Download presentation
Presentation is loading. Please wait.

1
Respiratory System Dr. Muhammad Atif Qureshi Associate Professor Department of Medicine

2
A 45 years old male presented with one year history of: Recurrent chest infections Fever Cough and expectoration

3
17 year old female presented with 3 months history of: Weight loss Cough with expectoration Fever Night sweats

4
60 years old male Chronic chain smoker Weight loss Cough Hemoptysis

5
Chest Pain 1.Onset 2.Severity 3.Site 4.Character 5.Nature 6.Aggravating factors 7.Relieving factor 8.Radiation 9.Referred pain 10.Associated complaints

6
Cough 1.Onset 2.Severity 3.Character 4.Aggravating factors 5.Relieving factor 6.Associated complaints 7.Hemoptysis

7
Other presenting symptoms – Apnea – Hoarseness – Stridor – Snoring – Fever – Night sweating – Weight loss

8
General physical examination Related to Respiratory system

9
Vital signs General appearance Hands – Tremers – Nicotine stains – Clubbing – Koilonychia – Pallor – Cyanosis – Palmar erythema Use of accessory muscles of respiration Lymph nodes

10
Hands examination Central Cyanosis – COPD, Asthma – Pulmonary fibrosis – Pneumonia, PE – A/V malformation – Cardiac Rt to Lt shunts Peripheral cyanosis – Cold weather – Low COP

11
Clubbing – Bronchiectasis – Ca lung – Lung abscess – Pulmonary fibrosis – Asbestosis – Cystic fibrosis

13
Hypertrophic pulmonary osteoarthropathy – Carcinoma lung

14
Tremors – FineB2 agonist – FlappingCO2 retention

15
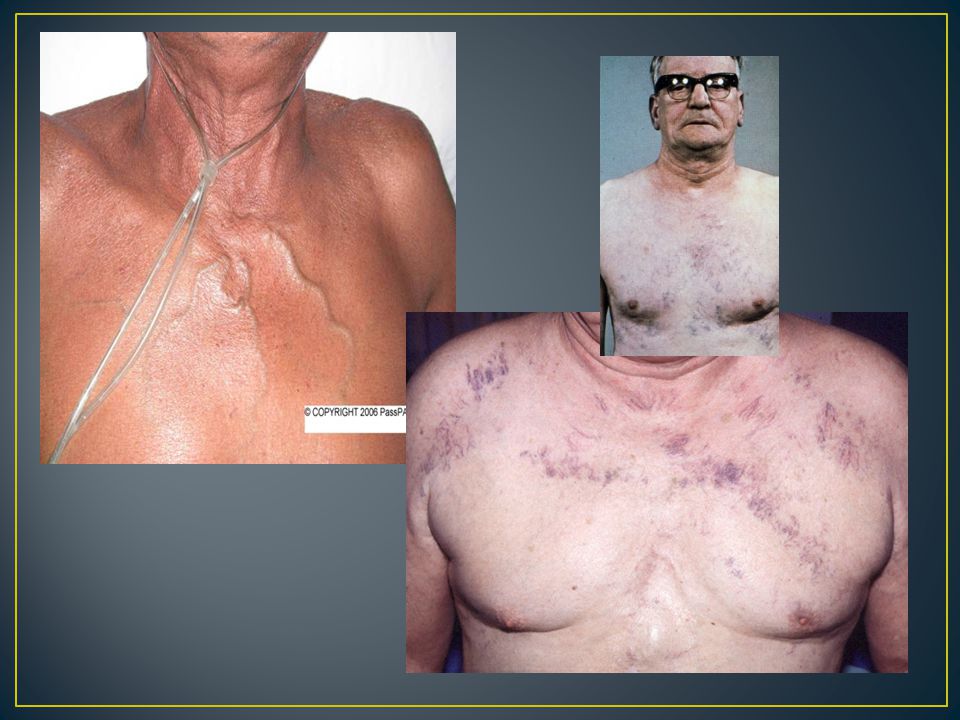
Inspection: 1.Shape: AP diameter compared to transverse (barrel-chest), pectus excavatum, pectus carinatum, kyphoscoliosis,…. others 2.Symmetry: assessment of upper & lower lobes should be done posteriorly looking for ↓ or delayed chest movement during moderate respirat’n. 3.Scars: from previous operat’n or chest drains or cautery marks or radiotherapy markings. 4.Prominent veins: in case of SVC obstruct’n

31
1.Trachea: normally central, slight Rt displacement could be N. Check for gross displacement. Tracheal tug means the N distance bet sternal notch & cricoid cartilage is < 3-4 finger breadths & occurs in chest overexpansion as copd. 2.Apex beat : Check for displacement. 3.Chest expansion : N expansion ≥ 5cm 4.Tactile vocal fremitus (TVF): can be done with the palm of one hand.
: can be done with the palm of one hand..")
36
Should be done symmetrically (Lt compared with the Rt), posteriorly (the back), anteriorly (the front) & laterally (the sides). Supraclavicular area, then clavicles should be percussed directly to evaluate the upper lobes. Liver dullness: of the upper edge starting at the 5 th rib MCL, resonant note below this area indicates hyper- inflation (copd, severe asthma) Cardiac dullness: may be ↓ in hyperinfated chest.
 Cardiac dullness: may be ↓ in hyperinfated chest..")
38
Using the diaphragm of a stethoscope & comment on the following: 1.Breath sounds (BS): Intensity: N or ↓ as in (consolidation, collapse, pl effusion, pneumothorax, lung fibrosis) Quality: Vesicular or bronchial in consolidation Differentiation between vesicular & bronchial BS: Vesicular: louder &longer on inspiration than expiratory phase & has no gap between the 2 phases Bronchial: louder &longer on exp phase & has a gap between the 2 phases
: Intensity: N or ↓ as in (consolidation, collapse, pl effusion, pneumothorax, lung fibrosis) Quality: Vesicular or bronchial in consolidation Differentiation between vesicular & bronchial BS: Vesicular: louder &longer on inspiration than expiratory phase & has no gap between the 2 phases Bronchial: louder &longer on exp phase & has a gap between the 2 phases")
39
Type: Wheezes or Crackles or friction rub Timing: inspiratory or expiratory WHEEZES: are continuous musical polyphonic sound, heard louder on expiration & can be heard on inspiration which may imply severe AW narrowing. High pitched- wheezes are found in BA due to acute/chronic airflow limitation & low pitched in COPD. Localized monophonic wheeze due to fixed AW obstruct’n in CA bronchus. CRACKLES: interrupted non-musical inspiratory sound coarse medium fine Crackles may be early, late or pan-inspiratory & fine, medium or coarse. Ex: late/pan-insp coarse crackles in bronchiectasis, late/pan-insp medium crackles in pul edema, late/pan-insp fine crackles in pul fibrosis

40
It’s due to thickened or roughened pleural surfaces rub together as lungs expand & contract & give off a continuous or intermittent grating sound. It indicates pleurisy & may be heard in pneumonia or pulmonary infarction. VOCAL RESONANCE: It’s the ability to transmit sounds. Ask patients to say 123 (Urdu) or 99 (English) & listen for the transmitted sound which may be ↓ or ↑ or N (low pitched component of speech heard with booming & high pitched become attenuated).
 or 99 (English) & listen for the transmitted sound which may be ↓ or ↑ or N (low pitched component of speech heard with booming & high pitched become attenuated)..")
42
Thank You

Similar presentations