
")
32
Dabigatran (Pradaxa) Oral anticoagulant approved for stroke prevention in atrial fibrillation. Normal dose is 150mg BID Renal dose (CrCl<30) 75 mg BID Do not use with CrCl < 15 or in dialysis patients Can be taken without regards to meals Capsule should never be chewed, crushed, or opened. Bioavailability increases 75% when capsule opened Must be stored in original packaging Cannot put in a pill organizer Twice daily med – must remain in blister pack until used for stability reasons. If drug is still in manufactuerer bottle it is good for 4 months from the date the bottle was opened
 75 mg BID. Do not use with CrCl < 15 or in dialysis patients. Can be taken without regards to meals. Capsule should never be chewed, crushed, or opened. Bioavailability increases 75% when capsule opened. Must be stored in original packaging. Cannot put in a pill organizer. Twice daily med – must remain in blister pack until used for stability reasons. If drug is still in manufactuerer bottle it is good for 4 months from the date the bottle was opened.")
33
Dabigatran (Pradaxa) No bridge therapy required
No routine lab monitoring Idarucizumab (Praxbind) approved 10/2015 for reversal! Side Effects Esophagitis Gastritis GERD GI hemorrhage Bleeding Indigestion Apcc – activated prothrombin complex concentrate – has been approved and is available at BHE but not much data available for its use – it is a possible reversal agent for emergent bleeds, it contains 4 clotting factors PRAXBIND – just approved
 approved 10/2015 for reversal! Side Effects. Esophagitis. Gastritis. GERD. GI hemorrhage. Bleeding. Indigestion. Apcc – activated prothrombin complex concentrate – has been approved and is available at BHE but not much data available for its use – it is a possible reversal agent for emergent bleeds, it contains 4 clotting factors. PRAXBIND – just approved.")
34
Dabigatran (Pradaxa) Discontinue use 1-6 days prior to invasive procedure or surgery. Based on renal function and bleeding risk of procedure. Do NOT use with other anticoagulants Anticoagulants.. oral and injectable Heparin Enoxaparin (Lovenox) Fondaparinux (Arixtra) Warfarin Dabigatran (Pradaxa) Rivaroxaban (Xarelto) Apixaban (Eliquis) Edoxaban (Savaysa) This includes epidurals Should not be used with anticoagulants but may see it used with antiplatelet agents
 Fondaparinux (Arixtra) Warfarin. Dabigatran (Pradaxa) Rivaroxaban (Xarelto) Apixaban (Eliquis) Edoxaban (Savaysa) This includes epidurals. Should not be used with anticoagulants but may see it used with antiplatelet agents.")
35
Factor Xa Inhibitors Prevents clots by inhibiting factor Xa
“Oral Arixtra” Rivaroxaban (Xarelto) Apixaban (Eliquis) Edoxaban (Savaysa) In development: betrixaban
 Apixaban (Eliquis) Edoxaban (Savaysa) In development: betrixaban.")
36
Rivaroxaban (Xarelto)
Oral anticoagulant approved for DVT prophylaxis post knee and hip surgery Stroke prevention in atrial fibrillation DVT and PE treatment and secondary prophylaxis Dose differs based on indication A. fib: 20mg once daily Crcl ml/min: 15 mg once daily Crcl < 15 ml/min: avoid use 15 mg to 20 mg doses should be taken with food to increase absorption. Take with largest meal of the day (usually supper) If crushed, must be administered into the stomach. Reduced bioavailability if administered into proximal intestine.
 If crushed, must be administered into the stomach. Reduced bioavailability if administered into proximal intestine.")
37
Rivaroxaban (Xarelto)
No bridge therapy required No routine lab monitoring No reversal agent Do NOT use with other anticoagulants Anticoagulants.. oral and injectable Heparin Enoxaparin (Lovenox) Fondaparinux (Arixtra) Warfarin Dabigatran (Pradaxa) Rivaroxaban (Xarelto) Apixaban (Eliquis) Apcc – activated prothrombin compex concentrate – has been approved and is available at BHE but not much data available for its use – it is a possible reversal agent for emergent bleeds, it contains 4 clotting factors Don’t use with other anticoagulants but may see this used with antiplatelet agents
 Fondaparinux (Arixtra) Warfarin. Dabigatran (Pradaxa) Rivaroxaban (Xarelto) Apixaban (Eliquis) Apcc – activated prothrombin compex concentrate – has been approved and is available at BHE but not much data available for its use – it is a possible reversal agent for emergent bleeds, it contains 4 clotting factors. Don’t use with other anticoagulants but may see this used with antiplatelet agents.")
38
Rivaroxaban (Xarelto)
Discontinue use 1-4 days prior to invasive procedure or surgery. Based on renal function and bleeding risk of procedure. Side Effects: Increased bleeding GI hemorrhage Epidural hematoma This includes epidurals

39
Apixaban (Eliquis) Oral anticoagulant approved for: Dose – 5mg BID
A fib – CVA/embolus prophylaxis DVT/PE treatment VTE prophylaxis postop arthroplasty of knee or hip Dose – 5mg BID Do not use with severe hepatic impairment Decrease to 2.5mg BID IF 2 or more of the following are present Age >/= 80 Weight </= 60 kg Serum Cr >/= 1.5mg/dL May be crushed. May be administered with or without food.

40
Apixaban (Eliquis) No bridge therapy required
No routine lab monitoring No reversal agent Do NOT use with other anticoagulants Anticoagulants.. oral and injectable Heparin Enoxaparin (Lovenox) Fondaparinux (Arixtra) Warfarin Dabigatran (Pradaxa) Rivaroxaban (Xarelto) Apixaban (Eliquis) Edoxaban (Savaysa) This includes epidurals
 Fondaparinux (Arixtra) Warfarin. Dabigatran (Pradaxa) Rivaroxaban (Xarelto) Apixaban (Eliquis) Edoxaban (Savaysa) This includes epidurals.")
41
Apixaban (Eliquis) Side Effects
Bleeding GI hemorrhage Intracranial hemorrhage Discontinue use 1-4 days prior to invasive procedure or surgery. Based on renal function and bleeding risk of procedure. This includes epidurals

42
Edoxaban (Savaysa) Newest oral anticoagulant approved for:
Stroke prevention in atrial fibrillation DVT/ PE Dose – 60 mg once daily Crcl ml/min: 30mg once daily Crcl < 15 ml/min: not recommended Do not use in moderate or severe hepatic impairment Do not use for atrial fibrillation if Crcl > 95 ml/min Increased risk of ischemic stroke May be crushed. Administer with or without food.

43
Edoxaban (Savaysa) No bridge therapy required
No routine lab monitoring No reversal agent Do NOT use with other anticoagulants Anticoagulants.. oral and injectable Heparin Enoxaparin (Lovenox) Fondaparinux (Arixtra) Warfarin Dabigatran (Pradaxa) Rivaroxaban (Xarelto) Apixaban (Eliquis) Edoxaban (Savaysa)
 Fondaparinux (Arixtra) Warfarin. Dabigatran (Pradaxa) Rivaroxaban (Xarelto) Apixaban (Eliquis) Edoxaban (Savaysa)")
44
Edoxaban (Savaysa) Discontinue prior to surgery Side Effects: Bleeding
At least 24 hours prior to procedure Reinstate once adequate hemostasis is established Side Effects: Bleeding Rash Abnormal liver function tests

45
Betrixaban In development Once daily dosing Low renal clearance
Studied in patients with all degrees of renal dysfunction. No significant CYP3A4 metabolism Currently in Phase 3 trial – seeking approval for hospital and post-discharge prevention of VTE in acute medically ill patients.

46
Bleeding Risk Letter Clinical Characteristic Points H Hypertension 1 A Abnormal liver or renal function 1 or 2 S Stroke B Bleeding L Labile INR E Elderly (age>65) D Drugs or Alcohol Most common tool used to assess bleeding risk: HAS-BLED score. Should be used to identify risk factors or define patients at elevated bleeding risk, not to determine who should or should not receive anticoagulation. Bleeding risk scores to quantify hemorrhage risk include HAS-BLED (Hypertension, Abnormal renal/liver function, Stroke, Bleeding history or predisposition, Labile INR, Elderly, Drugs/alcohol concomitantly), RIETE (Computerized Registry of Patients With Venous Thromboembolism), HEMORR2HAGES (Hepatic or Renal Disease, Ethanol Abuse, Malignancy, Older Age, Reduced Platelet Count or Function, Rebleeding, Hypertension, Anemia, Genetic Factors, Excessive Fall Risk and Stroke), and ATRIA (Anticoagulation and Risk Factors in Atrial Fibrillation) Points 1 2 3 4 5 Annual bleed rate 0.9% 3.4% 4.1% 5.8% 8.9% 9.1% JACC. 2014; 64(21): e1-76.
 D. Drugs or Alcohol. Most common tool used to assess bleeding risk: HAS-BLED score. Should be used to identify risk factors or define patients at elevated bleeding risk, not to determine who should or should not receive anticoagulation. Bleeding risk scores to quantify hemorrhage risk. include HAS-BLED (Hypertension, Abnormal renal/liver. function, Stroke, Bleeding history or predisposition, Labile INR, Elderly, Drugs/alcohol concomitantly), RIETE. (Computerized Registry of Patients With Venous Thromboembolism), HEMORR2HAGES (Hepatic or Renal Disease, Ethanol Abuse, Malignancy, Older Age, Reduced. Platelet Count or Function, Rebleeding, Hypertension, Anemia, Genetic Factors, Excessive Fall Risk and Stroke), and ATRIA (Anticoagulation and Risk Factors in Atrial. Fibrillation) Points Annual bleed rate. 0.9% 3.4% 4.1% 5.8% 8.9% 9.1% JACC. 2014; 64(21): e1-76.")
47
Emergent Antithrombotic Reversal
For life-threatening bleeds or emergent surgery Antiplatelet drugs Platelet infusion No specific reversal agents Warfarin Phytonadione (Vitamin K) 10mg IV FEIBA (activated prothombin complex concentrate) Dose depends on INR and site of bleeding FEIBA for warfarin: INR</= 5 = 500 units IV (do not exceed 2 units/kg/min infusion rate) INR > 5 OR intracranial bleed = 1000 units IV (do not exceed infusion rate of 2 units/kg/min) Recheck INR in 30 minutes, if > 1.5 contact physician to determine if another 500 units is needed.
 10mg IV. FEIBA (activated prothombin complex concentrate) Dose depends on INR and site of bleeding. FEIBA for warfarin: INR</= 5 = 500 units IV (do not exceed 2 units/kg/min infusion rate) INR > 5 OR intracranial bleed = 1000 units IV (do not exceed infusion rate of 2 units/kg/min) Recheck INR in 30 minutes, if > 1.5 contact physician to determine if another 500 units is needed.")
48
Emergent Antithrombotic Reversal
Direct thrombin inhibitor Idarucizumab (Praxbind) FEIBA 50 units/kg IV x1 Emergent hemodialysis (removes ~60% in 2-3 hr) Activated charcoal (if within 2hrs of ingestion) Factor Xa inhibitors FFP if bleeding still not controlled Activated charcoal (if within 8hrs of ingestion) Dialysis not useful for factor Xa inhibitors due to high protein-binding
 FEIBA 50 units/kg IV x1. Emergent hemodialysis (removes ~60% in 2-3 hr) Activated charcoal (if within 2hrs of ingestion) Factor Xa inhibitors. FFP if bleeding still not controlled. Activated charcoal (if within 8hrs of ingestion) Dialysis not useful for factor Xa inhibitors due to high protein-binding.")
49
FEIBA Activated prothrombin complex concentrate.
Contains inactivated factors II, IX, and X and activated factor VII No indication and not well studied for treatment of bleeding due to anticoagulants. Dosing comes from literature, not package insert. Should be used for life threatening bleeds only. Substantial risk for thrombotic and thromboembolic events. FDA indications for hemophilia A or B – prophylaxis or control of bleeding (with factor VIII or IX inhibitors) Increased thrombosis risk – evidence comes from studies involving hemophilia patients. Theoretically, higher risk with patients on anticoagulant due to pt’s baseline higher risk of thrombosis (reason for anticoagulation initially)
 Increased thrombosis risk – evidence comes from studies involving hemophilia patients. Theoretically, higher risk with patients on anticoagulant due to pt’s baseline higher risk of thrombosis (reason for anticoagulation initially)")
50
FEIBA Available in 500 unit, 1000 unit, and 2500 unit (approximate) strengths All units / kg doses will be rounded to the nearest vial size Dispensed from pharmacy: Volumes ≤ 20mL in syringe Volumes > 20mL in 50mL empty bag

51
Targeted Reversal Agents
Idarucizumab (Praxbind) – FDA approval 10/2015 dabigatran reversal Humanized dabigatran-specific antibody fragments RE-VERSE AD study Rapidly and completely reversed anticoagulation in 88-98% of patients who had elevated clotting times at baseline Andexanet alfa: Factor Xa inhibitor reversal Recombinant modified human Factor Xa molecule Studies underway REVERSE-AD: used dilute thrombin times and ecarin clotting times to evaluate efficacy Management of bleeding in patients receiving direct oral anticoagulants. Uptodate. N Engl J Med 2015;373:
 – FDA approval 10/2015. dabigatran reversal. Humanized dabigatran-specific antibody fragments. RE-VERSE AD study. Rapidly and completely reversed anticoagulation in 88-98% of patients who had elevated clotting times at baseline. Andexanet alfa: Factor Xa inhibitor reversal. Recombinant modified human Factor Xa molecule. Studies underway. REVERSE-AD: used dilute thrombin times and ecarin clotting times to evaluate efficacy. Management of bleeding in patients receiving direct oral anticoagulants. Uptodate. N Engl J Med 2015;373:")
52
Idarucizumab (Praxbind)
DOSE – 5gm IV given as a push or infusion Adverse reactions: Hypokalemia No dose adjustments needed Constipation Delirium CAUTION - hereditary fructose intolerance PNA Fever Consider restarting dabigatran within 24 hours of administration Hypersensitivity reaction $3500 per dose

53
Summary Use of antithrombotic therapy for stroke prevention requires careful consideration of a patient’s history and risk factors. Multiple antiplatelet and anticoagulant options available to provide individualization of therapy based on patient-specific factors. Antithrombotic medications have many other uses not related to stroke prevention.

Similar presentations






 Dabigatran and Rivaroxaban for the prevention of stroke and systemic embolism in nonvalvular atrial fibrillation Dr Dipti.>")









>")


