Download presentation
Presentation is loading. Please wait.

1
The Respiratory System: History and Physical Assessment

2
Physiologic Function of the Lungs
Exchange respiratory gases Maintenance of acid-base balance

3
Primary Muscles of Respiration
Diaphragm External Intercostals Inspiration active, 70% of your tidal volume is provided from your diaphragm movement, 30% from your external Intercostals Inspiration 1/3 of your respiratory cycle, expiration 2/3 Diaphragm moves down with inspiration, pushing lowering abdominal content to increase the intrathoracic space. External Intercostals increase anteroposterior diameter Normal respiratory rate 12-20, in elderly Discuss changes in the elderly: barrel chest from loss of muscle strength in thorax and diaphragm, less compliance, skeletal changes an increase in the dorsal curve of the thoracic spine, decrease in anteroposterior diameter, alveoli less elastic and more fibrous. Decreased cough/gag reflects and mucous membranes are drier. More prone to aspiration and not able to expel secretions, higher risk for pneumonia

4
Accessory Muscles Trapezius Sternocleidomastoid Abdominal Muscles
Internal Intercostals Which muscles are used with inspiration and with expiration

5
History Tobacco use Coughing Chest pain Dyspnea
marijuana use- amount in pack years Pack years = # of years smoked x # of packs per day, age started and the number of efforts to quit Coughing: Onset (sudden, gradual, duration) - nature of cough: dry, wet, hacking, hoarse, barking , whooping, productive, non-productive - sputum characteristics: amount, color, odor - pattern of coughing: regular, related to weather, activities, talking, deep breaths -associated symptoms: SOB, Chestpain, tightness, fever, stuffy nose, choking, hoarseness Chestpain: onset,duration - associated symptoms: shallow breathing, fever, radiation - efforts to treat: heat, splinting, pain medication Dyspnea: onset, duration - pattern: position most comfortable, amount of pillows - related to activities, at rest, worse with inhalation or exhalation
 - nature of cough: dry, wet, hacking, hoarse, barking , whooping, productive, non-productive. - sputum characteristics: amount, color, odor. - pattern of coughing: regular, related to weather, activities, talking, deep breaths. -associated symptoms: SOB, Chestpain, tightness, fever, stuffy nose, choking, hoarseness. Chestpain: onset,duration. - associated symptoms: shallow breathing, fever, radiation. - efforts to treat: heat, splinting, pain medication. Dyspnea: onset, duration. - pattern: position most comfortable, amount of pillows. - related to activities, at rest, worse with inhalation or exhalation.")
6
History Orthopnea Paroxysmal nocturnal dyspnea (PND)
Activity tolerance Recurrent pneumonia or bronchitis Pollutants (asbestos, coal dust, chemicals, etc.) Passive smoking R/O risk for TB Employment Nutritional status: weight loss, weight gain Travel exposure Hobbies: noxious exposure from animals, woodworking
 Passive smoking. R/O risk for TB. Employment. Nutritional status: weight loss, weight gain. Travel exposure. Hobbies: noxious exposure from animals, woodworking.")
7
History Review family history Pneumonia or influenza vaccine
Date of last TB test Cystic fibrosis, emphysema. allergies

8
Physical Exam General assessment * Inspect facial expression
* Posture configuration of chest (AP -diameter should be 1/3-1/2 transverse diameter) * Respiratory rate and pattern * Inspect hands for clubbing Ratio of respiration's to heartbeats 1:4 Note the rhythm: regular, irregular and the way the chest moves, not too shallow or too deep Orthopnea: SOB when lying down Platypnea: dyspnea increases in the upright position Tachypnea: >20/min Bradypnea: < 12/min hypopnea: abnormal shallow with pleuritis Hyperpnea: rapid, deeply with increased WOB Kussmaul: deep and rapid, metabolic acidosis Cheyne -Stokes: regular with periods of apnea, followed by crescendo-decrescendo sequence Biot: somewhat irregular, varies in depth Cyanosis: lips, nasal flaring
 * Respiratory rate and pattern. * Inspect hands for clubbing. Ratio of respiration s to heartbeats 1:4. Note the rhythm: regular, irregular and the way the chest moves, not too. shallow or too deep. Orthopnea: SOB when lying down. Platypnea: dyspnea increases in the upright position. Tachypnea: >20/min. Bradypnea: < 12/min. hypopnea: abnormal shallow with pleuritis. Hyperpnea: rapid, deeply with increased WOB. Kussmaul: deep and rapid, metabolic acidosis. Cheyne -Stokes: regular with periods of apnea, followed by. crescendo-decrescendo sequence. Biot: somewhat irregular, varies in depth. Cyanosis: lips, nasal flaring.")
9
Physical Exam Sitting position for posterior and lateral
May sit or supine for anterior Undressed from waist up NEVER listen through clothing!!!!!!

10
Normal Adult

11
Scoliosis

12
Kyphosis

13
Barrel Chest

14
Pectus Excavatum

15
Pectus Carinatum

16
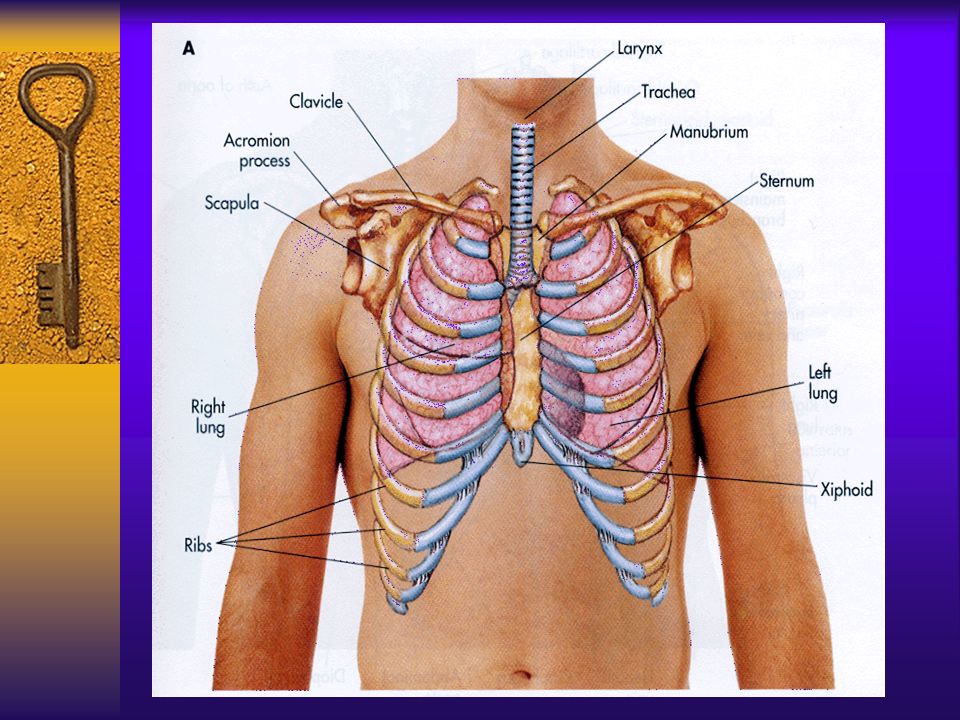
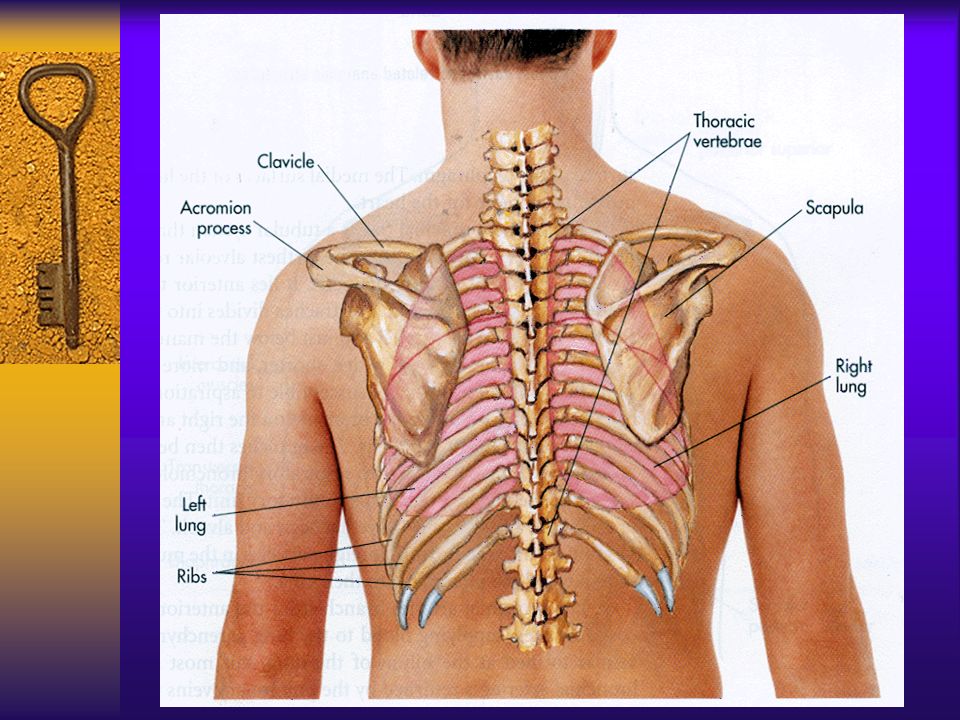
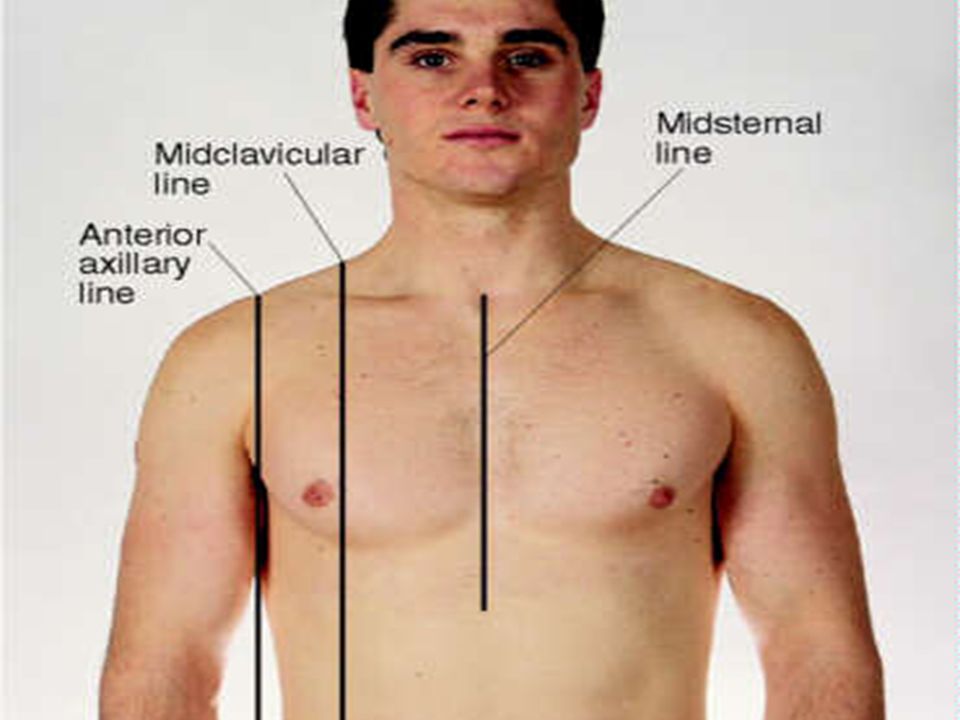
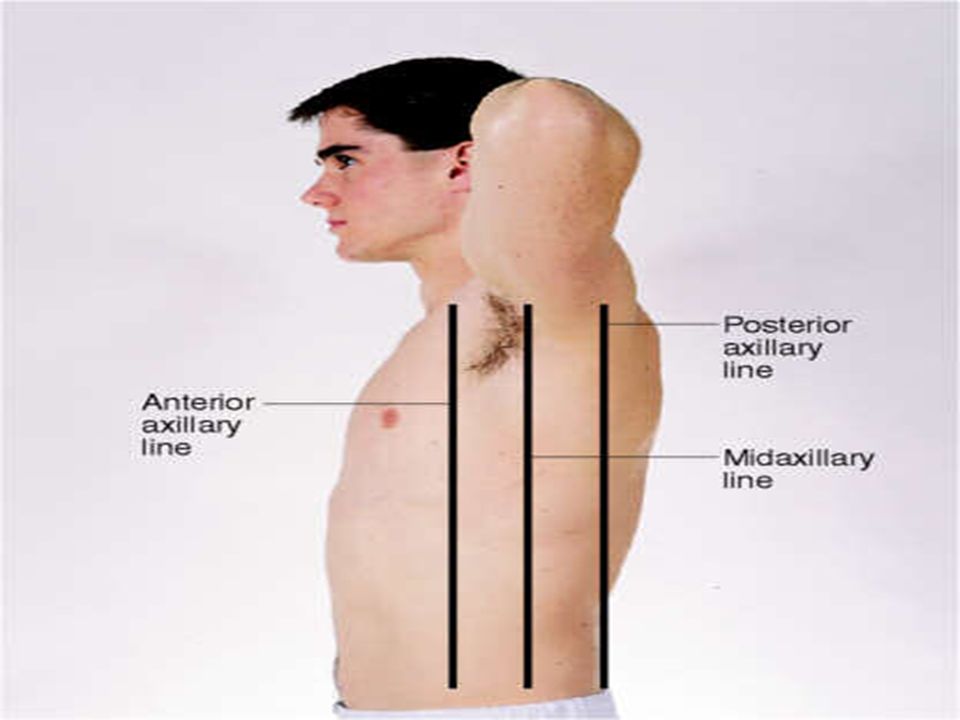
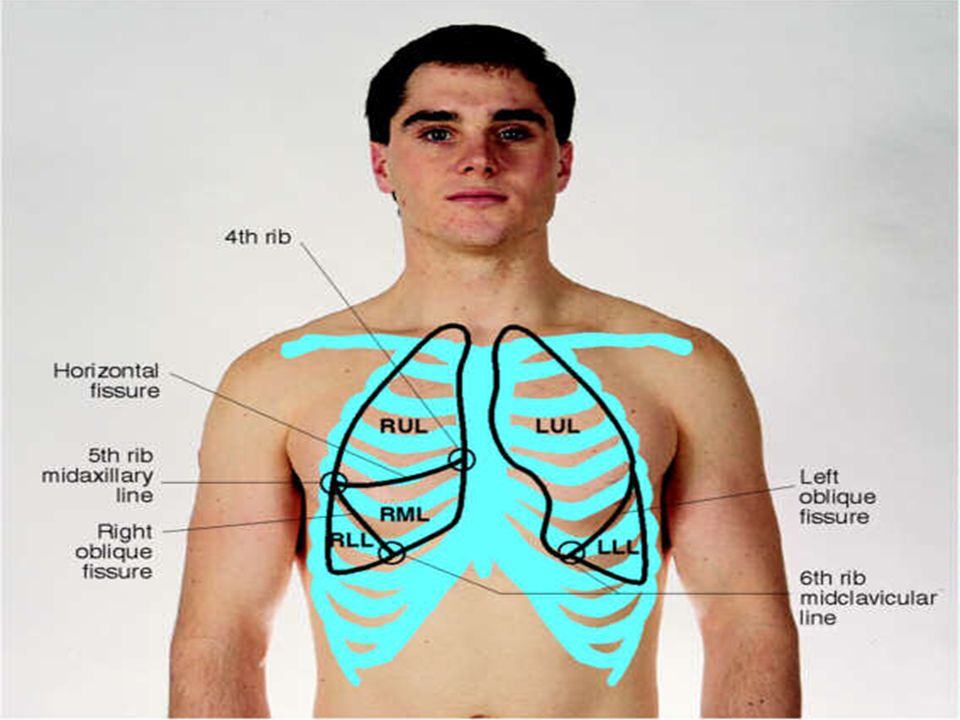
Landmarks of Clinical Importance
Sternum Clavicle Suprasternal notch Manubriosternal angle Midsternal line Midclavicular lines Anterior axillary lines Midaxillary lines Posterior axillary lines Scapular lines Vertebral line

25
Posterior Chest Palpate for any tenderness or abnormalities
Measure posterior chest excursion *Should be symmetrical Crepitus: crackly or crinkly sensation, bubbly feeling, indicates air in the subcutaneous tissue Pleural friction rub: palpable, coarse, grating vibration, mostly on inspiration, like leather rubbing over leather

26
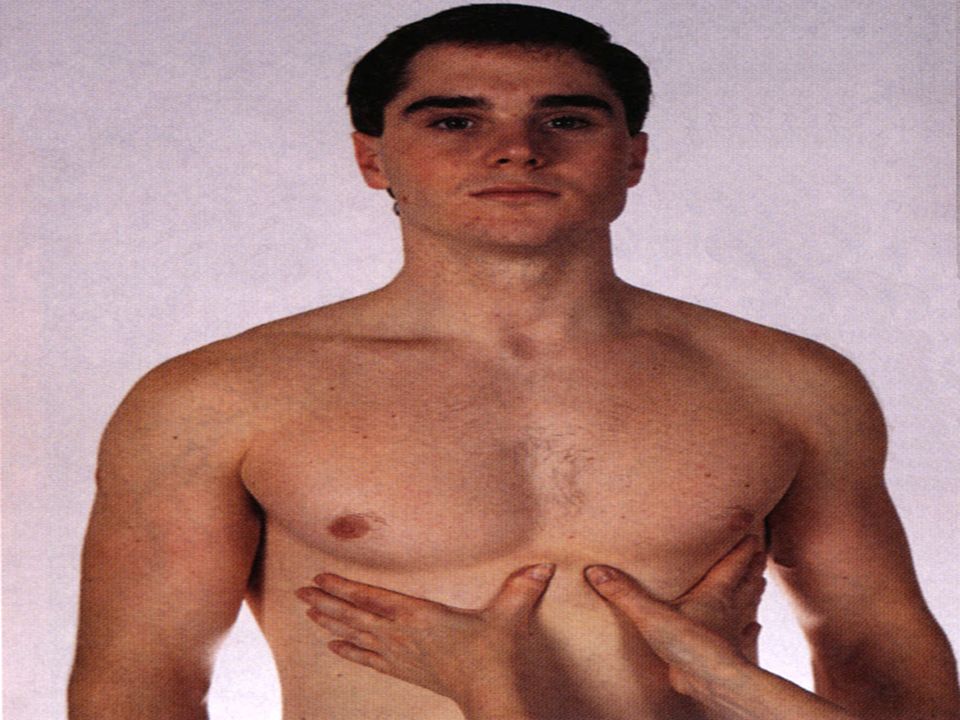
Thoracic expansion during respiration: watch and feel for symmetry,
watch the movement of your thumbs.

27
Posterior Chest Palpate for tactile fremitus
*Vibration of the chest wall during speech At each position ask the patient to say “99” If difficulty feeling, ask the patient to speak louder and deeper Decreased or absent fremitus: excess air as in emphysema, pleural effusion, massive pulmonary edema or bronchial obstruction. Increased fremitus: with fluids or solid mass within the lungs or with consolidation, heavy non-obstructing secretions

29
Tactile Fremitus Decreased fremitus is caused from excess air (emphysema, pneumothorax, atelectasis). Increased fremitus is caused by the presence of fluid or a mass.

30
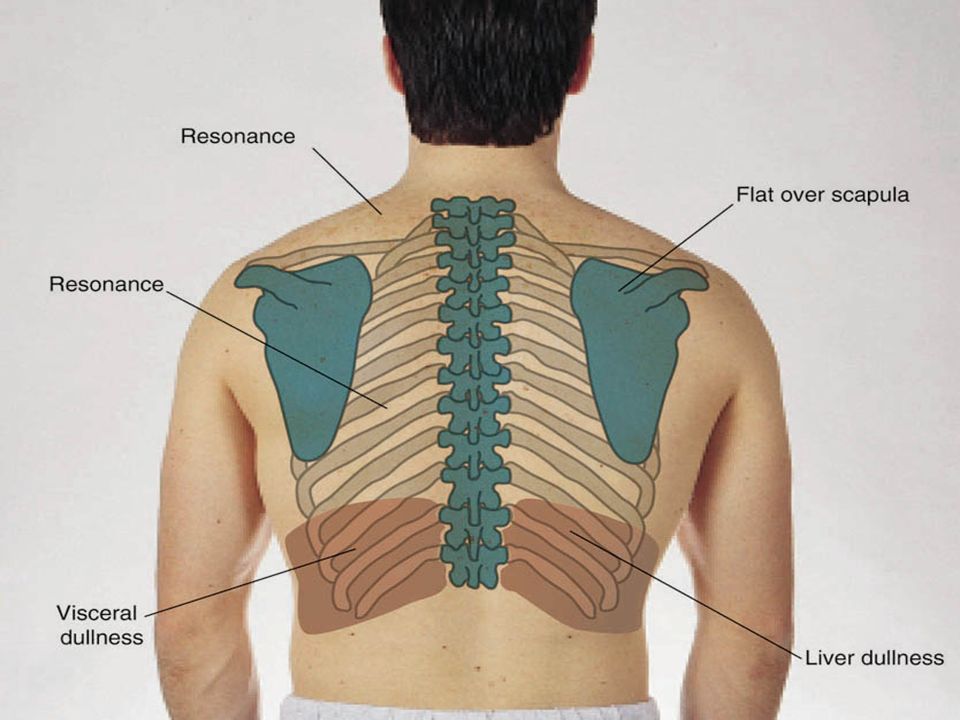
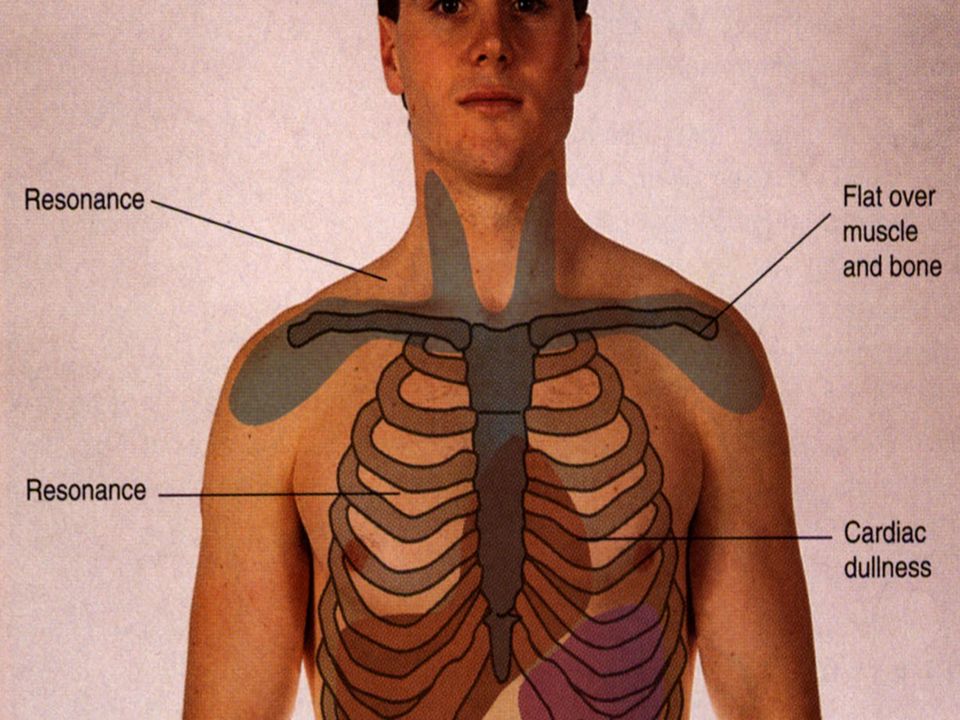
Posterior Chest Percussion- determine whether the lung tissue is air filled, fluid filled, or solid. Sounds of percussion * Resonant * Dull * Tympanic * Flat * Hyperresonant

33
Posterior Chest Measure diaphragmatic excursion
*Normal should be 3-5cm *The diaphragm is normally higher on the right. *Diaphragmatic descent may be limited by pulmonary lesions, abdominal lesions or pain.

34
1. Ask the patient to inhale deep and hold their breath
2. Percuss along the scapular line until you locate the lower border , mark the point were resonance turns into dullness 3. Ask the patient to take several deep breath, then exhale as much as possible 4. Percuss down from the marked point and again mark were resonance turns into dullness 5. Measure the distance between the marks

35
Posterior Chest Auscultation *Use diaphragm of stethoscope

36
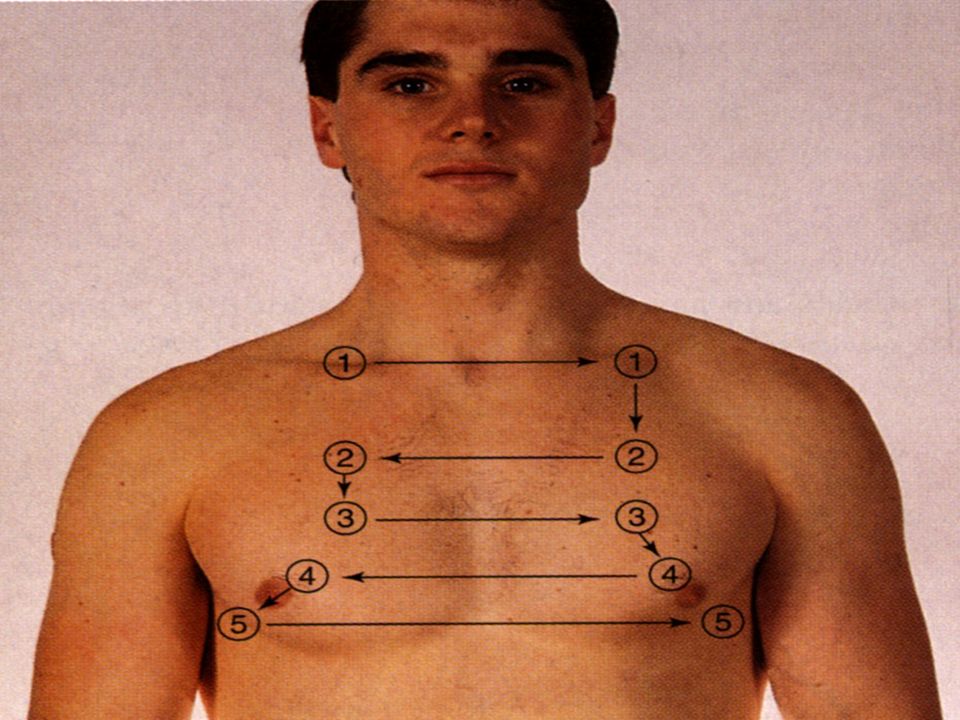
Explain arm position while auscultating, do not skip the lateral sides

37
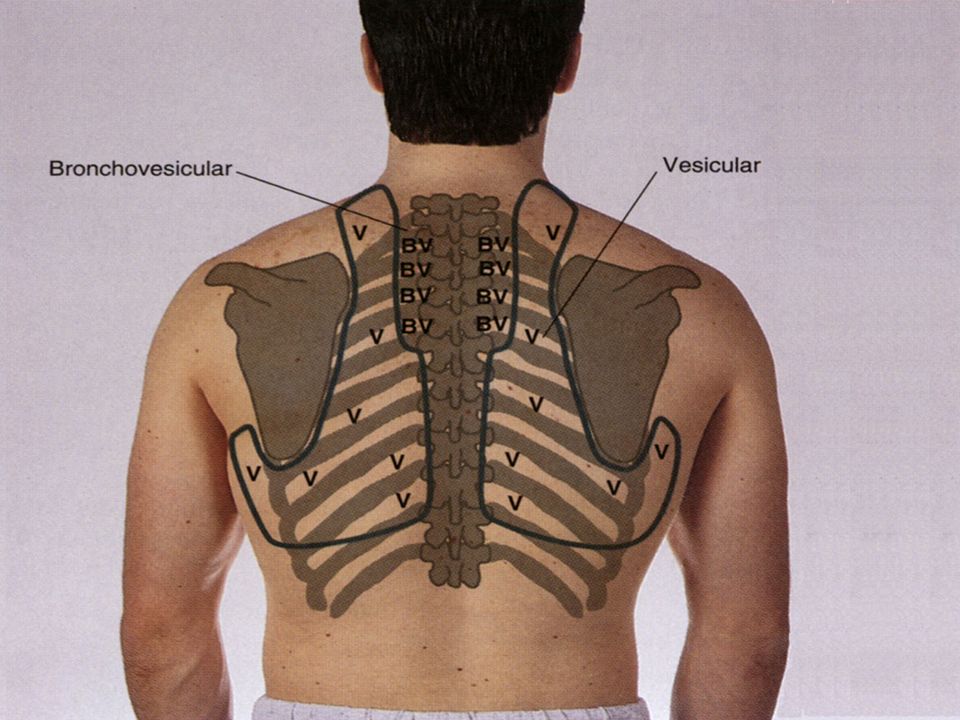
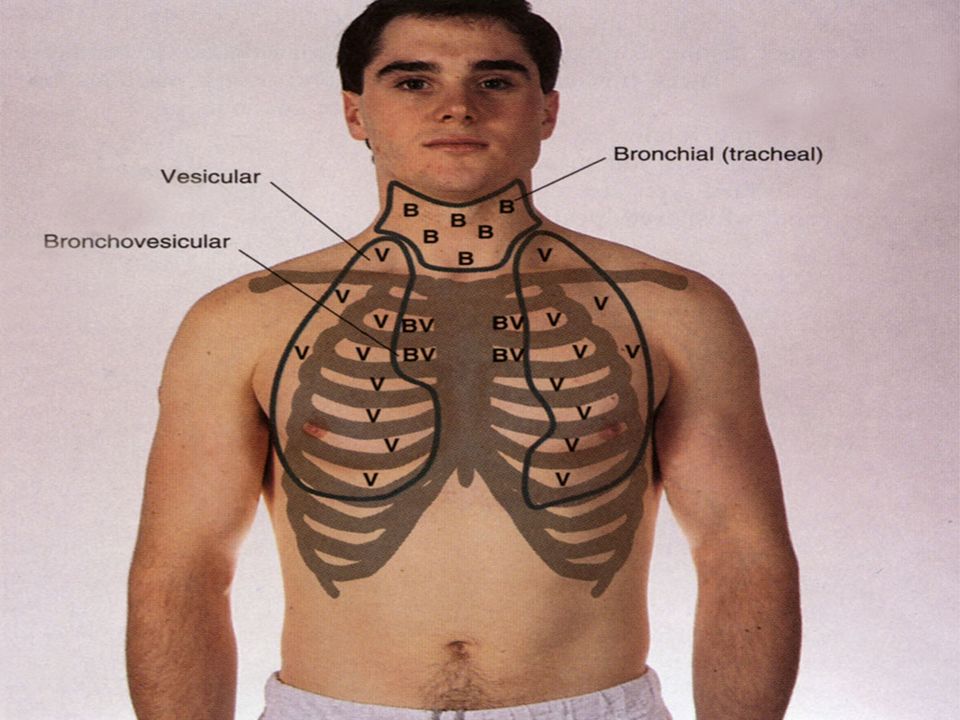
Types of Breath Sounds Bronchial: loud, high pitched.
Bronchovesicular: medium pitch. Vesicular: soft, low pitched. Bronchial- loud, high pitched. Heard over the trachea. I < E. Bronchovesicular- mixture of bronchial and vesicular. Medium pitch. Heard in the 1st and 2nd ICS anteriorly and between the scapula posteriorly. I = E. Vesicular- soft, low pitched. Heard over peripheral lung fields. I > E.

39
Additional Tests Abnormalities assessed in tactile fremitus, percussion, or auscultation Bronchophony- In same location as breath sounds say “99” or “eee”. *Normally sounds are muffled. Whispered pectoriloquy- In same location as breath sounds whisper “99”. *Whispered voice should be faint.

40
Lateral Chest Same as posterior chest, may perform along with posterior chest.

41
Anterior Chest Inspection Chest excursion Evaluate tactile fremitus

44
Anterior Chest Percussion Auscultation

48
Adventitious Breath Sounds
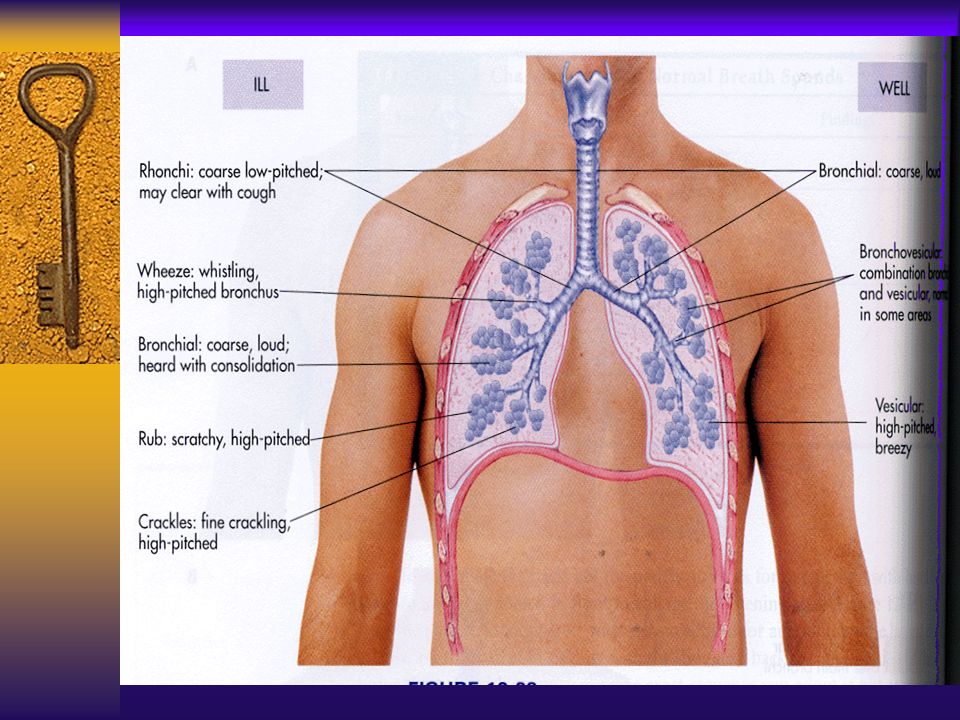
Crackles: Fine Crackles Medium Crackles Coarse Crackles Crackles- mostly heard in the dependant lobes. Caused by opening of collapsed distal airways. Fine crackles- high pitched, fine. Heard at the end of inspiration. Not cleared by coughing. Medium crackles- lower pitched, more moist. Heard during the middle of inspiration. Not cleared with coughing. Coarse crackles- loud, bubbly sounds. Heard during inspiration. Not cleared with coughing.

49
Adventitious Breath Sounds
Rhonchi Wheezes Pleural Friction Rub Rhonchi- Primarily heard over the trachea and bronchi. Due to fluid or mucus in the larger airways. Low-pitched, course sounds. Heard during inspiration and expiration May be cleared with coughing. Wheezes- Can be heard over all lung fields. Airflow through narrowed bronchus. High-pitched, musical sounds. Heard during inspiration and expiration Pleural friction rub- Heard over anterior lateral lung field. Due to inflamed pleura. Has dry, grating quality. Does not clear with coughing.

50
Order of the Physical Exam
Posterior Chest: Inspection - Palpation - Chest Excursion - Tactile Fremitus - Percussion - Diaphragmatic Excursion - Auscultation

51
Order of the Physical Exam
Lateral Chest: Inspection Palpation Tactile Fremitus Percussion Auscultation

52
Order of the Physical Exam
Anterior Chest: Inspection Palpation Chest Excursion Tactile Fremitus Percussion Auscultation

53
Adventitious Breath Sounds
Rhonchi: Primarily heard over the trachea and bronchi. Rhonchi: Primarily heard over the trachea and bronchi. Due to fluid or mucus in the larger airways. Low pitched , course sounds Heard during inspiration and expiration May Clear with coughing

54
Adventitious Breath Sound
Wheezes Wheezes: Can be heard over all lung fields Airflow through narrowed bronchus High-pitched musical sounds. Heard during inspiration and expiration

55
Adventitious Breath Sounds
Pleural Friction Rub Pleural Friction Rub Heard over anterior lateral lung field Due to inflammation in pleura Dry, grating quality Does NOT clear with coughing

Similar presentations
























. Associated symptoms.>")
